
Abstract
Background:
The aim of this study is to examine the hematological and biochemical variables in patients diagnosed with cancer-related stroke who have different types of cancer and to evaluate the effects of these variables.
Methods:
This retrospective study was conducted at a tertiary hospital stroke center and included 153 patients diagnosed with cancer-related stroke. Comprehensive etiological investigations were performed, and patients were classified according to the Trial of Org 101072 in Acute Stroke Treatment (TOAST) classification. Laboratory parameters including
Results:
The study found significant variations in hematological and biochemical parameters among different cancer types. Specifically, glomerular filtration rate, activated partial thromboplastin time, prothrombin time, and international normalized ratio levels showed significant differences across cancer types (P < 0.05), indicating that these factors may play distinct roles in the pathophysiology of cancer-related strokes.
Conclusions:
This retrospective study highlights the importance of considering cancer-specific factors in the management of stroke risk, particularly in cancers such as pancreatic and colon, which show a predisposition to earlier stroke occurrence. The elevated coagulation factors in these patients suggest the potential need for early preventive treatment with anticoagulants or thrombin inhibitors.
Introduction
The classification of ischemic stroke etiology is crucial for organizing treatment and establishing a common language among clinicians. For this reason, Adams Jr et al proposed the Trial of Org 101072 in Acute Stroke Treatment (TOAST) classification, which is easy to use and allows us to classify the etiological subtypes of ischemic stroke.1-3 The TOAST classification categorizes ischemic strokes into 5 subtypes based on their etiology. Large-artery atherosclerosis refers to strokes caused by significant stenosis or occlusion of large arteries, such as the carotid or vertebral arteries, typically resulting from emboli or hemodynamic compromise due to atherosclerosis. Cardioembolism (CE) involves strokes caused by emboli originating from the heart, often linked to conditions such as atrial fibrillation, myocardial infarction, or valve disease. Small-vessel occlusion, also known as lacunar stroke, results from the occlusion of small, deep penetrating arteries, commonly associated with chronic conditions such as hypertension (HT) or diabetes, leading to lacunar infarcts. Stroke of other determined etiology refers to strokes caused by less common conditions such as vasculitis, dissection, hypercoagulable states, or rare genetic disorders. Finally, stroke of undetermined etiology occurs when the cause of the stroke remains unclear, either due to the identification of multiple potential causes or the inability to determine a cause despite thorough evaluation. Following these 5 classifications, the increasing frequency of stroke in patients with cancer and the need to include this in the classification emerged. Therefore, the TOAST classification system has recently been expanded to include a category for cancer-related strokes. The inclusion of this category acknowledges that cancer can increase stroke risk through various mechanisms, including hypercoagulability, tumor compression of blood vessels, and abnormal platelet aggregation 4 (Table 1). These factors require distinct diagnostic and therapeutic strategies to effectively manage the risk and treatment of strokes in patients with cancer.
Updated TOAST classification with cancer-related stroke.

Cancer-related stroke is a significant and growing concern within the field of cerebrovascular diseases, representing a notable subset of ischemic strokes. It is estimated that cancer-related strokes account for approximately 10% to 13% of all ischemic strokes. 5 This subtype is particularly associated with certain cancers, including lung, pancreatic, colorectal, breast, and prostate cancers, which are often diagnosed at later stages. These advanced-stage cancers are linked to a higher risk of stroke, further complicating patient care and prognosis. 6
The mechanisms underlying the connection between cancer and stroke are complex and multifactorial. Shared risk factors such as smoking, obesity, and sedentary lifestyles contribute to the incidence of both conditions.6-8 Cancer-associated stroke can occur through various mechanisms, and this diagram categorizes the risk factors under several main headings. First, direct tumor effects, such as tumor invasion of blood vessels, sinovenous thrombosis, leptomeningeal metastases, and tumor emboli, can directly impact the vasculature, increasing the risk of stroke. Tumor cells can interact with the coagulation system through mechanisms such as producing hemostatic proteins, activating platelets, and adhering directly to normal cells. Chemotherapy and radiation therapy, commonly used in cancer treatment, also elevate stroke risk, particularly through the vascular effects of certain chemotherapy agents and radiation-induced vascular damage. In addition, invasive procedures (eg, lumbar puncture and craniotomy) may contribute to stroke risk by causing vascular trauma. Cancer-supportive therapies, such as hematopoietic stem cell transplantation and the use of growth factors, can also affect coagulation pathways. Finally, infections, which are frequent complications in patients with cancer, can trigger inflammatory responses that further increase the risk of stroke. Together, these factors illustrate why stroke risk in patients with cancer is complex and multifactorial.9-11
Patients presenting with cancer-related stroke often display distinct clinical and diagnostic features. Elevated
As advancements in cancer treatment continue and the global population ages, the incidence of cancer-related strokes is expected to rise. This trend underscores the urgent need for comprehensive research to establish standardized risk assessment protocols and treatment guidelines specifically for this subtype of stroke. Recognizing and addressing the unique pathomechanisms of cancer-related stroke is crucial for improving patient outcomes. 12
The aim of this study is to examine the hematological and biochemical variables in patients diagnosed with cancer-related stroke who have different types of cancer, and to evaluate the effects of these variables on the development of cancer-related stroke.
Materials and Methods
This retrospective study was conducted at the Stroke Center of Bakırköy Dr. Sadi Konuk Training and Research Hospital, a tertiary care facility.
All patients with stroke undergo etiological classification according to TOAST classification in the stroke clinic during hospitalization and after discharge. Baseline etiological tests include magnetic resonance imaging, carotid and vertebral magnetic resonance angiography, electrocardiogram, and echocardiography. Patients are further evaluated with 24- or 48-hour rhythm Holter monitoring, while younger stroke patients undergo transesophageal echocardiography (TEE), bubble test, vasculitis panel, Fabry disease testing, and a genetic thrombophilia panel. Patients whose tests return normal are defined as “other stroke etiology.” In addition, patients with lacunar infarcts and associated risk factors exclude from “other stroke etiology.” In our study, patients with a malignancy history or active malignancy and who were not classified under traditional stroke causes were evaluated by 3 stroke specialists, and those identified as cancer-related strokes were included.
Data collection
The independent variable was the type of cancer, and the dependent variables were the admission laboratory findings, specifically
Statistical analysis
Descriptive statistics were used to summarize the data, including mean, median, standard deviation, and range for each laboratory parameter within each cancer type. One-way analysis of variance (ANOVA) was performed to assess differences in CRP, ESR, and fibrinogen levels across different cancer types. Post hoc tests, specifically Tukey honest significance test or Bonferroni correction, were applied to identify specific group differences if the ANOVA indicated significant differences. All statistical analyses were conducted using SPSS software with a significance level set at P < .05.
Results
Patient demographics and cancer types
A total of 201 patients diagnosed with cancer-related stroke were evaluated retrospectively between January 2019 and January 2024. Forty-eight patients were excluded due to missing admission laboratory findings, incomplete follow-up data, or the presence of multiple etiologies. In the etiological examination of these patients, findings that could suggest CE as a stroke risk factor were identified. These included discrepancies between echocardiography results conducted a week apart, the possibility that long supraventricular tachycardia run (SV-RUN) attacks could be the cause, young patients without or unable to tolerate TEE, and some blood tests performed at other centers and being inaccessible. Therefore, these patients were excluded from the study due to the consideration of multiple possible etiological factors. Following the exclusion of 48 patients, a total of 153 patients were included in the study.
The mean age of the patients was 69.6 ± 11.4 years, with a median age of 70 years. The time from cancer diagnosis to the occurrence of stroke was calculated as 3.72 ± 3.12 (1-20) years. The gender distribution was 57.5% men and 42.5% women. The distribution of cancer types among the patients is detailed in Table 2.
The distribution of cancer types and time from cancer diagnosis to stroke and comorbidities.
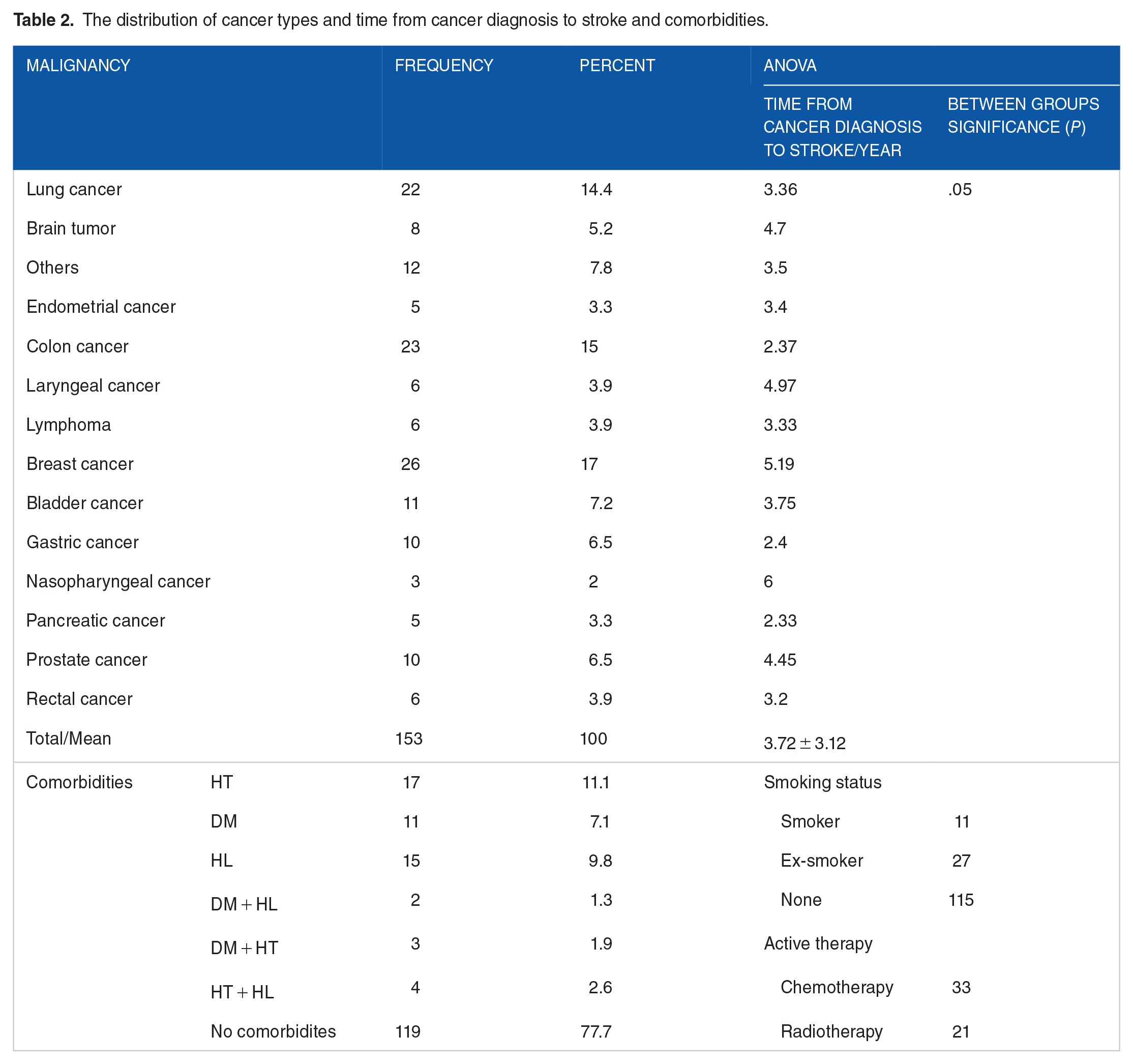
Patients with diabetes mellitus (DM), HT, or hyperlipidemia (HL) were analyzed separately, and those whose stroke etiology was attributed to these conditions were also excluded from the study. In 34 patients, etiology was not attributed to these conditions and considered cancer-related stroke. Of 34 patients, 17 had HT, 11 had DM, and 15 had HL. No patient had a history of coronary artery disease. Among the patients, 2 had both DM and HL, 3 had both DM and HT, and 4 had both HL and HT. In 119 patients, no comorbidities were present.
The time from cancer diagnosis to stroke varies according to the type of cancer. Of the 153 patients with cancer-related stroke, 6 had a history of pancreatic cancer and 24 had a history of colon cancer. The mean duration of stroke in patients with pancreatic cancer was 2.33 years and this value was 2.37 years in patients with colon cancer. The duration of stroke was found to be shorter in patients diagnosed with pancreatic and colon cancer compared with other cancer types and this difference was significant (Table 2).
Hematologic and biochemical variables in patients with cancer
Laboratory values for different types of malignancies including mean and standard deviation for various parameters are presented in Table 3. The values are organized by malignancy type, such as breast cancer, colon cancer, lung cancer, and cover a range of laboratory tests including glomerular filtration rate (GFR), activated partial thromboplastin time (aPTT), prothrombin time, international normalized ratio, platelet (PLT), white blood cell, neutrophil, lymphocyte,
Laboratory values for different types of malignancies.

Abbreviations: aPTT, activated partial thromboplastin time; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; GFR, glomerular filtration rate; INR, international normalized ratio; LYM, lymphocyte; NEU, neutrophil; PLT, platelet; PT, prothrombin time; S, second; Std. dev, standard deviation; WBC, white blood cell.
When comparing cancer types with laboratory findings, the GFR values showed a significant difference between groups (F = 1.97, P = .031). In addition, aPTT, PTZ, and INR also demonstrated significant differences between groups (P = .049, P = .013, P = .011). A highly significant difference was observed in
Comparison of cancer types and laboratory values.

Abbreviations: aPTT, activated partial thromboplastin time; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; GFR, glomerular filtration rate; INR, international normalized ratio; PT, prothrombin time; s, second.

Graphical representation of cancer types and laboratory values.
Discussion
Cancer-related strokes represent a significant challenge within the broader field of cerebrovascular diseases. Despite the growing body of research, there remains a substantial gap in understanding the specific mechanisms by which different types of cancer influence stroke onset and progression.13-15 This study aims to address this gap by examining the hematological and biochemical variables associated with cancer-related strokes, with a focus on how these variables differ across various cancer types.
In our study, a significant difference was found between cancer types and the time to stroke development among the groups. The shortest duration was observed in colon cancer, and the longest duration in nasopharyngeal cancers. In a systematic review showing that stroke incidence increases in survivors of adult cancers, 16 the average time from cancer to stroke for colon cancer was found to be 1.47 years. Although this duration was found to be longer in our study, it is still shorter compared with other types of cancer included in the study. This may indicate that patients with colon cancer are at higher risk of stroke. It may also suggest that colon cancer has a higher procoagulant effect. Based on this, while earlier initiation of anticoagulant therapy for these patients might be considered, due to ischemias related to metastasis and the risk of bleeding, early anticoagulation cannot be definitively recommended.
Breast cancer had the highest number of patients in the study. Despite this, the time from cancer diagnosis to stroke was 5.1 years for breast cancer and 2.3 years for colon cancer. This significant difference showed that the reason for the earlier occurrence of stroke in patients with colon cancer was independent of the number of patients. The fact that breast cancer is seen at a younger age compared with colon cancer,17-19 and that vascular risk factors for stroke have not yet been seen in these patients may explain why the time until stroke occurrence is longer in patients with breast cancer compared with those with colon cancer.
Our study found significant variations in hematological and biochemical parameters among different cancer types. Notably, GFR, aPTT, PTZ, and INR levels showed significant differences across cancer types, indicating that these factors may play distinct roles in the pathophysiology of cancer-related strokes. The most striking findings were observed in
Our results align with previous studies that have highlighted the role of hypercoagulability in cancer-related strokes. The significant elevation of
In a study comparing the new-generation oral anticoagulant with aspirin, no significant difference was found in terms of use among cancer-related stroke patients. 29 In another study, it was shown that direct thrombin inhibitors and antiplatelet agents reduced stroke recurrence in these patients.14,15 The finding of significantly elevated coagulation parameters in the laboratory results of this study suggests that anticoagulant therapy may be effective in selected cancer types, especially in rectal and endometrial cancers. Recommending anticoagulant therapy for all cancer types may be insufficient in this regard. However, it may be suggested that early initiation of anticoagulants or thrombin inhibitors may be necessary as stroke preventive treatment in patients with rectal and endometrial cancer.
The limitations of our study are being retrospective and the sample size, while adequate for general trends, may not fully capture the heterogeneity of cancer-related strokes across all cancer types. Another limitation is the potential for confounding variables such as the use of anticoagulants, the stage of cancer at diagnosis, or therapies for cancers. The duration of anticoagulant use, differing treatment protocols for each type of cancer, the length of cancer treatment, and the end of treatment create gray areas that prevent the standardization of risk factors in patients with cancer-related stroke. This presents itself as a limitation in our study. These factors could impact the observed associations between cancer type and stroke-related biochemical parameters. In addition, the fact that the study was conducted in a single tertiary center limits the generalizability of the findings.
Future studies should focus on prospective analyses with larger and more diverse patient populations to confirm our findings. Investigating the efficacy of early intervention with anticoagulants or thrombin inhibitors in patients with high-risk cancer such as rectal and endometrium could provide valuable insights into preventive strategies.
Conclusions
This retrospective study offers important insights into how various cancer types impact the biochemical profile of cancer-related strokes. Examining data retrospectively allows for a comprehensive evaluation of cancer-specific factors that influence stroke risk, but limits a deeper understanding. The findings highlight the particular stroke risk in cancers such as pancreatic and colon, where earlier stroke occurrence is more common. In addition, elevated coagulation factors observed in patients with rectal and endometrial cancer suggest a potential need for early preventive measures, including anticoagulants or thrombin inhibitors.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
İA: concept, writing, draft, literature searching, methodology, data analysis; HAE: writing, literature searching, data analysis, writing; ET: data collecting, contributed materials, writing, draft; VY: methodology, design and supervision. All authors approved the version to be published.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for Publication
We confirm that we have obtained the necessary consent for publication from the patients or their legal guardians for the use of their data as reported in the study
Ethical Declaration
The study was conducted in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Clinical Research Ethics Committee of Bakırköy Dr. Sadi Konuk Training and Research Hospital. The approval was obtained decision number 2023-18-09 and protocol number 2023/368 at September 18, 2023. We confirm that written informed consent was obtained from all participants or their legal guardians prior to the initiation of the study. This has been explicitly approved by the ethics committee.