
Abstract
Background:
Preoperative absolute lymphocyte count (ALC) and carcinoembryonic antigen (CEA) are useful prognostic indicators in colorectal cancer (CRC); however, the role of the ALC-to-CEA ratio (LCR) has been less addressed.
Methods:
A total of 189 stage I to III CRC patients who underwent radical resection were enrolled retrospectively. The significance of the LCR in predicting disease-free survival (DFS) and overall survival (OS) was calculated and compared with other markers based on ALC. The DFS and OS differences among the low- and high-LCR subgroups and risk factors for the outcome were estimated by Kaplan–Meier analysis and the Cox proportional hazards model, respectively.
Results:
Taking 0.28 as the cutoff point, the LCR has a sensitivity and a specificity of 75.60% and 77.00%, respectively, in predicting OS. The prognostic efficacy of LCR was significantly superior to that of other markers based on ALC for predicting DFS and OS. A total of 34.92% (66/189) of patients displayed a low LCR (<0.28), and these patients were more likely to present poor cell differentiation (P = .03), tumor deposits (P < .01) and advanced T (P < .01) and liver metastasis (P = .02). Patients with a low LCR had significantly worse DFS (Log Rank = 34.98, P < .01) and OS (Log Rank = 43.17, P < .01) than those with a high LCR. The LCR was an independent prognostic factor for both DFS (hazard ratio (HR) = 0.35, 95% confidence interval (CI): 0.20-0.62, P < .01) and OS (HR = 0.18, 95% CI: 0.08-0.37, P < .01).
Conclusions:
The LCR is a superior predictor of survival in stage I to III CRC, and patients with a low LCR have an inferior outcome; however, additional studies are required to validate its prognostic role.
Keywords
Introduction
Colorectal cancer (CRC) is a serious health problem worldwide, with annually increasing morbidity and mortality among those younger than 50 years. 1 Although stages I and II and most stage III patients can be cured by a single surgery or surgery plus chemotherapy, 2 unfortunately, a high proportion of these early-stage cases will eventually progress to metastatic disease, and 80% to 90% of these patients will become unresectable. 3 The search for reliable and easily accessible prognostic markers for these patients is clinically important.
It has long been established that immune cells play a fundamental role in controlling the initiation and progression of cancer4,5 and that lymphocytes are the main source of adaptive antitumor immune responses. 4 In line with these findings, the peripheral absolute lymphocyte count (ALC) was reported to have an important prognostic role in many cancers, including gastric cancer, 6 pancreatic cancer, 7 breast cancer, 8 and CRC.9,10 However, it is notable that ALC is limited due to its low efficacy in predicting the outcome of CRC. For example, Shinji et al 11 reported that the area under the curve (AUC) of ALC in predicting recurrence-free survival (RFS) was 0.61, with a specificity of 48.8%. In addition, Iseki et al’s 10 study also indicated that the AUC of ALC in predicting overall survival (OS) was 0.58, with a sensitivity of 26.8%. To improve these disadvantages, a group of new prognostic indicators were explored based on ALC in recent years, including the neutrophil-to-lymphocyte ratio (NLR), 12 lymphocyte-to-monocyte ratio (LMR), 13 and prognostic nutritional index (PNI). 14 However, these indicators commonly featured elevated AUCs12-14 but were not consistently superior to ALC by itself in different studies,9,11 and more robust markers are still needed.
Carcinoembryonic antigen (CEA) is a classical tumor marker in CRC that plays a critical role in the diagnosis, surveillance, and prognosis of the disease. 15 However, it is also notable that a single preoperative CEA level is limited by its inferior efficacy in predicting the outcome. For example, Gunawardene et al 16 performed a study that enrolled 237 stage I to IV patients and found that the AUC of a single CEA measurement in predicting OS was 0.62 with a reduced cutoff point (3.3 ng/mL). In addition, Kim et al conducted a study that included 463 stage II patients who underwent curative surgery and found that the AUC of a single CEA in predicting RFS was 0.60 (with a cutoff point similar to Kim et al). 17 In recent years, some studies have tried to combine CEA with other markers, such as PNI and CA199; however, such combinations still have difficulty distinguishing the outcome in separate subgroups.18-20 Mechanistically, CEA has a profound effect in encouraging the disease by inducing the epithelial-mesenchymal transition (EMT) process, increasing cell invasiveness and inhibiting apoptosis. 21 Taking into consideration that ALC reflects the antitumor immune strength and CEA represents the aggressiveness of the cancer cells, it is plausible that the ALC-to-CEA ratio (LCR) would be a sound marker to reflect the battle between the immune system and cancer cells and would be useful for prognostication; however, related studies are still rare.
In this study, we explored the prognostic value of the LCR and compared its prognostic efficacy with additional markers established on ALC in stage I to III CRC.
Methods
Patient enrollment
Colorectal cancer patients experiencing radical resection from December 2012 to April 2020 in Hainan Hospital of Chinese PLA General Hospital were retrospectively enrolled. Patients were included with the following criteria: (1) age > 18 years and (2) pathologically confirmed as adenocarcinoma; and they were excluded if any one of the following criteria was met: (1) receiving any preoperative neoadjuvant therapies; (2) lack of preoperative laboratory results or missing any pathological tumor node metastasis (TNM) information; (3) suspected distant metastasis by imaging examinations, in particular by positron emission tomography-computed tomography (PET-CT); (4) multiple cancers; and (5) loss or refusal to follow-up or a follow-up period of fewer than 3 years. In addition, pT4, lympho-vascular, or perineural invasion are analyzed as risk factors according to the European Society for Medical Oncology (ESMO) or National Comprehensive Cancer Network (NCCN) guidelines. Other data were collected as previously described.22,23 This study was supervised and approved by the ethics committee of Hainan Hospital of Chinese PLA General Hospital (ID: 301HLFYLS15) and conducted in accordance with the principles stated in the Declaration of Helsinki; informed consent was obtained from the patients or their authorized relatives.
Tests for ALC, CEA, and calculation of LCR
Laboratory tests were carried out as described in our previous report. 23 The ALC and CEA were obtained from routine blood tests before surgery; for those with more than one test result, the nearest one to surgery was adopted. The reference for ALC and CEA was 0.7 to 4 × 109/L and 0 to 5 µg/mL, respectively. The LCR was calculated by ALC divided by CEA and then divided by 109 for the convenience of data input. The NLR, LMR, and PNI were calculated as described in previous studies.12-14
Definition of disease-free survival and OS
The follow-up was conducted as described in previous reports. 23 Disease-free survival (DFS) was defined from the time of surgery to the date of any recurrence or metastasis or the date of death from any cause. Overall survival was defined from the same point to the date of any cause of death. The latest follow-up point was December 2021.
Statistical analysis
Statistical analyses were carried out by SPSS 20.0 (SPSS Inc., Chicago, IL, USA) and MedCalc v19.0.7 (MedCalc Software Ltd., Ostend, Belgium). The optimal discriminator point of the LCR was calculated by receiver operating characteristic (ROC) curve analysis for OS, and the AUCs of different markers, including the LCR, were then compared. The differences in clinicopathological parameters among subgroups were estimated by chi-square test or Student’s t-test, and the relationship of the liver metastasis and LCR subgroups was tested by Spearman’s correlation coefficient. The DFS and OS differences among the LCR subgroups and risk factors for the outcome were estimated by Kaplan-Meier analysis and the Cox proportional hazards model with iterative forward LR method, respectively. Double-sided P < .05 was considered statistically significant.
Results
Demographic features of the cohort and the prognostic efficacy of LCR
Following the exclusion criteria, a total of 189 patients were collected in the final cohort (Figure 1). The numbers of patients with stage I, II, and III disease were 38, 75, and 76, respectively, and there were 122 men and 67 women. The mean age of the patients was 59.20 (range: 24-85) years, and the mean follow-up time was 52.16 (range: 1-111) m. During the follow-up, 17 patients presented with a single liver metastasis, and 4 patients presented with multiple metastases, including liver metastases. By ROC analysis, the LCR (AUC = 0.80) had a sensitivity and a specificity of 75.60% and 77.00%, respectively, in predicting OS (Figure 2). The prognostic efficacy of the LCR in predicting DFS and OS was then compared with ALC, CEA alone and NLR, LMR, and PNI alone. The results indicated that LCR was superior to single ALC (Z = 2.06, P = .04), CEA (Z = 2.38, P = .02), NLR (Z = 2.45, P = .01), LMR (Z = 2.33, P = .02), and PNI (Z = 2.64, P = .01) in predicting DFS; moreover, it was also better than single ALC (Z = 3.23, P < .01), NLR (Z = 3.84, P < .01), LMR (Z = 3.13, P < .01), and PNI (Z = 2.89, P < 0.01) in predicting OS, but not CEA (Z = 1.49, P = .14).
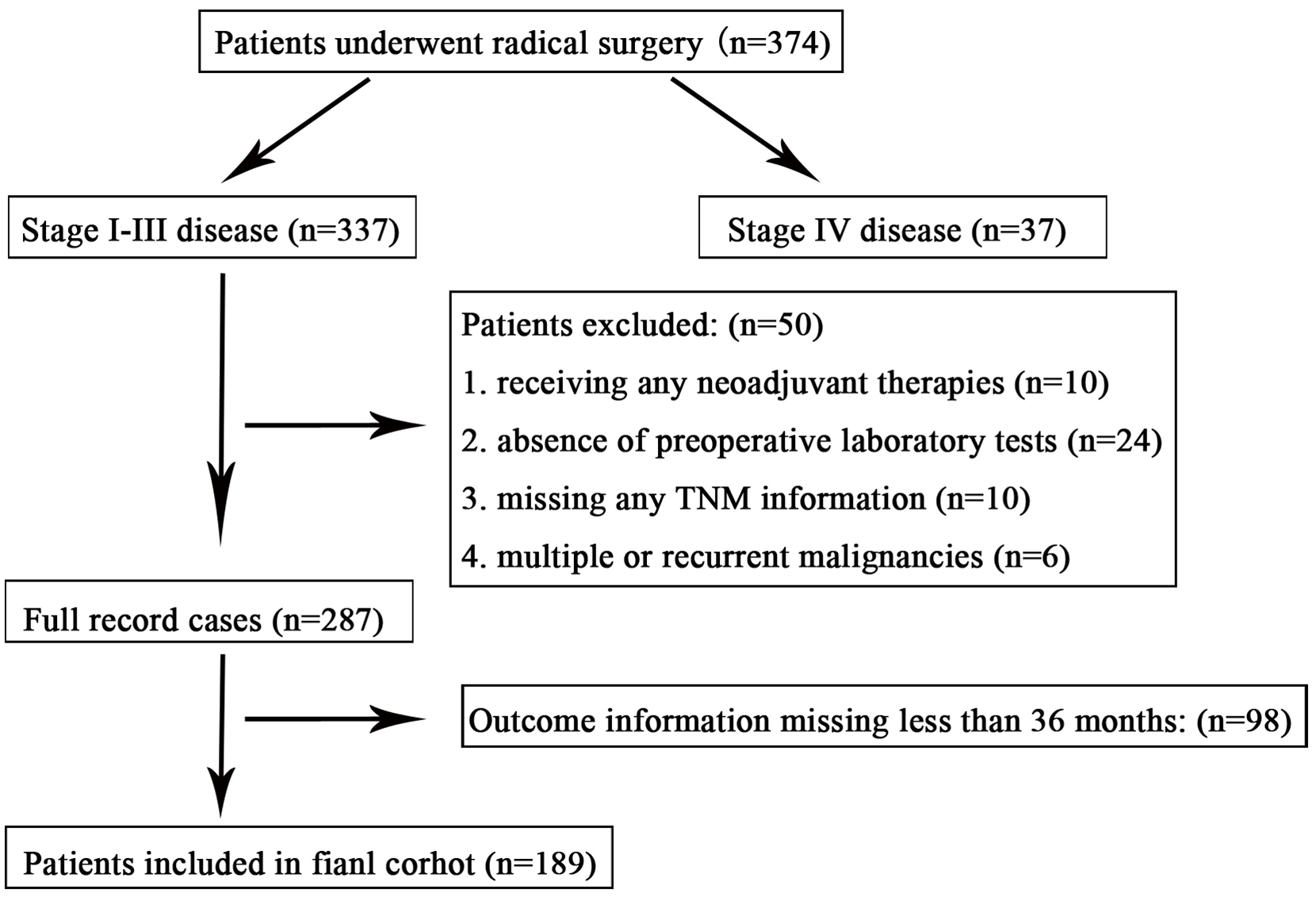
Research flow chart of the study. TNM indicates tumor-node-metastasis.

Results of the ROC analysis of the indicators for DFS (A) and OS (B).
Differences in clinicopathological parameters among LCR subgroups
According to the Youden index from the ROC curves (taking OS as the endpoint), 0.28 was determined as the cutoff point for the low (<.28) or high (⩾.28) LCR subgroups. A total of 34.92% (66/189) of patients displayed a low LCR (<0.28), and these patients were more likely to present poor cell differentiation (P = .03), tumor deposits (P < .01) and advanced T (P < .01) (Table 1). In addition, these patients were more likely to experience subsequent liver metastasis than the high LCR patients (R = −.17, P = .02).
Differences of varied clinicopathological parameters among LCR low or high subgroups.
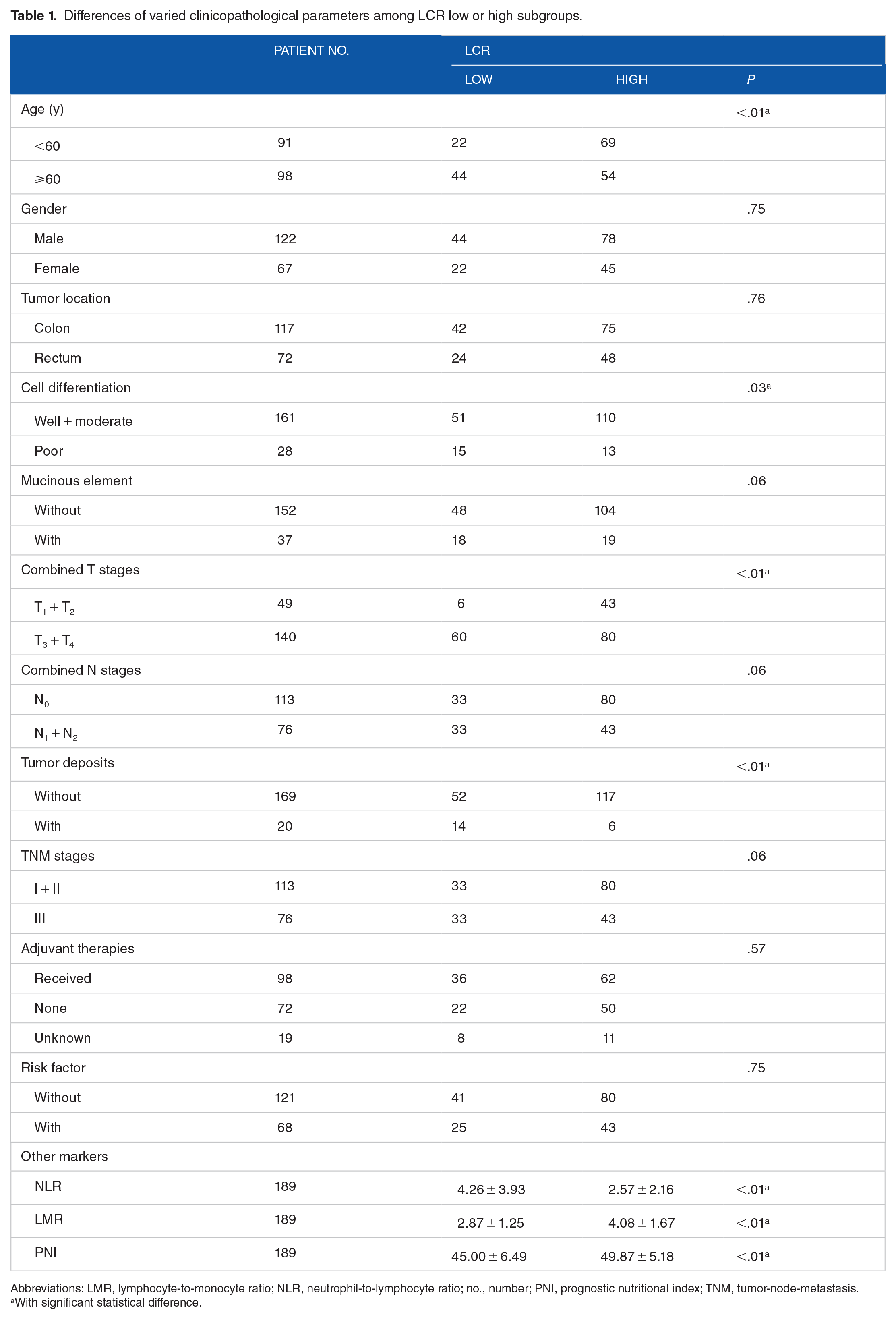
Abbreviations: LMR, lymphocyte-to-monocyte ratio; NLR, neutrophil-to-lymphocyte ratio; no., number; PNI, prognostic nutritional index; TNM, tumor-node-metastasis.
With significant statistical difference.
Survival differences among the LCR subgroups
By Kaplan-Meier analysis, patients with a low LCR presented a significantly inferior DFS (Log Rank = 34.98, P < .01) and OS (Log Rank = 43.17, P < .01) compared with those with a high LCR. Interestingly, such survival differences were maintained in stages I and II and stage III cases (Figure 3). In addition, the 1-, 2- and 3-year DFS (1-year: 71.21% vs. 95.12%, P < .01; 2 years: 54.55% vs. 92.68%, P < .01; 3 years: 51.52% vs. 89.43%, P < .01), and OS (1 year: 89.39% vs. 99.17%, P < .01; 2 years: 74.24% vs. 96.75%, P < .01; 3 years: 62.12% vs. 94.31%, P < .01) rates were significantly different between the low and high LCR subgroups.

Survival difference between the low and high LCR subgroups in terms of DFS and OS: (A) DFS difference in stage I and II patients; (B) DFS difference in stage III patients; (C) DFS difference in stage I-III patients; (D) OS difference in stage I and II patients; (E) OS difference in stage III patients; and (F) OS difference in stage I to III patients.
Univariate and multivariate tests of risk factors for DFS and OS
By univariate tests, the combined T, N, and TNM stages, with or without tumor deposits, adjuvant therapies, NLR, LMR, PNI, and LCR were risk factors for DFS (Table 2), and these factors (except for the adjuvant therapies) plus cell differentiation, with or without mucinous elements, were risk factors for OS (Table 2). When all of these statistically significant factors were entered into multivariate tests for DFS and OS (with those only P < .05), the results indicated that the LCR was one of the independent prognostic factors for both DFS (hazard ratio [HR] = 0.35, 95% confidence interval [CI]: 0.20-0.62, P < .01) and OS (HR = 0.18, 95% CI: 0.08-0.37, P < .01; Table 3).
Univariate analyses of risk factors for DFS and OS.
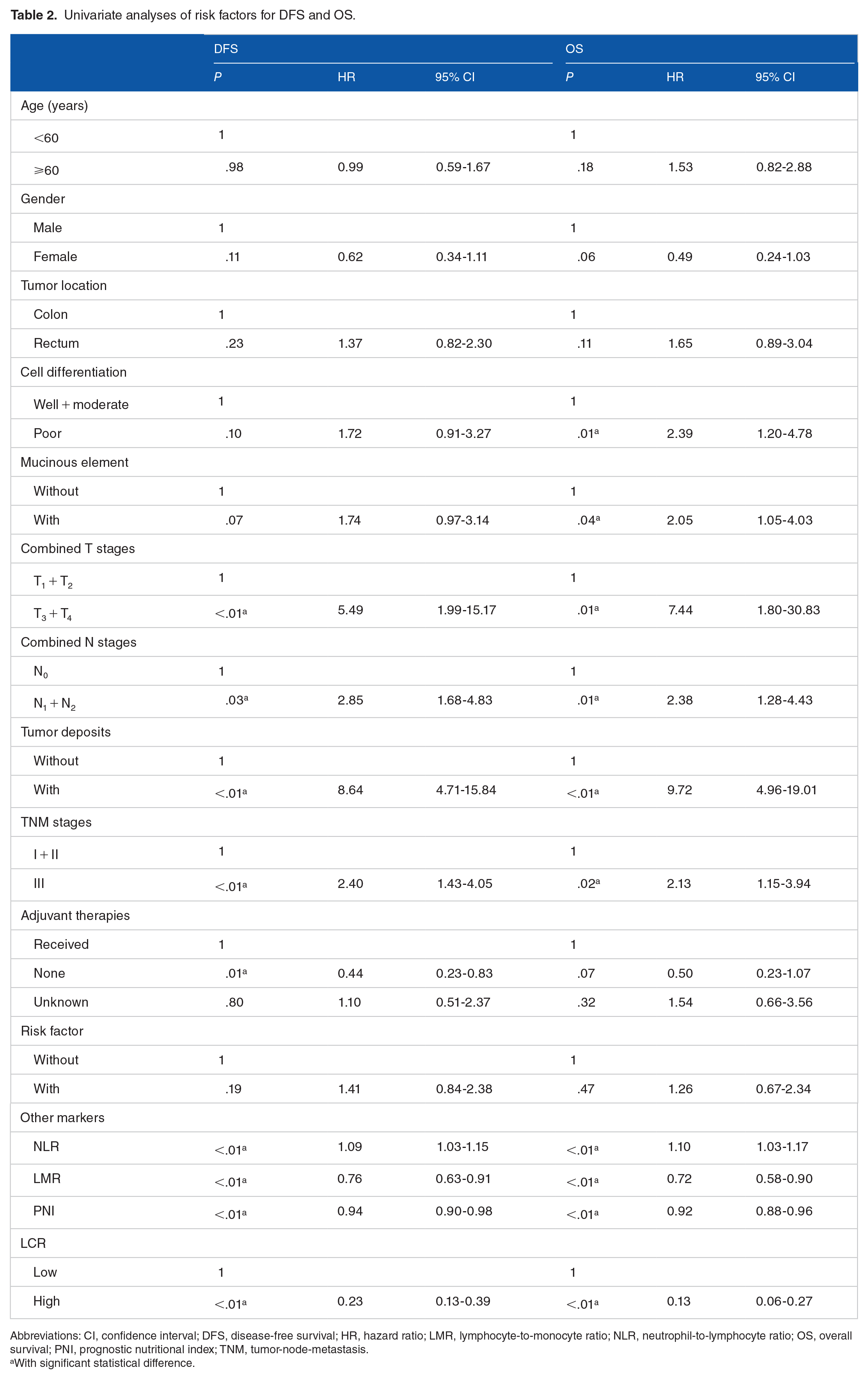
Abbreviations: CI, confidence interval; DFS, disease-free survival; HR, hazard ratio; LMR, lymphocyte-to-monocyte ratio; NLR, neutrophil-to-lymphocyte ratio; OS, overall survival; PNI, prognostic nutritional index; TNM, tumor-node-metastasis.
With significant statistical difference.
Multivariate analyses of risk factors for DFS and OS.

Abbreviations: CI, confidence interval; DFS, disease-free survival; HR, hazard ratio; OS, overall survival.
With significant statistical difference.
Discussion
In this study, the LCR was found to be a superior predictor of survival in stage I to III CRC with a relatively high sensitivity and specificity. The prognostic efficacy of LCR was superior to ALC, CEA, and other markers, including NLR, LMR, and PNI. Patients with a low LCR present a poor outcome and easily experience liver metastasis. To the best of our knowledge, this is the first report concerning the prognostic role of LCR in CRC.
Previously, the prognostic value of ALC and CEA was well established in CRC, but with some limitations. For ALC, Noh et al included 231 stage II and III patients who underwent curative surgery and subsequent adjuvant chemotherapy to examine the role of neutrophil count, ALC, and NLR in predicting the outcome; their results indicated that patients with a low ALC during chemotherapy would have a lower 5-year DFS rate and ALC was an independent prognostic factor for DFS. 11 In line with this, Liang et al 24 enrolled 1332 stage II patients with a similar scenario, among which 459 cases with high risk received adjuvant chemotherapy; their results also suggested that a low ALC in high-risk patients was associated with the worst DFS, and ALC was an independent risk factor for these patients. Nonetheless, the prognostic efficacy of ALC by itself is still insufficient, and its AUC in predicting the outcome ranged from 0.58 to 0.61, with relatively low sensitivity and specificity.10,11 For CEA, Fenqi et al 25 included 1081 stage II patients after radical resection and found that the AUC of CEA in predicting cancer-specific survival was 0.62; similarly, Ming-Sheng et al 26 collected 330 stage I to IV patients who underwent surgery and found that the AUC of CEA in predicting OS was 0.57, with a sensitivity of 35.4%. In addition, when other prognostic markers were included in the analysis, CEA alone was not an independent risk factor for the outcome.27,28 To overcome these limitations, some studies have tried to combine ALC or CEA with other markers; however, such combinations are not conventionally superior to individual ALC or CEA.9,11,29 In our study, the AUC for the LCR was 0.80, with a sensitivity and specificity of 75.60% and 77.00%, respectively, and the AUC comparison indicated that the LCR was more accurate than other markers based on ALC.
It is well known that lymphocytes are the most powerful actors in the adaptive immune system in the anticancer immune response. 30 Although the phenotypes of these cells are heterogeneous, they could exert different roles in regulating the development of cancer. For example, cancer stem cells (CSCs) have been identified in CRC (CCSCs) and they play a fundamental role in multiple aspects, including initiation, progression and metastasis of the disease.3,31 Eradication of these cells is thought to be essential to control or even cure the disease. 32 Notably, it was found that peripheral cytotoxic T lymphocytes (CTLs) could efficiently recognize human CCSCs; 33 in turn, CCSCs would avoid T lymphocyte-mediated killing by reducing MHC-I. 34 In addition, another peripheral subpopulation of lymphocytes, namely, T helper lymphocytes, could synthesize interleukin-12,35,36 which could also inhibit the survival of CCSCs and their tumor initiating capacity. 37 Noticeably, the activity and count of peripheral lymphocytes could also be influenced by cancer cells,38,39 and a negative correlation between CTL activity and cancer cell proliferation has been noted in CRC. 40 Carcinoembryonic antigen is mainly produced by CRC cells, 41 particularly drug-resistant cells. 42 Mechanistically, CEA could promote the development of the disease by regulating EMT or increasing cell invasiveness and preventing cell apoptosis; 21 in addition, CEA could contribute to the radioresistance of cancer cells. 43 Based on these facts, it is plausible that a low LCR in CRC would reflect an impaired recognition or elimination of CCSCs and the probability of a high number of drug-resistant cancer cells with a tendency to become more aggressive, which would not surprisingly result in a poor outcome. In addition, taking into consideration, the important role of CCSCs in liver metastasis44,45 and the role of CEA in cancer progression,21,43 it is also believable that patients with a low LCR could more easily develop liver metastasis.
In addition, patients with a low LCR are also characterized by poor cell differentiation and tumor deposits, which are notorious indicators of poor survival in CRC. For example, Bagante et al 46 reported that poorly differentiated cases would be more common in mucinous or signet-cell adenocarcinoma, which correlated with worse survival. Wuxiao et al 47 indicated that in stage III patients, those with poorly differentiated histology would have poor OS. In addition, Cohen et al 48 conducted a post hoc analysis of patients in the CALGB/SWOG80702 trial and found that when tumor deposits were counted as metastatic nodes, 7.1% of N1 cases would be elevated to N2, and the 3-year DFS and 5-year OS rates of these patients were worse than those of N1 cases. Furthermore, Lino-Silva et al 49 performed a study including 392 patients and found that stage I to III patients with tumor deposits would behave similarly to stage IV patients, and these patients were also less likely to benefit from adjuvant chemotherapy. 50 Interestingly, patients with poor cell differentiation or tumor deposits would have an elevated CEA,46,47,51 and it is plausible that these cases would be more apt to present a low LCR. Notably, a low LCR was also accompanied by a high NLR and a low LMR and PNI in our study. These indicators are well-established prognostic markers, as a group of systematic reviews and meta-analyses indicated that high NLR or low LMR and PNI correlated with poor OS in CRC.52–57 All of these results support that patients with a low LCR would have a poor outcome.
There are several limitations to our study. First, it was a retrospective study with a relatively small sample, and the results could be biased by other confounding factors. Second, at least half of the patients in our cohort received adjuvant chemotherapies (as indicated in Table 1). It is well known that chemotherapy would have a profound effect on ALC9,24 and thus could influence the significance of LCR in these cases. Third, the phenotypes of peripheral lymphocytes were heterogeneous with different or even opposite functions in controlling the development of the disease, and it would be more sound to identify a specific subpopulation of these cells and examine the role of LCR in CRC.
Conclusion
Overall, our study found that compared with other markers based on preoperative ALC, the LCR was a superior predictor of survival in stage I to III CRC, and patients with a low LCR have an inferior outcome. However, taking into consideration the limitations of our study, more studies with larger samples are needed to validate these results in the future.
Research Data
sj-xlsx-1-onc-10.1177_11795549221126249 – Supplemental material for Preoperative Absolute Lymphocyte Count to Carcinoembryonic Antigen Ratio Is a Superior Predictor of Survival in Stage I to III Colorectal Cancer
Supplemental material, sj-xlsx-1-onc-10.1177_11795549221126249 for Preoperative Absolute Lymphocyte Count to Carcinoembryonic Antigen Ratio Is a Superior Predictor of Survival in Stage I to III Colorectal Cancer by Yue Zhou, Fei Cheng, Zihao Zhang, Jia Xiang, Tianhui Xue, Qianwen Ye and Bing Yan in Clinical Medicine Insights: Oncology
Footnotes
Acknowledgements
The authors would like to express their sincere appreciation to Prof. Xiutang Cao (Institute of Management, Chinese PLA General Hospital, Beijing) and Dr. Hewei Zhang (Department of Health Statistics, Naval Medical University, Shanghai) for the constructive suggestions and check for the statistical results of our work.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
BY was responsible for the conception of the work. YZ, FC, ZZ, JX, TX, and QY obtained the data. BY analyzed the data. YZ, FC, ZZ and BY wrote the manuscript. JX, TX, QY and BY critically revised the manuscript. All authors are accountable for the contents of this work. The authors read and approved the final manuscript.
Availability of Data and Materials
The data sets generated or analyzed during this study are available from the corresponding author on reasonable request.
Ethical Approval
This study was supervised and approved by the ethics committee of Hainan Hospital of Chinese PLA General Hospital (ID: 301HLFYLS15) and conducted in accordance with the principles stated in the Declaration of Helsinki; informed consent was obtained from the patients or their authorized relatives.
Consent for Publication
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.