
Abstract
Background:
Extrathyroidal extension (ETE) significantly affects the treatment strategy for thyroid cancer. We present a new method to predict ETE of papillary thyroid carcinoma (PTC).
methods:
We enrolled 1 481 patients with PTCs. The ETE was classified into minimal and gross ETE. Using the novel “contact angle of the tumor on sonography” (CATS) system, we calculated optimal cutoffs for predicting ETE according to tumor location and compared the diagnostic performance to that of previous methods.
Results:
The optimal cutoff angles for predicting anterior minimal and gross ETE were 41.5° and 49.4°, respectively, while those for posterior ETE were 39.8° and 54.6°, respectively. The optimal cutoff angle predicting tracheal ETE was 88.0°. The diagnostic performance was comparable to that of previous methods.
Conclusion:
The CATS method for predicting ETE is a valuable alternative.
Introduction
Extrathyroidal extension (ETE) is an adverse prognostic factor in patients with papillary thyroid carcinoma (PTC).1,2 The risk of lymph node metastasis and local recurrence increases, and survival is reduced if an ETE is present.3-5 The American Joint Committee on Cancer (AJCC) staging system includes ETE status. 6
However, the significance of ETE remains controversial. PTC with gross ETE requires near-total or total thyroidectomy although some studies have suggested that active surveillance (AS) is possible for papillary thyroid microcarcinoma (PTMC) with gross ETE limitedly.7,8 The recently updated eighth version of the AJCC staging system classifies a tumor with gross ETE into the strap muscle as T3b; a tumor with minimal ETE is not classified in this manner. 9
However, the 2015 American Thyroid Association (ATA) guidelines consider patients with minimal ETE at intermediate risk of recurrence. Minimal ETE is a risk factor for poor locoregional recurrence-free survival compared with cases without ETE.10,11 Although thyroid lobectomy or AS may be adequate for patients with anterior minimal ETE, for those with posterior minimal ETE, it is important to carefully consider the surgical extent, or employ AS, because of the risk of esophageal or recurrent laryngeal nerve invasion. 12 It is essential to rule out an ETE before choosing AS or surgical extent.
Preoperative ultrasonography (US) is the modality widely used to evaluate ETE status in PTC patients. 13 Most of the various methods are difficult to apply and characterized by interobserver variability; also, methods differ by tumor location.14-17 We present a new method for predicting minimal or gross ETE and identify the optimal cutoff angles for predicting ETE in all locations.
Patients and methods
Patients
We retrospectively collected data for 1,545 consecutive patients who underwent thyroidectomy for PTC from March 2010 to January 2019 at Haeundae Paik Hospital, Inje University of Korea. Patients with no preoperative US images or who were operated on to treat recurrent cancer were excluded. Patients with US nodules > 4 cm in diameter were excluded because they required total thyroidectomy. Finally, 1 481 patients with PTC were included, of whom 371 had pathologically confirmed ETE that was microscopic (minimal) (n = 324) or macroscopic (gross) (n = 47).
Definitions of ETE
ETE was classified into minimal and gross ETE. Minimal ETE was defined as tumor invasion beyond the thyroid capsule identified only by pathological examination. Gross ETE was defined as tumor invasion beyond the thyroid identified at surgery and confirmed by the pathologist. No ETE indicates that neither pathological examination nor intraoperative inspection revealed tumor invasion.
Imaging and image analysis
Our Department of Thyroid and Endocrine Surgery conducts preoperative US evaluations for all patients scheduled for thyroidectomy. The US images and medical records were retrospectively analyzed focusing on ETE confirmed during surgery. All US images were analyzed by one endocrine surgeon (operator). If multiple thyroid nodules were present, we analyzed the largest one diagnosed before surgery. The US images were classified with reference to a previous study 18 as follows: the capsular abutment, disruption, or protrusion. Capsular abutment was defined as the lack of intervening tissue between the nodule and thyroid capsule. Capsular disruption was defined as loss of the perithyroidal echogenic line at the site of contact with the nodule. Capsular protrusion was defined as bulging as into adjacent structures with loss of the normal thyroid margins. Capsular abutments and protrusions are graded according to the perimeter ratios (abutment or protrusion perimeter/nodule perimeter × 100%) (Figure 1A). The abutment and protrusion ratios were measured anteriorly and posteriorly in the transverse view. A posterior thyroid capsule evident on US was defined as a linear margin between the point where the posterior capsule of the thyroid gland reached the common carotid artery and the point where the posterior capsule and trachea of the thyroid met (Figure 1B and C). The angle between the tumor and thyroid capsule was defined the point (vertex) at which the transverse and anteroposterior diameters of the tumor were maximal. 19 We then set two points where the outer border of the tumor met the thyroid capsule and measured the angle defined by these three points (Figure 1D).

Classification of ultrasonography images. (A) Anterior margin of the thyroid lobe (white dotted line), posterior margin of the thyroid nodule (black short-dashed line), and tracheal margin (white long-dashed line). (B, C) Contact angle between the tumor and thyroid capsule (arrow). (D) Contact angle between the tumor and tracheal wall (arrow).
Statistical analysis
The clinical and pathological characteristics of the two groups were compared using the χ2 or Fisher’s exact test for continuous data and the independent t-test or the Mann–Whitney U-test for categorical data. Receiver operating characteristic (ROC) analysis was used to determine the optimal angles for predicting ETE. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and diagnostic accuracy were calculated. All statistical analyses were performed with SPSS software (version 25.0; IMB Corp., Armonk, NY, USA). A P value < .05 was considered significant.
Results
The demographic characteristics of the patients and histological characteristics of the tumors are provided in Table 1. Of the 1 481 patients, ETE were observed in 371 (25.1%), including 324 with minimal ETE (21.9%) and 47 with gross ETE (3.2%). Patients with ETE had significantly larger tumors than those without ETE (mean diameter, 1.2 ± 0.6 vs 0.9 ± 0.5 cm, P < .001). Compared to patients without ETE, those with ETE were more likely to undergo total thyroidectomy (68.7% vs 92.7%, P < .001) and exhibit central and lateral lymph node metastases (28.3% vs 39.1% and 4.2% vs 12.1%, respectively, P < .001).
Demographic characteristics of the patients.

Abbreviations: ETE, extrathyroidal extension; LN, lymph node; LND, lymph node dissection.
Values are expressed as mean ± standard deviation or numbers (%).
The ROC curves obtained for diagnosing anterior ETE are shown in Figure 2 (see also Table 2). The optimal cutoff for ruling out anterior minimal ETE was 41.5°, and the optimal cutoff for predicting anterior gross ETE was 49.4° (for a tumor ⩽ 4 cm in diameter).

ROC curves of the contact angles for detecting anterior minimal ETE (A) and gross ETE (B). ETE indicates extrathyroidal extension; ROC, receiver operating characteristic.
CATS cutoff points based on the ROC curves.

Abbreviations: AUC, area under the curve; CATS, contact angle of tumor on sonography; ETE, extrathyroidal extension; ROC, receiver operating characteristic; SE, standard error.
The AUC, SE, 95% confidence interval, and P value data are provided for each anterior ETE category.
The ROC curve for diagnosing posterior ETE is shown in Figure 3 (see also Table 3). The optimal contact angle of tumor on sonography (CATS) cutoff ruling out a posterior minimal ETE was 39.8° and the optimal cutoff for predicting a posterior gross ETE was 54.6° (for a tumor ⩽4 cm in diameter).

CATS ROC curves for detecting posterior minimal ETE (A) and gross ETE (B). CATS indicates contact angle of tumor on sonography; ETE, extrathyroidal extension; ROC, receiver operating characteristic.
CATS cutoff points based on the ROC curves.
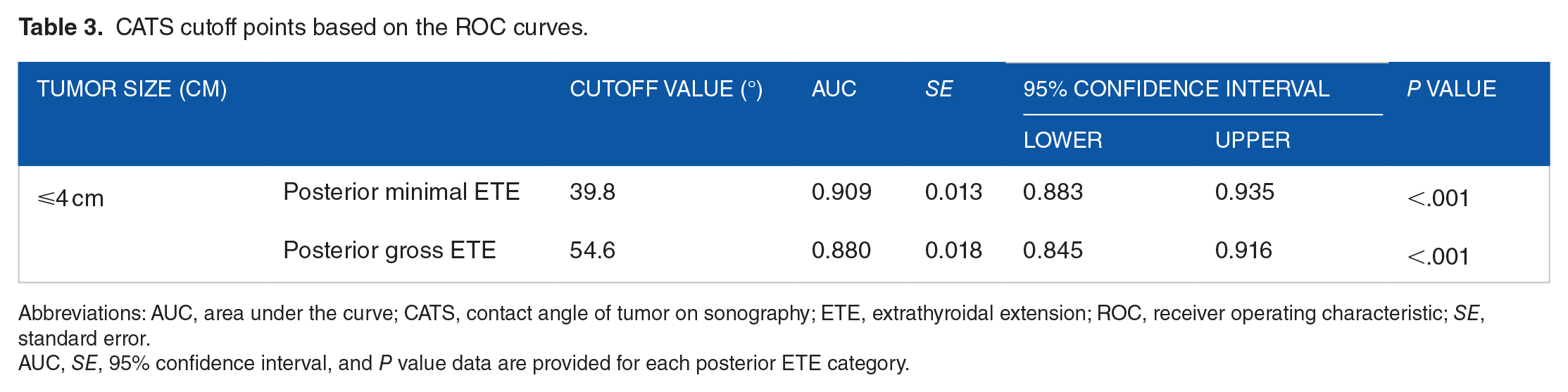
Abbreviations: AUC, area under the curve; CATS, contact angle of tumor on sonography; ETE, extrathyroidal extension; ROC, receiver operating characteristic; SE, standard error.
AUC, SE, 95% confidence interval, and P value data are provided for each posterior ETE category.
The ROC curve for diagnosing tracheal invasion is shown in Figure 4 (see also Table 4). The optimal CATS cutoff for ruling out tracheal invasion was 88.0°.

CATS ROC curve for tracheal invasion. CATS indicates contact angle of tumor on sonography; ROC, receiver operating characteristic.
CATS cutoff for tracheal invasion based on the ROC curves.

Abbreviations: AUC, area under the curve; CATS, contact angle of tumor on sonography; ROC, receiver operating characteristic; SE, standard error.
AUC, SE, 95% confidence interval, and P value data are provided.
Discussion
Thyroid cancer is the most common type of cancer among young adults of both sexes in Korea. 20 PTC is the most common type of thyroid carcinoma, but the frequency of PTMC < 1 cm in diameter is increasing. 21 New management strategies in low-risk PTMC are proposed, but they need to be applied cautiously. 22
The most appropriate surgical extent for PTMC remains controversial.23,24 According to the recently revised 2015 ATA guidelines, patients with thyroid cancer < 1 cm in diameter without ETE and no clinical evidence of cervical lymph node metastasis are indicated for lobectomy. If the tumor is >1 cm but <4 cm in diameter, lobectomy is an appropriate initial treatment. 7
Recently, AS has been suggested for patients with low-risk PTMC < 1 cm in diameter.25,26 It has been claimed that an anterior ETE is not a contraindication for AS. 12 However, a gross ETE requires more extensive surgery and higher staging. So, PTMC patients scheduled for AS should be carefully selected. For some patients treated via thyroid lobectomy and all who require total thyroidectomy, thyroid hormone replacement therapy is necessary. ETE was an exclusion criterion in a South Korean multicenter study of AS.27,28 Some patients may require surgery (lobectomy or total thyroidectomy) and radioactive iodine (RAI) ablation if the postoperative pathological results indicate aggressive histology, vascular invasion, lymph node invasion, or ETE.29,30 Preoperative tumor staging is important to plan the surgery. US is the most sensitive modality for detecting thyroid nodules and can clearly show their shape and size. US also detects lymph node metastases and can be used to determine if there is a need for fine needle aspiration. 31 Thus, US plays a major role in planning surgical extent.
Many retrospective studies reported that minimal ETE was not an independent risk factor for mortality or disease recurrence.32,33 Minimal ETE had little effect on prognosis or quality of life, even if surgery is performed after disease progression. 8 However, a recent study suggested that the combination of a tumor diameter > 2 cm and minimal ETE might be an independent poor prognostic factor. 34 Also, in the 2015 ATA guidelines, minimal ETE is among the indications for RAI. Although a gross ETE does not affected disease-specific survival, several studies found that it affected recurrence. Therefore, the seventh edition of the AJCC staging system includes “T3b” as a new category of tumors with gross ETE.
It is important to evaluate both minimal and gross ETE preoperatively.35,36 Chung et al 18 found that capsular disruption was indicative of anterior minimal ETE (sensitivity: 61.6%; specificity: 87.1%; PPV: 58.5%; NPV: 88.5%; accuracy: 81.3%), while replacement of the strap muscle was indicative of anterior gross ETE (sensitivity: 45.4%; specificity: 99.1%; PPV: 75.9%; NPV: 96.7%; accuracy: 96.0%). Jeong et al 37 found that posterior capsular abutment was indicative of posterior minor ETE (sensitivity: 81.5%; specificity: 68.7%; PPV: 52.6%; NPV: 89.7%; accuracy: 72.5%). The diagnostic performance of our method was similar to that of other methods (Tables 5 and 6).
Diagnostic performance of the sonographic features of anterior ETE.
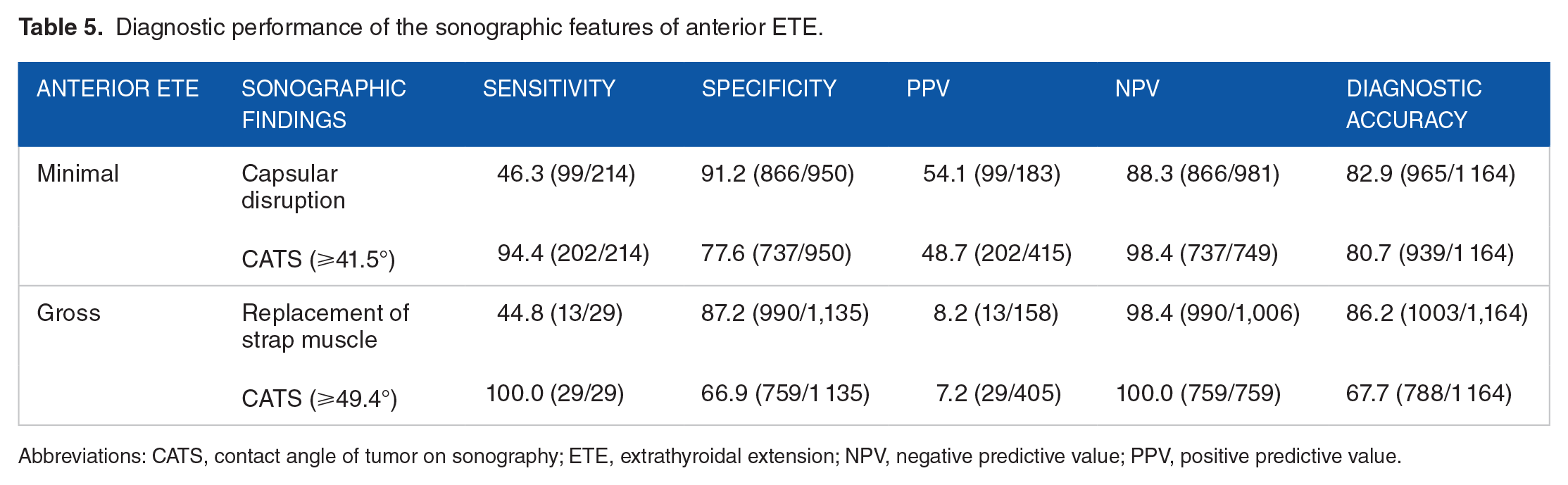
Abbreviations: CATS, contact angle of tumor on sonography; ETE, extrathyroidal extension; NPV, negative predictive value; PPV, positive predictive value.
Diagnostic performance of the sonographic features of posterior minimal ETE.

Abbreviations: CATS, contact angle of tumor on sonography; ETE, extrathyroidal extension; NPV, negative predictive value; PPV, positive predictive value.
We calculated the optimal CATS cutoff for predicting tracheal invasion. An obtuse angle (⩾88.0°) afforded the highest diagnostic performance. Using the images, we calculated the optimal CATS cutoff for predicting ETE of PTMC in various locations (Table 7). Existing methods are compromised by interobserver variability, and results differ by tumor location. The CATS method can be used to evaluate tumors in all locations and simply predict ETE; the results are comparable to those of other methods. So, the CATS system is clinically useful.
CATS cutoff based on ROC curves.

Abbreviations: AUC, area under the curve; CATS, contact angle of tumor on sonography; ETE, extrathyroidal extension; PTMC, possible for papillary thyroid microcarcinoma; ROC, receiver operating characteristic; SE, standard error.
The AUC, standard error, 95% confidence interval, and P value data are provided for ETE in each PTMC location.
This study had some limitations. First, it is a retrospective design and uses previously captured images. We think that a prospective study with preoperative images captured by surgeons would have been preferable. Also, three-dimensional ultrasound images are more accurate than the images we analyzed and reduce interobserver variability. Also, we did not evaluate interobserver agreement. A large future prospective study would likely provide more accurate results. Finally, the number of gross ETE was small. Although an AUC value ⩾0.7 is statistically meaningful, more precise results would have been obtained if more cases with gross ETE had been evaluated.
Conclusion
Our new CATS system for ETE evaluation yields results comparable to those of existing methods. Our study suggests that CATS may be a valuable tool in predicting the surgical extent and identifying potential candidates for AS. While these preliminary findings show promise, additional research is necessary to confirm this potential application of CATS. Although the CATS system is useful for predicting ETE. A large prospective study would enhance the reliability of the cutoff. So, the CATS system shows promise as an additional method for predicting ETE in PTC.
Footnotes
Acknowledgements
None
Author contributions
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
The study protocol was designed according to the principles of the Declaration of Helsinki and approved by the Institutional Review Board of Inje University Haeundae Paik Hospital (approval no. HPIRB 2022-03-012). The need for informed consent was waived.