
Abstract
Aim:
To assess parents’ ability to express their concerns and hopes for the future in their children with disability and assess their children’s disability as well as to analyse these data for consistency.
Method:
Parents of 162 children with spina bifida, spinal muscular atrophy, muscular disorders, cerebral palsy, visual impairment, hearing impairment, mental disability, or disability following brain tumours were asked to freely express their concerns and hopes for the future and to assess disability in their own children by employing a set of 26 International Classification of Functioning, Disability and Health, Children and Youth Version (ICF-CY) body function (b) codes and activity and participation (d) codes. A grounded theory approach was employed to systematize parents’ expressions of concerns and hopes; then, parents scored qualifiers on a 5-step qualitative Likert scale. Parents assessed their children’s disability in the same way using the ICF-CY 5-step qualifier scale.
Results:
Altogether, 119 parents freely expressed their concerns and hopes, and 101 of them also assessed their children’s disability using the 26 ICF-CY codes. A total of 475 expressions of concern and hopes (issues) were expressed and categorized into 34 areas of concern and hopes (subsections). The most frequently mentioned issues were education; understanding, goodwill, and communication between parents; and community support. Qualitative data on both 5-step qualifier scales showed good reliability. Rasch analysis maps on concerns and hopes for children as well as on the ICF-CY assessment demonstrated good alignment and a clinically relevant progression from the least to the most disabled children.
Conclusion:
Parents can express valid and reliable data on their concerns and hopes for the future and can reliably assess disability in their own children.
Keywords
Introduction
Children with disabilities are followed clinically by us throughout their childhood and youth. In this setting, parents very often express their concerns and hopes for the future, which are very often expressed on behalf of their children. These families’ life conditions as well as help and support from the society around them are in frequent focus.
From other studies, we know how parents care for their children with disabilities, health care, and concerns and hopes for the future are interrelated and may affect each other. Three areas of importance are as follows.
First, parents seek qualitative and inclusive care for their children with disabilities, and this implies understanding of family needs.1–3 Such care includes social support with coping strategies to reduce parental stress. 4 Parents should be fully involved in decisions on behalf of their children’s health and social care, and furthermore they should be able to avoid the need to fight for their children. 5
Second, hope may be experienced and expressed in different terms according to different circumstances. Thus, hope is strongly correlated to cure, as well as to the idea that the child will feel loved and that the parents will always do the best for their child. 6 Hope is related to quality of life, the physical body, future well-being, future health, and medical care and may relate to a broader meaning of a child’s illness.6–10 It is important for health care professionals to support families by partnering with parents. 11 Parents in turn are supported by hope as they care for their children 12 and as they adapt to living with in caring for a child with a disability. 13 Hope may help parents find a way to rediscover their children with disabilities. 14 Hope may also be gained when there is uncertainty about a diagnosis or when parents encounter challenges in daily life or planning for the future. 15 Hope may change over time. 7
Third, clinicians may be hesitant to discuss the severity of children’s disabilities and prognostic issues with parents in clinical settings because of their fear of how the parents will respond to such information. This occurs when children are critically ill 16 but mainly also apply in other situations when dealing with severe disabilities and related hopes and concerns for the future. At minimum, communication and partnership with parents should be honest and informed to continuously nurture hope. 11
From 2011 onward, we had the privilege of repeated contact with Danish parents of a population of 332 children with 8 disabilities ranging in severity from mild to severe. We conducted interviews and forwarded questionnaires to obtain parents’ assessments of disability in their children and assess the feasibility of applying parts of the World Health Organization (WHO) International Classification of Functioning, Disability and Health, Children and Youth Version (ICF-CY) coding system 17 to parents of this population of children. 18 We found that the parents’ assessments are valid and that the set of codes related to everyday living functions well and is stable when repeated. 18
We then invited these parents to take 1 step further to freely express their concerns about and hopes for the future of their children with disabilities. At the same time, we again asked them to assess the severity of their children’s disabilities by scoring an identical set of ICF-CY codes to the one previously used. 18 We employed a grounded theory approach to analyse their freely expressed hopes and concerns.
The purpose of this seemingly novel approach was first to hear the hopes and concerns the parents expressed and the importance they personally attached to these issues. Second, the extent to which the parents’ assessment of the severity of their children’s disability was aligned with their individual hopes and concerns for the future of their children would become clearer and more understandable. And to compare these unique sets of qualitative information the best possible way by converting to quantitative data sets for alignment. To that end, we employed Rasch analysis methods.
Methods
Children with disability
We started dialogues with the parents of 332 children with disabilities in 2011 by visiting them in their homes. We wanted to apply the WHO ICF-CY model to descriptions of disabilities in each child by applying body functions (b codes) and activities and participation in daily living (d codes). In 2015, we again contacted 263 of the original 332 parents by post to assess reliability and validity when scoring their children according to 26 selected and joined b and d codes. Six months later, we used by post to contact the 162 parents who responded to invite them to freely express their concerns about the future of their children and score their children with identical codes once again.
Parents’ expressed concerns and future hopes
A grounded theory approach was employed in which parents were encouraged in writing to freely express their thoughts, concerns, and reflections on their children’s near and farther future, both in positive and more concerned terms. They were not given any guidelines or examples.
When each parent’s written text was received, both the social worker (M.B.) and the child neurologist (N.O.I.) independently read the parents’ thoughts and sorted them into freely expressed issues based on their individual understandings of the text’s meaning. These issues were then grouped into meaningful sections.
Then, M.B. and N.O.I. met and discussed the meaning of the parents’ expressions and issues, the sections, and the wording of the sections. The aim was to give as detailed a picture as possible of the parents’ concerns.
This final list of sections and issues was forwarded to the parents in written format, and the parents were asked to score the sections and one or more common issues that were listed in each section.
For scoring, a 5-step Likert scale was employed, and the parents had the opportunity to express one of the following responses:
1: No common hopes and concerns;
2: Slightly common hopes and concerns;
3: Some common hopes and concerns;
4: Considerably common hopes and concerns;
5: Very considerably common hopes and concerns.
The parents were also asked to assess disability in their own children by employing the 26 ICF-CY joined body function (b codes) and activity and participation (d codes) codes mentioned below. The parents knew these codes beforehand.
ICF-CY codes
Each of the 26 selected and combined b and d codes were topics related to daily living from early morning until night (Table 1), and the qualifiers were worded in the same way as they had been previously 3 and scored by the parents as follows:
1: The child’s ability is as expected for his or her age.
2: The child has difficulties but is still functioning in the expected range for his or her age.
3: The child needs help from another person with functions, activities, and participation.
4: The child needs help and care; the child has only limited ability with respect to body functions, activities, and participation.
5: The child is totally dependent on others for body functions, activities, and participation.
The 26 ICF-CY codes selected were all second level out of 4 codes: They are listed here in the order they were presented in the questionnaire.

Abbreviation: ICF-CY, International Classification of Functioning, Disability and Health, Children and Youth Version.
Supplementary wording was provided to help the parents understand the meaning of the codes.
Psychometric analysis of hopes and concerns as well as ICF-CY code data
Both data sets were analysed for coherence by employing psychometric and Rasch analyses, and the data were compared for correlation between parents’ assessments of disability severity and concerns for their children’s futures.
Data targeting was estimated from the code scale’s midpoint, the range, and the observed scores with floor and ceiling effects. The reliability was estimated using Cronbach’s α coefficient, inter-code correlation, standard error, and standard error of measurement (SEM). The validity was estimated with corrected code-total correlations and Cronbach’s α: α = N ×
Rasch modelling on hopes and concerns as well as ICF-CY code data
The Rasch model defines an individual’s probability of success (P) on a given item in terms of the difference between the individual’s disability (B) and the item difficulty (D): P = exp(B − D)/1 + exp(B − D) or logP/(1 − P) = B − D. The probability of success P can also be expressed as log(odds) = B − D or logit = B − D.
Rasch analysis was applied to all 5 qualifiers for the scale expressions regarding future hopes and concerns as well as the selected ICF-CY b and d codes. In practice, when a child’s level of disability is equal to a certain qualifier level, B and D are identical, and the derived log(odds) or logit value will be 0. For codes at which the level of hopes and concerns for the child or the child’s disability level is higher or lower, the relevant logit value will be positive or negative, respectively.4–8 A logit scale constitutes the latent construct or variable (also called the measure in Rasch terminology) for the parents’ hopes and concerns qualifiers as well as the 26 joined ICF-CY b and d codes.
There were 5 hopes and concerns qualifiers and 5 ICF-CY code qualifiers; thus, 4 Rasch-Andrich thresholds were defined, with each threshold indicating equal probabilities of hopes and concerns or disability levels between 2 adjacent expressed qualifiers. The thresholds are denoted as τ1, τ2, τ3, and τ4.
Fit is denoted if the data conform to the Rasch model. Fit is expressed in terms of mean squared values as infit mean-squared values (MNSQ) and outfit MNSQ. An infit MNSQ close to 1 indicates that the data are reliable (not assessed randomly), while an outfit MNSQ close to 1 signifies that the results are not at odds with the overall set of data.
Winsteps 3.74.0 was used to perform the Rasch measurements. 8
Analysis of correlation
Both the concerns and hopes for the future scale and the assessment of disability scale are Likert scales of qualitative data and are therefore not directly comparable. As Rasch analysis converts qualitative data into quantitative and thus comparable data, measures were employed for correlation. Correlation factor R was computed for the obtained measures and presented graphically.
Results
Children with disabilities
Out of 162 questionnaires sent to the parents, 119 (73.5%) were returned. Among those, 101 also contained ICF-CY codes. The 119 children had spina bifida (26), spinal muscular atrophy (7), muscular disorders (14), cerebral palsy (44), visual impairment (4), hearing impairment (4), mental disability (5), or disabilities following treatment for brain tumours (15). Their mean age was 13.9 years (range = 7-18 years), and 57 (47.8%) were girls.
Parents’ expressed concerns and future hopes
The social worker (M.B.) identified 220 issues formulated by parents, and the child neurologist (N.O.I.) identified 254 issues. The material was not saturated. In total, 15 sections were identified.
After bilateral discussion about each issue and the sections, a total of 474 issues were formed. The number of sections was reduced from 15 to 14, and 34 subsections were created; 79 issues changed sections (Table 2).
Parents’ common issues, concerns, and future hopes: In total, 119 parents answered this questionnaire.
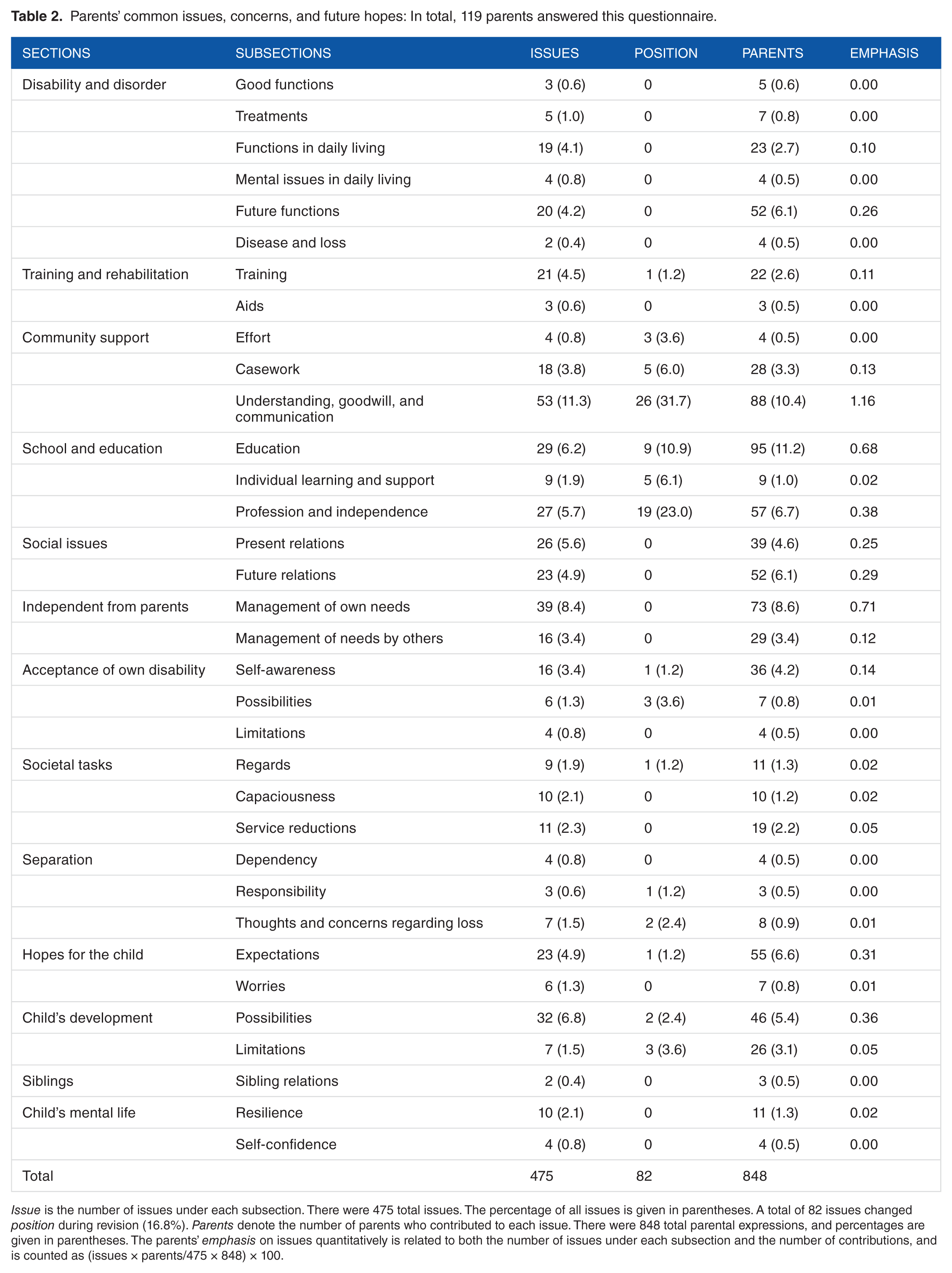
Issue is the number of issues under each subsection. There were 475 total issues. The percentage of all issues is given in parentheses. A total of 82 issues changed position during revision (16.8%). Parents denote the number of parents who contributed to each issue. There were 848 total parental expressions, and percentages are given in parentheses. The parents’ emphasis on issues quantitatively is related to both the number of issues under each subsection and the number of contributions, and is counted as (issues × parents/475 × 848) × 100.
The final questionnaire, with its 475 common issues sorted into 14 sections and 34 subsections, was forwarded to the parents, together with the ICF-CY questionnaire on 26 codes related to disability. The parents emphasized certain issues both by producing a high number of related issues and by scoring the issues. The most predominantly expressed issues were those related to education, understanding, goodwill, and communication (Table 2).
The 2 most frequently expressed hopes and concerns within each subsection are presented in Table 3.
Parents’ common issues regarding concerns and future hopes: Two representative examples are mentioned for each common issue to illustrate parents’ thoughts and concerns.

The sentences have been shortened due to space concerns.
ICF-CY codes
To obtain close and time-related relationships between both scores, parents scored their children’s disabilities on the 26 combined b and d code ICF-CY qualifiers at the same time as when they scored the qualifiers for their future hopes and concerns.
Psychometric analysis of hopes and concerns issues and ICF-CY code data
The ICF-CY code data from all 101 questionnaires and the corresponding 101 questionnaires on hopes and concerns underwent identical psychometric analyses. The data were coherent and reliable, with corrected code-total correlations of 0.58 for hopes and concerns and 0.74 for ICF-CY code scores. The inter-code correlation was 0.35 and 0.57, and Cronbach’s α was 0.95 and 0.97 for the hopes and concerns data and ICF-CY code data, respectively (Table 4).
Qualitative analyses of data sets on concerns and future hopes and on ICF-CY codes, respectively: There were 34 sections containing common issues regarding future concerns.
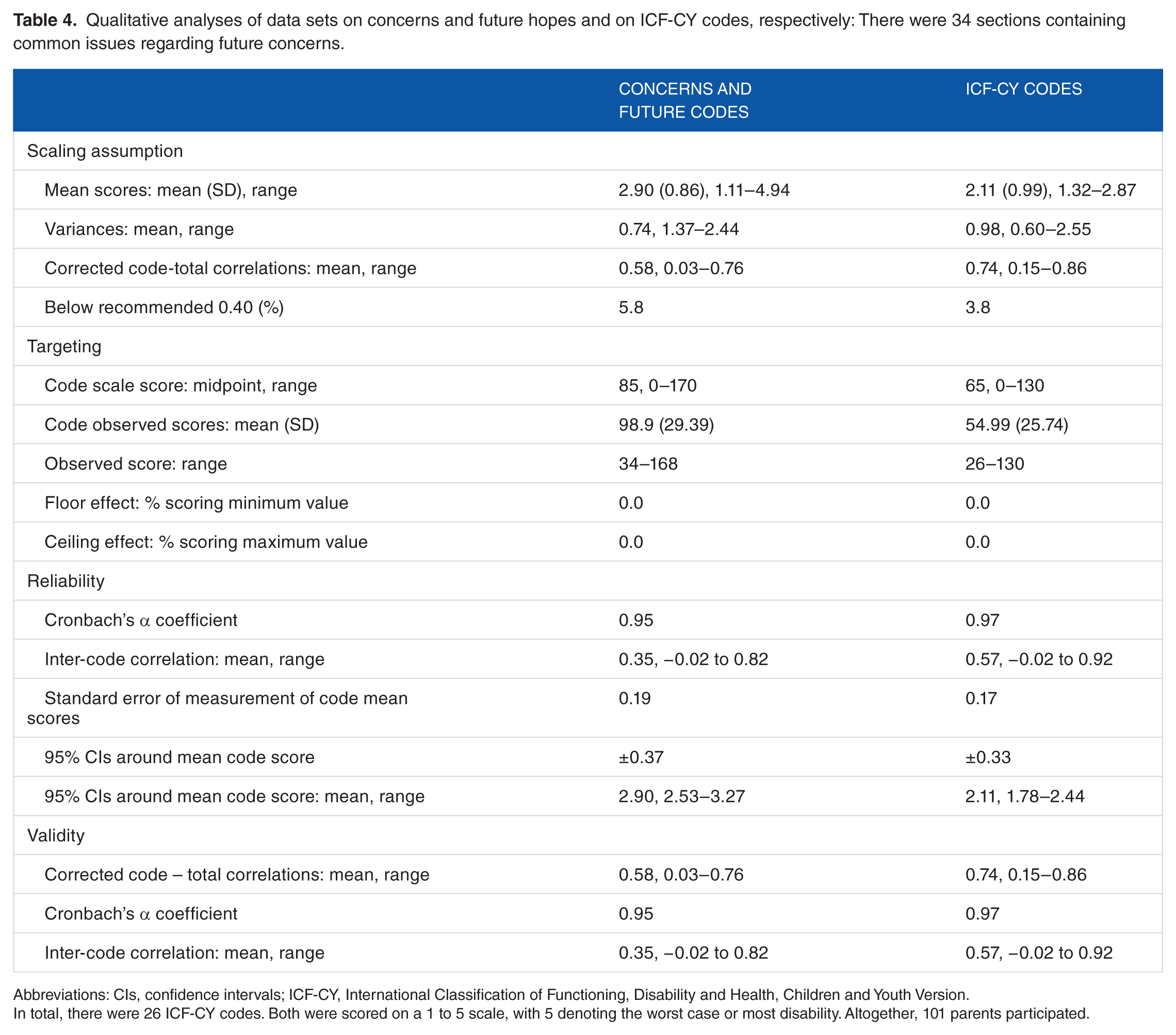
Abbreviations: CIs, confidence intervals; ICF-CY, International Classification of Functioning, Disability and Health, Children and Youth Version.
In total, there were 26 ICF-CY codes. Both were scored on a 1 to 5 scale, with 5 denoting the worst case or most disability. Altogether, 101 parents participated.
Rasch modelling on hopes and concerns issues and ICF-CY code data
All of the questionnaires on hopes and concerns and the corresponding questionnaires on ICF-CY code data underwent Rasch analysis. The average measures were around 0, and the infit and outfit MNSQs were around 1 (Table 5). However, the item ‘good functions’ had a high infit MNSQ of 2.33 and a high outfit MNSQ of 4.07, indicating that the item was difficult for the parents to comprehend or too general in meaning. Regarding the ICF-CY code scores, the same may have been true for d310 ‘receiving spoken messages’, for which the infit MNSQ was 3.16 and the outfit MNSQ was 8.64.
Rasch measure data on 26 joined ICF-CY codes and 34 codes on concerns about and hopes for the future: The measure expresses the most severe disability and most common hopes and concerns as positive and the least severe disability and least common hopes and concerns as negative.

Abbreviation: ICF-CY, International Classification of Functioning, Disability and Health, Children and Youth Version.
The average measure should be close to 0. Infit and outfit MNSQ represent conformity to the Rasch model and should be close to 1. The children who were the subject of disability scoring and hopes and concerns scoring should also represent a continuum of disability. This is likewise indicated by proper infit and outfit data. Each step represented in the two 5-point qualifier scales used here should have proper distance between each step, without overlapping. This is indicated by the tau (τ) values.
The τ values demonstrated no overlapping between qualifiers; however, the τ values for ICF-CY code qualifiers 4 and 5 were closely aligned, indicating that differentiating between code qualifiers 4 and 5 might have been problematic for the parents (Table 5).
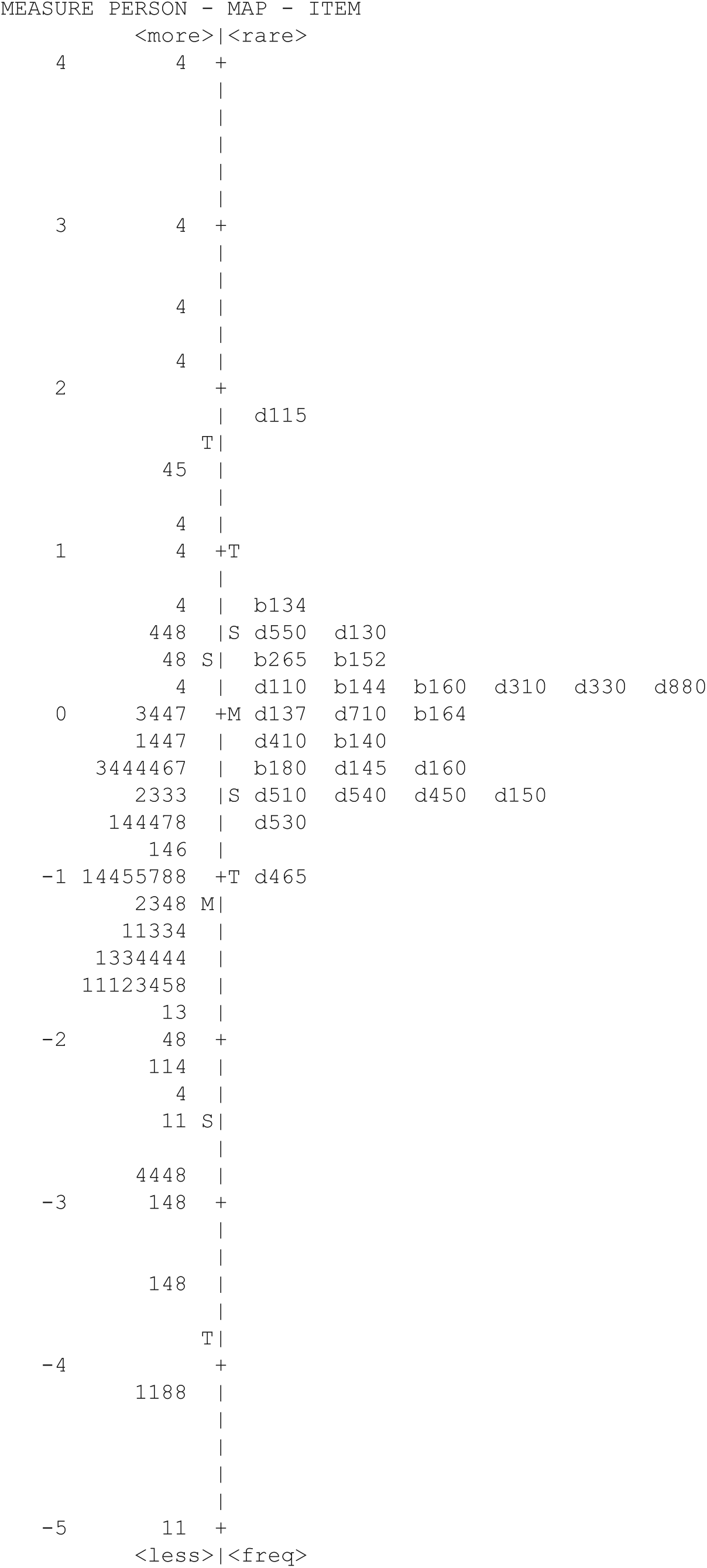
Considering the measure data demonstrated in the Rasch map of children’s futures and concerns about their children, parents who scored the specific subsections weighted concerns about ‘aids’ highest, particularly those whose children had the most severe disabilities related to spina bifida, spinal muscular atrophies, muscular disorder, cerebral palsy and disability following brain tumour. However, ‘expectations’ for the children were also expressed among parents of children with less severe disabilities (Figure 1).

Child and concerns and future hopes map for 101 parents: Each digit in the left column represents 1 child. M equals mean, S represents 1 SD and T represents 2 SDs. Each bar represents an interval on the measure scale of .12. The different numbers refer to (number) 1: spina bifida (21), 2: spinal muscular atrophy (3), 3: muscular disorders (12), 4: cerebral palsy (41), 5: visual impairment (4), 6: hearing impairment (2), 7: mental disability (5), and 8: disabilities following treatment for brain tumours (13). The right column constitutes future concerns represented by 34 subsections: good functions (goodf), treatments (treat), functions in daily living (fundl), mental issues in daily living (mendl), future functions (futuf), disease and loss (disel), training (train), aids (aids), effort (effor), casework (casew), understanding, goodwill, and communication (undgc), education (educa), individual learning and support (indls), profession and independency (profi), present relations (presr), future relations (futur), management of own needs (manan), management of needs by others (manno), self-awareness of own disability (selfa), possibilities for own disability (possi), restrictions for own disability (restr), regards (regar), capaciousness (capac), service reductions (servr), dependency (depen), responsibility (respo), thoughts and concerns regarding loss (thocl), expectations (expec), worries (worri), possibilities (possi), limitations (limit), sibling relations (siblr), resilience (resili), and self-confidence (selfc).
When dealing with ICF-CY code scores, d115 (‘listening’) was naturally scored highest among parents of children with severe disabilities related to cerebral palsy, as was d465 (‘moving around using equipment’) among parents of children with the least severe disabilities in all categories of disorders (Figure 2).
Child and disability map for 101 parents: Each digit in the left column represents 1 child. M equals mean, S represents 1 SD and T represents 2 SDs. Each bar represents an interval on the measure scale of .12. Different numbers refer to (number) 1: spina bifida (21), 2: spinal muscular atrophy (3), 3: muscular disorders (12), 4: cerebral palsy (41), 5: visual impairment (4), 6: hearing impairment (2), 7: mental disability (5), and 8: disabilities following treatment for brain tumours (13). ICF-CY codes are located in the right column. See Table 1 for further detail on the meaning of the codes. ICF-CY indicates International Classification of Functioning, Disability and Health, Children and Youth Version.
Analysis of correlation
The correlation between the 101 measures of hopes and concerns and the 101 measures of ICF-CY codes demonstrated an R value of .36 and a considerable spread in the measure data (Figure 3).
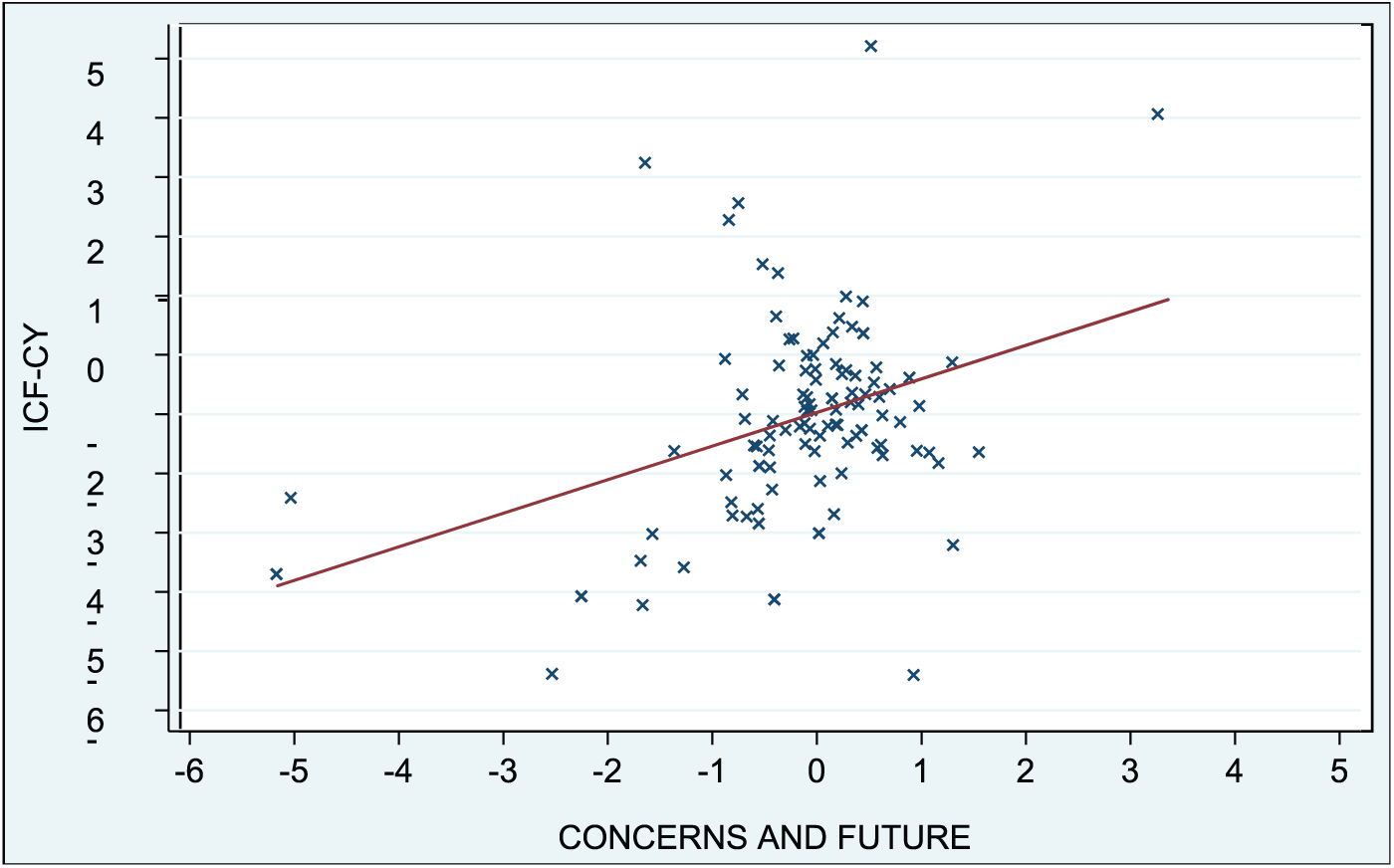
Correlation of Rasch measure between concerns and future data (X-axis) and ICF-CY code data (Y-axis). The correlation R is .36. ICF-CY indicates International Classification of Functioning, Disability and Health, Children and Youth Version.
Discussion
In recent years, care for children with disabilities and their families has become a focus of daily clinical practice. In particular, interventions and support to the whole family are important and can positively affect a family and a child’s quality of life.1–5 The ‘F-words’ – function, family, fitness, fun, friends and future – illustrate the importance of support tailored to each individual family and child.19–23
Because support for children and families is crucial to their present daily living and their future, we wanted to find ways to improve relationships between families and services to connect them, the hospital setting and health services in the community. This included providing ways for parents to identify disability in their own children and thus enter into a dialogue to build a mutual understanding of disability. To that end, we explored ICF-CY body function b codes and activity and participation d codes. We found that parents can contribute constructively in assessing disability in their children.18,24–26
We then took 1 step further by considering parents’ most frequent orally expressed concerns and hopes for the future. First, we listened to what they were actually saying to analyse their expressions and find ways to help and support them better in the future. Such expressions especially apply when children grow older and make the transition from day care to school as well as in adolescence. Second, we wanted to identify a possible relationship between their own freely formulated expressions about their concerns and hopes for the future and their own assessment of their children’s disability. Third, we wanted to validate both sets of information using psychometric and Rasch data analysis.27,28 This would allow for consideration of methods for online and repeated registration of parents’ concerns and assessment data to provide better support and services and for creation of methods of repeated follow-up on purposely improved interventions.
To gather information on parents’ concerns and hopes for the future, we employed a grounded theory approach 29 with which parents expressed their thoughts and concerns freely. The authors read the parents’ writings, evaluated and discussed the writings, and sorted them into sections and subsections. We evaluated and agreed on changes in our opinions, and finally we counted and multiplied the issues delivered and issued by the parents. We found that the parents covered a wide range of issues regarding concerns and hopes. Despite 475 different issues being expressed, the data were not saturated, indicating that more concerns could have been added if more parents had participated. When reading, understanding and sorting the data, we agreed on 83% of the expressions and sorted the remaining 17% on repeated reading and discussion about the expressed meaning. When multiplying the number of issues by the number of parents expressing them, we found that quantitatively, by far, the most imminent concerns were about education and especially about understanding, goodwill, and communication related to community support (Table 2). This is in line with our daily clinical experience. Examples of the expressed issues are given in Table 3.
The obtained data were consistent and tended to measure related issues, as the inter-issue correlation was .35, the corrected issue-total correlation was .58, and Cronbach’s α was high at .95. The 95% confidence intervals around the mean issues score were also narrow, indicating that data collection could be repeated with a good probability of obtaining identical results (Table 4).
When analysing the variance of issue data using the Rasch approach, we found good alignment to the Rasch model, with mean infit and outfit MNSQs around 1 and a mean measure around 0. The τ values showed good discrimination ability when using the 5-qualifier scoring (Table 5). Also, and very importantly, the Rasch map of concerns and hopes for the future illustrated a sound distribution of issues on the right side of the map and children on the left (Figure 1). The issues expressed and the children who were the subjects of the expressions were closely aligned, and the children were shown to represent a continuum of disability severity (Figure 1). So far, we can conclude that the expressed issues represented the population of children well. In other words, parents’ concerns and hopes for the future were representative of the population of children mentioned, and the parents represented the children well. It can be that concerns and hopes for the future may have a different meaning when they are illustrated through the degree of concern on each issue. Thus, aid is only mentioned as a concern by a few parents (Table 2) but is of the most concern among the parents of children with the most severe disabilities (Figure 1). However, understanding, goodwill, and communication qualitatively still apply for the parents of many children in general, not only for the parents of children with the most severe disabilities. This is in alignment with our experiences in clinical practice, where the difficulties of children with the most severe disabilities are often more easily communicated than those of children with milder and often not immediately seen or experienced disabilities.
As in a previous study, 24 the parents were asked again to assess their own children’s disability using 26 ICF-CY b and d codes (Table 1), qualifiers representing issues with body functions as well as activity and participation items representing situations in daily living from the morning to the next morning. When comparing the child code maps of the ICF-CY data from the 2 occasions half a year apart, the ICF-CY codes had similar placements (data not shown). However, the values were not exactly the same, as the population of children represented was different, because fewer parents chose to assess their child’s disability with ICF-CY codes the second time (Figure 2). 24 Also, the τ values showed high closeness between qualifiers 4 and 5 (Table 5). Qualifier 4 describes children with only limited ability, and qualifier 5 describes children with no ability.
We combined the ICF-CY assessment and the concerns and hopes expressions to detect how closely related the degree of severity of disability was to the degree of most frequent concerns and hopes for the future. The Rasch measures for both assessments represented quantitative data, so they could be aligned. The correlation R was .36; thus, the assessment data only showed a modest relationship. The closest relationship was seen in the middle field of level of disability, while an increased spread of data was seen among the least and the most disabled children (Figure 3). We did not include other parental factors that could influence concerns and hopes for the future; however, such factors could theoretically influence outlier data, as observed in the figure. We might conclude that the relationship between severity of disability and concerns and hopes for the future is not most strongly aligned among children with the most disability but rather among children over a broader spectrum of disability. In addition, we could conclude that each parent had personal and thus relatively diverse concerns and hopes for the future.
According to the 3 areas of concern regarding hope, as mentioned in the ‘Introduction’ section, we found the following.
First, the documented finding that parents seek qualitative and inclusive care, including understanding of family needs, social support, coping strategies, involvement in decisions, and avoidance of fighting for their children,1–5 applies to our group of parents as well. These desires are represented in sections regarding community support, social issues, and social tasks, and there is a strong emphasis on understanding, goodwill, and communication (Table 2). Examples are given in Table 3. Related to severity of disability and by comparing data in Table 2 with corresponding data in Figure 1, parents of children with relatively less severe disabilities were more concerned about most of these issues than other parents were. A concern with the efforts of dedicated personnel to support the child and plan for the future was expressed most often by parents of children with more severe disabilities. These findings may point to the fact that support for children which thus gives hope to their parents is more common among children with more severe disabilities, whereas support rendering hope is more difficult to receive or less often provided for children with less severe disabilities.
Second, hope is expressed in relation to different circumstances. Hope that treatments and a cure will make the child better is only weakly expressed with zero emphasis on treatment (Table 2). Quality of life, future well-being, future health, education, medical care, and support from health care professionals are expressed in many different ways, as illustrated by topics such as future functions, training, casework, understanding, education, individual learning and support, future relations, management of needs by others, societal perceptions, capaciousness, expectations, possibilities, and sibling relations (Table 2). Examples are given in Table 3. As illustrated in Figure 1, these issues of hope are related to children with less severe disabilities, except hope about sibling relations, which is expressed on behalf of children with far more severe disabilities. The worry that a child will not experience contentment in adult life is also expressed related to children with less severe disabilities. Finally, parents of children with relatively more severe disabilities express hopes that their children will accept their own disabilities and have self-confidence (Figure 1).
Third, as mentioned earlier, the issue of communication and partnership with parents is most strongly expressed by parents of children with less severe disabilities (Table 3 and Figure 1). Communication related to fear of loss is also shown to be an issue in families who have a child with the most severe level of disability (Figure 1).
In conclusion, parents freely expressed their concerns about and hopes for the future of their children with disabilities, without using a defined questionnaire. We analysed the data on parents’ concerns and hopes using a grounded theory approach; then we sorted and discussed the issues and had the parents assess their concerns and future hopes on the basis of the issues that emerged by using a 5-step qualifier scale. Concomitantly, the parents assessed their children’s disability again using a group of 26 ICF-CY body function b codes and activity and participation d codes covering issues during 24 h of daily living, which they assessed on a 5-step qualifier scale. Both sets of qualitative data demonstrated good reliability and validity in psychometric data analysis. Rasch analyses of both scales showed good alignment to the Rasch model, thus strengthening the consistency of both data sets. The child map and the issue and code map showed good alignment between the participating children, the issues produced, and the ICF-CY codes employed. When relating the quantitative data produced by Rasch analysis of both scales, we demonstrated some alignment between disability severity and parents’ concerns and hopes for the future, but we also found that other unanalysed factors may be influential.
We believe that both approaches could strengthen trust in parents’ own expressions of concerns about and hopes for the future as well as their own assessments of disability in their children and that such data could strengthen cooperation between parents and health services directed towards both the family and their children with disabilities. Furthermore, repeated expressions and assessments of parents, analysed accordingly, could be fruitful for continuing dialogue and assessment of improvements in health services. We believe that parents do know best about their family and their own children with disabilities.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Danish Ministry of Social Affairs, partnership project §16,21,31, and administered by the National Board of Health.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
N.O.I. contacted parents, obtained score data, performed statistical data analysis, and drafted the manuscript. M.B. and N.O.I. separately and then together performed a grounded theory approach to parents’ expressions, and K.O.G. contributed to data design and data analysis. All reviewed and accepted the manuscript.
Ethical Considerations
Neither the Danish Ministry of Social Affairs nor the National Board of Health influenced the study protocol, data collection, data analyses, or results. All of the eligible parents in a defined geographical area were contacted by mail to participate in this study. The parents were known to us. Participation was voluntary for the parents and caregivers. The protocol was accepted by and registered at the Danish Data Protection Agency (DOK121763) before the start of the research. Approval for the protocol was sought from the National Board of Health (Project 7-202-05-207/8).