
Abstract
Patients from Asia with non-small-cell lung cancer (NSCLC) often have mutations in the epidermal growth factor receptor (EGFR) gene. While an increasing number of EGFR tyrosine kinase inhibitors (TKIs) are now available for patients with EGFR mutation-positive NSCLC, most patients inevitably develop resistance to the treatment. Evidence from clinical studies suggests that treatment outcomes and resistance mechanisms vary depending on the choice of TKI therapy in the first-line setting. Hence, it is important to develop optimal treatment sequencing strategies that can provide maximum survival benefit for the patient. In this review we present clinical evidence in Asian patients with NSCLC for various EGFR TKIs, with the goal of supporting the optimization of treatment sequencing.
Epidemiology of EGFR Mutation-Positive NSCLC in Asia
In Asia, lung cancer is a rapidly growing healthcare problem, with China currently the epicenter. Every year, approximately 1.31 million individuals (about 60% of the global incidence) in Asia are diagnosed with lung cancer, of which about 0.8 million new cases are from China.1,2 Asians with non-small-cell lung cancer (NSCLC) are more likely to have mutations in the epidermal growth factor receptor (EGFR) gene. A pooled analysis of 456 studies showed that about 32% of patients with NSCLC have EGFR mutations; however, there is a striking difference between Asians and non-Asians for the prevalence of EGFR mutation-positive NSCLC, whereby 38% (95% confidence interval [CI]: 36.5-40.3) of patients with NSCLC in Asia harbor EGFR mutations, compared with 24% (95% CI: 22.1-26.8) in the America (North and South) and 14% (95% CI: 12.7-15.5) in Europe. 3 The prevalence of EGFR mutations also differs by tumor histology, with about 50% of Asian patients with adenocarcinomas having EGFR mutations compared with 14% of patients with non-adenocarcinomas.3 -5 Within East and Southeast Asia, the prevalence of EGFR-mutation-positive adenocarcinoma cases ranges from 47.2% in Hong Kong to 64.2% in Vietnam. 5 About half of the patients with adenocarcinoma in China carry an EGFR mutation (50.2%). 5 Global and regional guidelines recommend screening of all patients with advanced lung adenocarcinomas for EGFR mutations, along with other mutations, regardless of their clinical characteristics.
EGFR Mutations and Targeted Therapy in Asia
The EGFR gene, which is situated on the short arm of chromosome 7, is considered one of the important driver genes that determine the carcinogenesis of lung adenocarcinoma.6 -8 The transmembrane growth factor receptor encoded by the gene exhibits tyrosine kinase (TK) activity. On binding of extracellular ligands, the EGFR forms homodimers or heterodimers with members of the ErbB family, activating the cytoplasmic TK domain. Downstream EGFR signaling is crucial to cellular growth and differentiation under physiological conditions.8,9 However, somatic mutations leading to EGFR overexpression contribute to tumor progression by increasing proliferation, angiogenesis and metastasis, and decreasing apoptosis. 10
For Asian patients with NSCLC and adenocarcinoma histology, the most common types of EGFR mutations include exon 19 deletions (Ex19del) and exon 21 (Ex21) L858R substitutions, accounting for 85% to 90% of all TK domain mutations.3 -5, 11 Other uncommon mutations or double mutations are reported in about 4% of patients. EGFR mutations resistant to certain tyrosine kinase inhibitor (TKI) therapies, such as T790M, or exon 20 insertions (Ex20Ins), are also reported in treatment-naive patients, though at a very low frequency (~3% of patients).3 -5 Furthermore, a minority of patients (about 2%) also report a combination of sensitizing and resistant EGFR mutations. Despite wide differences in EGFR mutation prevalence between Asians and Caucasians, the 2 most common EGFR mutations in these regions remain the same, namely Ex19del and L858R in Ex21.3 -5
Therapies targeting these EGFR mutations have been the mainstay of treatment. In the frontline treatment of patients with EGFR mutation-positive NSCLC, eight EGFR TKIs are available across three therapeutic generations.12,13 First-generation therapies such as gefitinib, erlotinib, and icotinib reversibly block the TK domain, and have been shown to improve progression-free survival (PFS) over chemotherapy; however, patients inevitably develop resistance to these molecules. Thus, the second-generation molecules, afatinib and dacomitinib, were designed to irreversibly block the TK domain of EGFR with a broad activity extending to other ErbB family receptors and certain EGFR mutations. Afatinib has also been shown to be effective against some uncommon mutations. The three third-generation agents, osimertinib, almonertinib, and alflutinib, are irreversible TKIs with activity against certain EGFR mutations, specifically the T790M mutation. 12
In a recent review, Kim et al 14 examined the clinical evidence of EGFR TKIs in Asians and non-Asians with NSCLC harboring EGFR mutations. Multiple Phase III trials comparing first- and second-generation EGFR TKIs with chemotherapy established these TKIs as standard-of-care in EGFR-mutated advanced NSCLC, showing comparable efficacy for Asian as well as non-Asian patients.15 -25 Despite improved PFS, overall survival (OS) was comparable between the first-generation EGFR TKIs versus chemotherapy (Table 1).15 -19 Conversely, the second-generation EGFR TKIs showed a significant OS benefit over chemotherapy, specifically in patients with Ex19del mutations (median OS: 31.4-33.3 months with afatinib vs 18.4-21.1 months with chemotherapy; Table 1).21 -24 Similarly, dacomitinib was associated with improved OS compared with gefitinib (overall population: 34.1 months vs 27 months; data for the Asian subgroup are presented in Table 1).25,26 In addition, osimertinib has been approved for frontline treatment of EGFR-mutated advanced NSCLC based on its superior PFS over gefitinib/erlotinib.27 -30 Almonertinib and alflutinib are also approved in China in the second line if progression occurred after treatment with other EGFR TKIs.
Summary of randomized controlled trials on EGFR TKIs in patients from Asia.

Abbreviations: CI, confidence interval; EGFR, epidermal growth factor receptor; HR, hazard ratio; NR, not reached; ORR, overall response rate; OS, overall survival; PFS, progression-free survival; TKI, tyrosine kinase inhibitor.
The Pan-Asian adaptation of the European Society for Medical Oncology (ESMO) guidelines, which was developed in collaboration with Asian oncological societies from China (Chinese Society of Clinical Oncology), Japan (Japanese Society of Medical Oncology), Korea (Korean Society of Medical Oncology), Taiwan (Taiwan Oncology Society), Malaysia (Malaysian Oncological Society), and Singapore (Singapore Society of Oncology), recommended first-line therapy with EGFR TKIs with no preference for any particular therapy. 13 In the second-line setting, the guidelines recommend osimertinib for patients testing positive for EGFR T790M mutation, or those with central nervous system disease. Of note, the first-generation EGFR TKIs are reimbursed in all the participating countries, whereas afatinib is reimbursed in all countries except Malaysia. Osimertinib is reimbursed only in China, Japan, and Korea. 13
The treatment landscape for NSCLC has evolved substantially over the past few decades. With the availability of several targeted treatments, there is substantial improvement in survival, making NSCLC a chronic disease that patients can survive over years rather than months. Patients also understand the need for multiple lines of targeted therapies as the tumor eventually mutates. 43 However, there are limited data from randomized controlled trials (RCTs) examining the efficacy of sequential EGFR TKI therapy in NSCLC; therefore, real-world studies can be used to bridge the evidence gap for sequential treatment. Real-world studies have the additional advantage of including patients with adverse prognostic factors (the elderly, uncommon EGFR mutations, poor performance status, or comorbid conditions) that are not typically included in clinical trials.
Here we review different sequential EGFR TKI treatment options in the first- and second-line settings based on efficacy and resistance profiles, whilst providing new insights into optimal sequencing strategy for patients with NSCLC harboring EGFR mutations.
First-Line EGFR TKIs Have Variable Efficacy in Asian Patients With NSCLC Harboring EGFR Mutations
Efficacy of different EGFR TKIs in the first-line setting
Evidence from multiple RCTs and real-world studies suggests that Asian patients with EGFR-mutant NSCLC experience different outcomes depending on the TKI therapy received at first-line setting. In this section we review outcomes in patients from Asia following treatment with different first-line TKI therapies.
It has been established from Phase III clinical trial results that first- and second-generation EGFR TKIs provide significantly longer PFS compared with chemotherapy in Asians with EGFR-mutated NSCLC. Although no benefit in OS was observed with first-generation TKIs,15 -17 second-generation TKIs improved both PFS and OS when compared to chemotherapy (Table 1).21,22,25 Median OS in a subgroup analysis of the LUX-Lung 3 study in Japanese patients was higher with afatinib than chemotherapy (46.9 vs 35.8 months; hazard ratio [HR]: 0.75, 95% CI: 0.40-1.43), with a significant difference observed for patients with Ex19del mutations (46.9 vs 31.5 months; HR: 0.34, 95% CI: 0.13-0.87). 36 Similarly, in a subgroup analysis of the LUX-Lung 6 trial in Chinese patients with NSCLC (Table 1), afatinib treatment was associated with a significant OS benefit in patients with Ex19del mutations (31.6 vs 16.3 months; HR: 0.61, 95% CI: 0.41-0.91). 24
The next key question was whether second-generation EGFR TKIs provided greater PFS benefit than first-generation TKIs. Afatinib and gefitinib were compared in a global population in the Phase IIb LUX-Lung 7 trial, where patients from Asia accounted for 59% of the population.37,38 The study demonstrated the superiority of afatinib over gefitinib in terms of PFS (HR: 0.73, 95% CI: 0.57-0.95), with similar effects in Asian and non-Asian patients (HR: 0.76 vs 0.72; Table 1); the PFS benefit was sustained even after a longer median follow-up of 42.6 months (HR: 0.74, 95% CI: 0.57-0.95).37,38 Similarly, in the Phase III ARCHER 1050 study in a global cohort that comprised 75% Asian patients, dacomitinib was associated with an improved PFS (global cohort: 14.7 vs 9.2 months; HR: 0.59, 95% CI: 0.47-0.74) and OS (global cohort: 34.1 vs 27.0 months; HR: 0.75, 95% CI: 0.59-0.95) compared with gefitinib, with similar effects observed for Asian and non-Asian subgroups.25,26
The third-generation TKI, osimertinib, was compared with either gefitinib or erlotinib in the FLAURA trials. In the Asian subgroup analysis (N = 322), median PFS was significantly improved with osimertinib compared with the first-generation TKIs (Asian subgroup: 16.5 vs 11.0 months; HR: 0.54, 95% CI: 0.41-0.72; P < 0.0001; Table 1). 30 The PFS benefit of osimertinib over erlotinib/gefitinib was less pronounced in Asian compared with non-Asian patients in the overall FLAURA trial (non-Asian subgroup: HR: 0.34, 95% CI: 0.23-0.48). 28 Similarly, in a Japanese subanalysis of FLAURA, PFS benefit of osimertinib over erlotinib/gefitinib did not appear to be as pronounced as for the overall population (HR: 0.46, 95% CI: 0.37-0.57) owing to a stronger PFS in the comparator arm (median: 19.1 vs 13.8 months; HR: 0.61, 95% CI: 0.38-0.99). However, the OS was lower with osimertinib compared with erlotinib/gefitinib; median OS was 39.3 months in the osimertinib group whereas it was not reached in the erlotinib/gefitinib group.41,42 In the FLAURA China study, osimertinib was associated with significantly longer PFS compared with erlotinib/gefitinib (17.8 vs 9.8 months; HR: 0.56, 95% CI: 0.37-0.85). Median OS was comparable in the osimertinib and erlotinib/gefitinib groups (33.1 vs 25.7 months; HR: 0.85, 95% CI: 0.56-1.29; Table 1). 29
Overall, the EGFR TKIs have demonstrated remarkable benefits in response rates compared with chemotherapy. A recently published network meta-analysis compared response rates of different EGFR TKIs in the first-line setting, relative to chemotherapy. 44 This pooled analysis of RCTs demonstrated that patients receiving EGFR TKIs are 4.5-times more likely to have an objective response than with chemotherapy (odds ratio [OR]: 4.49, 95% CI: 3.16-6.37). Among different EGFR TKIs, afatinib was ranked first in terms of response rates, with an OR of 5.69 (95% CI: 3.40-9.54) compared with chemotherapy. 44
Several real-world studies have evaluated the efficacy of EGFR TKIs, particularly first- and second-generation TKIs, in the first-line setting for Asian patients with NSCLC.45 -49 Afatinib consistently showed superior PFS in comparison to gefitinib or erlotinib, consistent with results from RCTs. Furthermore, the superior efficacy of afatinib compared with gefitinib or erlotinib was consistent in patients with or without brain metastasis, as well as in those with common mutations, Ex19del and Ex21 L858R mutations. Some of the key studies with a large sample size are summarized here.
In a retrospective study of 448 patients enrolled in Taiwan between 2011 and 2015, afatinib therapy demonstrated a significantly higher PFS compared with gefitinib (median PFS not reached vs 11.4 months; HR: 0.51, 95% CI: 0.34-0.78; P < 0.001). 49 These effects were consistent across patients with Ex19del (HR: 0.54, 95% CI: 0.32-0.90) and Ex21 L858R (HR: 0.38, 95% CI: 0.18-0.80) mutations. Furthermore, in a retrospective study of Korean patients who had received EGFR TKIs between 2014 and 2016 (N = 467), median PFS was significantly higher for afatinib versus gefitinib and erlotinib (19.1 vs 13.7 and 19.1 vs 14.0 months, respectively; P = 0.001). 48 The superior PFS with afatinib was more remarkable in subgroups of Ex19del (19.1 vs 15.0 vs 16.3 months, respectively; P = 0.01) or uncommon EGFR mutations (not reached vs 5.0 vs 6.1 months; P = 0.06). 48 In another retrospective study of patient data collected at Mackay Memorial Hospital (Taiwan) between 2013 and 2017 (N = 176), afatinib was associated with a significantly better PFS compared with first-generation TKIs (HR: 0.64, 95% CI: 0.42-0.97, P = 0.036). 50
Multiple real-world studies have reported the effects of first- and second-generation EGFR TKIs on time to treatment failure (TTF). A retrospective analysis of outcomes in patients with NSCLC presenting at a tertiary hospital in Taiwan from 2011 to 2016 (N = 853) showed a significantly higher TTF with afatinib compared with gefitinib (16.1 vs 11.5 months; HR: 0.54, 95% CI: 0.41-0.71) and erlotinib (16.1 vs 11.7 months; HR: 0.62, 95% CI: 0.46-0.83). 46 The superior TTF benefit with afatinib was consistent in patients with Ex19del (18.2 vs 11.1 vs 11.9 months; P = 0.003) and Ex21 L858R (16.1 vs 12.0 vs 11.4 months; P = 0.187) mutations. In addition, the TTF benefit of afatinib over gefitinib was consistent in patients with (HR: 0.45, 95% CI: 0.29-0.70) or without (HR: 0.61, 95% CI: 0.43-0.87) brain metastasis. 46 Another large retrospective study of the Taiwan Cancer Registry that included 5940 patients receiving EGFR TKIs between 2011 and 2015 demonstrated a significantly higher TTF with afatinib compared with gefitinib (15.8 vs 11.9 months; P < 0.001) and erlotinib (15.8 vs 12.7 months; P < 0.001). 47 Similar results were reported from a multicenter study that enrolled consecutive Japanese patients receiving EGFR TKIs between 2008 and 2017 (N = 1366). 45 After propensity score matching, median TTF was significantly higher with afatinib compared with first-generation TKIs (14.4 vs 10.6 months; HR: 0.793, 95% CI: 0.722-0.872; P < 0.0001), which was consistent in those with Ex19del (HR: 0.864, 95% CI: 0.754-0.990; P = 0.0348) and Ex21 L858R (HR: 0.834, 95% CI: 0.716-0.971; P = 0.0192) mutations, or brain metastasis (HR: 0.765, 95% CI: 0.639-0.915; P = 0.0034). 45
Clonal selection and resistance profiles
With the availability of next-generation sequencing (NGS) platforms and other technological advances, it is now possible to track tumor mutations over time, as well as to distinguish clonal and subclonal events. Emerging evidence suggests that NSCLC tumors with EGFR mutations are highly heterogeneous, with multiple types of EGFR mutations occurring within a single tumor, as well as other co-occurring alterations in other oncogenic pathways, such as WNT (CTNNB1), cell cycle (CDK6), epigenetic (MYC), hormone signaling (AR), and PI3K (PIK3CA).51 -53 Notably, the clonal nature of tumor evolution implies that any targeted therapy or chemotherapy may enable emergence of resistant tumor cells or mutations with unique molecular characteristics. 54
Patients who receive EGFR TKI therapy eventually develop acquired resistance to therapy. Emergence of T790M mutation is the most commonly reported resistance mechanism following treatment with first- and second-generation EGFR TKIs, occurring in about 38% to 63% of patients from Asia (gefitinib: 35%-62%; erlotinib: 44%-67%; icotinib: 29%-51%; afatinib: 41%-75%).55 -65 Certain initial EGFR mutations are strong predictors for the subsequent development of T790M resistance. Among Asian patients with Ex19del EGFR mutations, around 52% to 64% develop T790M mutation following first- or second-generation TKIs,55,57,59,60,62,66 whereas the corresponding rate in those with Ex21 L858R EGFR mutations ranges between 37% and 45%. These observations paved way for the third-generation TKI therapies (eg, osimertinib), which selectively block the T790M EGFR variant. Predictably, osimertinib as second-line therapy demonstrated PFS benefit and high response rates in patients with T790M-positive tumors following first- and second-generation EGFR TKIs. 67
While EGFR T790M mutation is most often detected in patients who progressed on first-line TKI therapy, evidence suggests that T790M mutant clones may coexist with the wild-type clone in a small proportion of treatment-naive patients.68 -71 This suggests that one of the possible mechanisms underlying the emergence of T790M is the selective pressure induced by the therapy. Conversely, T790M may evolve gradually from de novo events in the resistant tumor cells with heterogeneous co-occurring genetic alterations. 72 In a genomic analysis of 1122 EGFR mutation-positive NSCLC samples, Blakely et al 53 showed that T790M mutation-positive samples had a higher number of co-occurring genetic alterations compared with T790M mutation-negative samples. Studies examining the clonal evolution paths during EGFR TKI (gefitinib) therapy showed 2 distinct types of T790M mutation-positive clones, which corresponds with the proposed mechanisms: (a) T790M mutant clones emerging early, suggesting coexisting mutant clones at baseline, and b) T790M mutant clones emerging late, suggesting de novo mutation acquired during TKI treatment.73,74 These observations may affect clinical outcomes of EGFR TKIs in the first- and second-line settings. In general, homogeneous T790M clones are more sensitive to the third-generation TKIs, with a higher chance for an enduring response. 67 ,75 -79 The use of EGFR TKIs with a narrow spectrum of activity in first line may lead to expansion of multiple resistant mutations, resulting in heterogeneous tumors that are difficult to treat. Conversely, EGFR TKIs with a broad spectrum of activity in the first-line setting may suppress multiple mutations and result in the emergence of a more homogeneous resistant tumor, with a more predictable response to subsequent lines of therapy.77 -79 Among different EGFR TKIs available, afatinib exhibited a broad spectrum of activity against EGFR mutations, including various uncommon mutations.80 -82 In addition, afatinib has shown to induce more homogeneous T790M clones compared with first-generation TKIs; thus, improving the likelihood of an enduring response to subsequent treatment with third-generation TKIs. 83
The resistance mechanisms following osimertinib therapy are diverse and include on-target EGFR mutations such as C797, L792, and L718 substitution mutations or loss of T790M mutation, co-occurring genetic aberrations such as PI3KCA, MEK1, JAK2, and HER2 or amplification of KRAS, MET, or EGFR, and transformation to small-cell or squamous-cell histology.84 -88 In addition, an analysis of cell-free DNA from NSCLC tumor samples identified MAPK-, PI3K- and WNT-pathway mutations as potential drivers of primary resistance to osimertinib. 53 Following treatment failure with osimertinib, patients usually receive chemotherapy due to the lack of clear targeted therapy options as a result of the highly heterogeneous resistance mechanisms. Recently, Schoenfeld et al 89 characterized the resistance mechanisms following osimertinib therapy in first-line versus later-line settings, using tumor samples before treatment initiation and following progression. The analysis showed different resistance profiles following osimertinib therapy in these settings; in first line it resulted in early emergence and high frequency of co-occurring aberrations (19%; MET amplification, BRAF fusion, RET fusion, KRAS mutation) and histological transformation (15%), whereas EGFR-mediated resistance mechanisms were uncommon (4%). 89 In addition, 59% of samples had an unknown mechanism of resistance following osimertinib in the first-line setting; conversely, in the cohort with later-line osimertinib therapy, 71% had an established mechanism of resistance. A C797S or C797G mutation was found in 29% of cases. Analysis of clinical outcomes revealed that patients receiving osimertinib in later lines had a significantly longer time to treatment discontinuation (18.0 vs 13.2 months; P = 0.04) and OS (not reached vs 29 months; P < 0.001), compared with those treated in the first-line setting. 89
Taking clonal evolution into consideration, the resistance outcomes of patients can be controlled through appropriate sequencing of EGFR TKIs. Therefore, evaluation of molecular and genetic characteristics at baseline is highly valuable in guiding the selection of first-line therapy that is most effective in delaying the onset of resistance, as well as in the identification of appropriate therapy following progression.
Optimizing Treatment Sequencing in EGFR Mutation-Positive NSCLC
With the approval of all 3 generations of EGFR TKIs for the frontline treatment of NSCLC, clinicians face the complex challenge of utilizing these agents to achieve maximum clinical benefit, and to delay the need for chemotherapy. As the ultimate goal of therapy is to prolong OS, it is important that there are effective EGFR TKIs available beyond the first-line setting; therefore, optimal sequencing of EGFR TKIs is crucial in achieving the best possible survival outcomes.
Based on available evidence from head-to-head clinical trials and real-world evidence in patients from Asia, second-generation EGFR TKIs, notably afatinib, are evidently superior to first-generation EGFR TKIs when used as first-line therapy. However, data on the comparative efficacy of second- and third-generation TKIs are lacking. In the absence of clinical trial data, understanding molecular mechanisms of acquired resistance is crucial to determine the optimal sequence strategy that would yield maximum benefit. The clonal nature of tumor evolution in response to therapy could be utilized to achieve predictable resistance outcomes following first-line therapy. First- and second-generation EGFR TKIs are associated with very well characterized mechanisms of resistance, with T790M being the predominant mechanism, occurring in 38% to 63% of Asian patients. In addition, third-generation EGFR TKIs are highly effective against these mutations. 67 In the Phase III AURA3 trial, osimertinib as second-line therapy demonstrated a significantly longer PFS (HR: 0.30, 95% CI: 0.23-0.41; P < 0.001) and better response rates (OR: 5.39, 95% CI: 3.47-8.48; P < 0.001), compared with chemotherapy in patients with T790M mutation-positive NSCLC who had received prior EGFR TKI therapy. 67
Based on the available evidence, it appears that the maximum net survival benefit could be achieved for approximately 38% to 63% of Asian patients with NSCLC who acquire T790M-mediated resistance by using osimertinib in the second-line setting. In terms of predictors for the emergence of T790M-mediated resistance, patients with Ex19del mutations demonstrated a 1.5-fold higher likelihood of acquiring T790M resistance compared with those possessing Ex21 L858R mutations.90 -92 Therefore, using a treatment sequence strategy with afatinib as the first-line therapy followed by osimertinib could provide the best possible survival benefit for patients with NSCLC with EGFR Ex19del mutations. This is supported by evidence from real-world studies, as well as post-progression analysis from the LUX-Lung trials. Here, it is noteworthy that the benefits of this strategy should be weighed against its safety and tolerability profile, such as the higher incidence of diarrhea and rash with afatinib and prolonged QT interval with osimertinib.93 -95
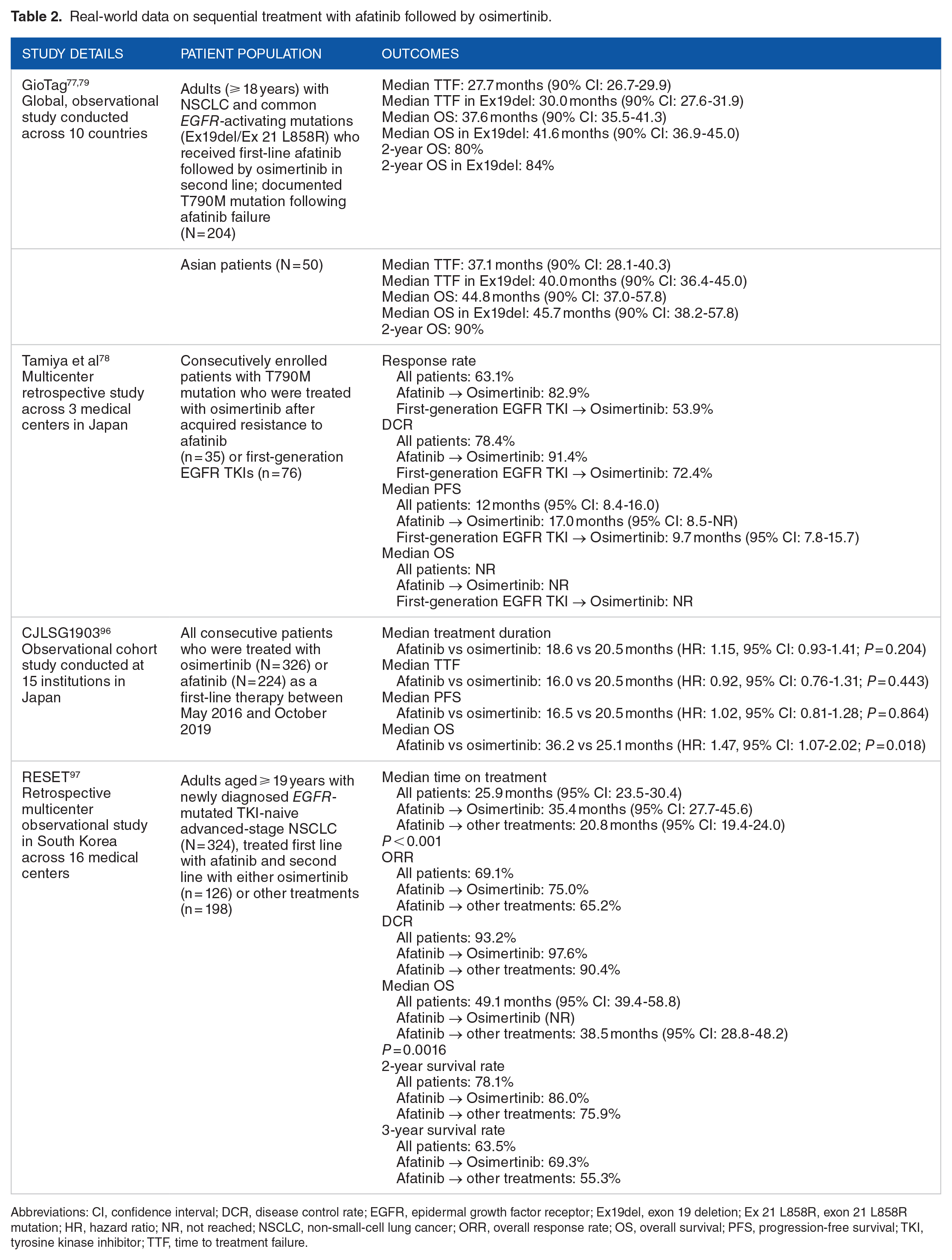
A post-progression analysis of the LUX-Lung 3, 6, and 7 trials identified 37 patients who received osimertinib as subsequent therapy, including 10 patients in second line. 76 In these 37 patients, first-line treatment with afatinib resulted in a median PFS of 21.9 months, and the median duration of subsequent osimertinib therapy was 20.2 months. Following 4.7 years of follow-up, median OS for these patients was not reached. 76 In another post-progression analysis of the LUX trials, a subset of patients (~10%-12%), predominantly women and with Ex19del mutations, demonstrated long-term response with a median PFS of 49.5, 55.5, and 42.2 months in LUX-Lung 3, 6, and 7, respectively. 75 Real-world studies have also demonstrated the effectiveness of sequential afatinib and osimertinib treatment (Table 2).77 -79 A global observational study, GioTag, assessed the outcomes in T790M-positive patients (N = 204) treated with sequential afatinib and osimertinib. For the patients from Asia (n = 50), median time on treatment was 37.1 months (90% CI: 28.1-40.3), and in 31 Asian patients with Ex19del-positive tumors, median time on treatment was 40.0 months (90% CI: 36.4-45.0). Overall, median OS was 37.6 months (90% CI: 35.5-41.3) with a 2-year survival rate of 80%.77,79 Outcomes were particularly encouraging in the Asian group (median OS: 44.8 months, 90% CI: 37.0-57.8), as well as Asian patients with Ex19del-positive tumors (median OS: 45.7 months, 90% CI: 38.2-57.8; Table 2).77,79 Similarly, in a Japanese study, Tamiya et al 78 retrospectively evaluated the outcomes in patients treated sequentially with afatinib and osimertinib (n = 35) versus those treated sequentially with erlotinib/gefitinib and osimertinib therapy (n = 76). Notably, the response rate to osimertinib was significantly higher in patients who had received afatinib previously, compared with those who had received erlotinib/gefitinib (83% vs 54%; P = 0.0065), and there was a trend toward improved PFS in the afatinib group (17.0 vs 9.7 months). Median OS was not reached in either group. 78
Real-world data on sequential treatment with afatinib followed by osimertinib.
Abbreviations: CI, confidence interval; DCR, disease control rate; EGFR, epidermal growth factor receptor; Ex19del, exon 19 deletion; Ex 21 L858R, exon 21 L858R mutation; HR, hazard ratio; NR, not reached; NSCLC, non-small-cell lung cancer; ORR, overall response rate; OS, overall survival; PFS, progression-free survival; TKI, tyrosine kinase inhibitor; TTF, time to treatment failure.
Ito et al 96 conducted an observational cohort study that enrolled consecutive Japanese patients receiving first-line osimertinib or afatinib therapy between May 2016 and October 2019 (N = 554; Table 2). After propensity score adjustment, there were no significant differences in treatment duration between the afatinib and osimertinib groups (median treatment duration: 18.6 vs 20.5 months; HR: 1.146, 95% CI: 0.929-1.414). Median PFS (16.5 vs 20.5 months; HR: 1.02, 95% CI: 0.81-1.28) and TTF (16.0 vs 20.5 months; HR: 0.92, 95% CI: 0.76-1.13) were also comparable between the two groups. However, OS was significantly longer in the afatinib versus osimertinib group (36.2 vs 25.1 months; HR: 1.47, 95% CI: 1.07-2.02; P = 0.018). Median OS was significantly higher with afatinib vs osimertinib for patients with Ex21 L858R mutation-positive tumor without brain metastasis (HR: 2.31, 95% CI: 1.01-5.30; P = 0.047). 96
The retrospective, multicenter, observational study, Real-world experience of sequential treatment of afatinib and osimertinib (RESET), was conducted across 16 medical centers in South Korea (Table 2). 97 The study examined medical records from October 2014 to 2019 for newly diagnosed patients with NSCLC who had received first-line afatinib, and second-line therapy with either osimertinib (n = 126) or chemotherapy regimens (n = 198). Median overall time on treatment for patients receiving sequential afatinib and osimertinib was significantly higher compared with those receiving sequential afatinib and chemotherapy (35.4 months [95% CI: 27.7-45.6] vs 20.8 months [95% CI: 19.4-24.0]; P < 0.001). Median OS was not reached in patients receiving sequential afatinib and osimertinib treatment compared with patients receiving sequential afatinib and chemotherapy (median OS: 38.5 months; P = 0.0016). Similarly, 2- and 3-year survival rates were significantly higher in the afatinib/osimertinib sequential treatment group compared with the afatinib/chemotherapy group (2 years: 86.0% vs 75.9%; 3 years: 69.3% vs 55.3%). 97
While EGFR T790M mutation is the most commonly reported acquired resistance, several other resistance mechanisms are observed following first-line afatinib therapy. The resistance mechanisms in EGFR T790M-negative tumors can be broadly classified as bypass pathway activation, such as amplification of HER2 or MET, mutations of downstream signaling pathways such as PI3K and BRAF, small-cell or epithelial-mesenchymal transition histologic transformations, and unknown mechanisms. 98 As a result, patients that develop T790M-negative tumors have fewer specific therapeutic options. Currently, platinum-based doublet chemotherapy is recommended as second-line treatment in these patients. In the RESET study, patients with T790M-negative mutation were treated with second-line chemotherapy following first-line afatinib therapy. Median overall time on treatment and OS were 20.8 and 38.5 months, respectively, and 2- and 3-year survival rates were 75.9% and 55.3%, respectively. 97
EGFR TKIs have also been evaluated in the T790M-negative NSCLC setting. For example, the TREM study assessed the efficacy of osimertinib in patients with acquired resistance following first- or second-generation EGFR TKI, regardless of T790M status (N = 172; 52 with T790M-negative NSCLC). 99 While the efficacy of osimertinib was superior in patients with T790M-positive NSCLC, clinically significant activity was also observed in patients with T790M-negative NSCLC. After a median follow-up of 27 months, overall response rate (ORR) and disease control rate in patients with T790M- negative NSCLC were 28% and 64%, respectively, and median PFS and OS were 5.1 and 13.4 months, respectively. 99 Another real-world study from Japan reviewed medical records between 2012 and 2020 to compare the efficacy of first- or second-generation TKIs with chemotherapy as second-line therapy in patients with T790M-negative NSCLC (n = 39). 100 Median PFS and OS were 5.4 and 16.1 months in the chemotherapy group versus 3.4 and 12.8 months in the TKI group, respectively. 100 Similarly, in a study comparing the efficacy of anlotinib versus chemotherapy in Chinese patients with T790M-negative NSCLC (N = 20), median PFS was longer with chemotherapy compared with anlotinib (4.5 vs 3.0 months; P = 0.021). 101 Furthermore, the Afatinib plus Bevacizumab Combination study demonstrated the efficacy and safety of this combination therapy in patients with NSCLC with acquired resistance to EGFR TKIs, regardless of T790M status (N = 32, including 14 with T790M-positive and 18 with T790M-negative NSCLC). 102 ORR was 14.3% in patients with T790M-positive tumors compared with 22.2% in those with T790M-negative tumors. Median PFS was 6.3 and 7.1 months in patients with and without T790M-positive tumors, respectively. 102
The immunotherapy and chemotherapy combination also represents a potential therapeutic option for patients with T790M-negative NSCLC. In a subgroup of patients with NSCLC harboring EGFR mutations enrolled in the IMpower150 trial, median PFS was longer with atezolizumab plus bevacizumab plus carboplatin plus paclitaxel versus bevacizumab plus carboplatin plus paclitaxel (10.2 vs 6.9 months), including for those who had previously received TKI therapy (9.7 vs 6.1 months), 103 although T790M status was not available from the study. A Phase II study in Chinese patients (N = 40) with T790M-negative NSCLC enrolled between April 2018 and March 2019 showed promising efficacy of toripalimab plus platinum doublet therapy, with an ORR of 50% and median duration of response of 7.0 months. 104 Patients with programed death-ligand 1-positive tumor biopsy (60% vs 39%) or TP53 co-mutation (62% vs 14%) showed significantly better ORR; median PFS was 7.0 months whereas median OS was not reached at the data cutoff date (January 20, 2020). 104 A randomized Phase III trial is ongoing to further validate these findings (NCT03924050). 105 Similarly, two Phase III trials, CheckMate722 (nivolumab plus chemotherapy or nivolumab plus ipilimumab vs chemotherapy; NCT02864251) 106 and KEYNOTE-789 (pembrolizumab plus chemotherapy vs chemotherapy; NCT03515837), 107 and a Phase II trial, ILLUMINATE (durvalumab plus tremelimumab plus chemotherapy; NCT03994393) 108 are currently ongoing in patients with EGFR T790M-negative NSCLC.
Finally, several targeted therapies against specific resistance mechanisms are being investigated for patients with NSCLC harboring T790M-negative EGFR mutations. The combination therapy with selective MET inhibitors such as capmatinib, 109 tepotinib 110 and savolitinib, 111 and EGFR TKIs have shown promising antitumor activity in Phase I/II studies in patients with T790M-negative MET-driven resistance. In addition, an ongoing study is evaluating the efficacy of sapanisertib (a mTOR complex 1/2 inhibitor) in combination with osimertinib in patients with T790M-negative tumors (NCT02503722). 112
In summary and as illustrated in Figure 1, there are 2 major sequential treatment pathways for patients with EGFR mutation-positive NSCLC, depending on the type of EGFR TKI used in the frontline setting, and the acquired resistance mechanism associated with its failure. When afatinib or a first-generation EGFR TKI is used as frontline treatment, osimertinib becomes a subsequent option for patients who develop EGFR-dependent resistance mechanisms, including the T790M mutation (with the exception of certain acquired rare EGFR mutants such as G719X, S768I, L861Q and some compound mutations, or for rare cases acquiring Ex20Ins). For patients with EGFR-independent resistance mechanisms, combination treatment can be used for those with co-occurring genetic mutations, or chemotherapy for those with histologic transformations or unknown mechanisms. Conversely, osimertinib as first-line therapy can result in either clear resistance mechanisms (such as C797 S mutations in the EGFR or co-occurring genetic aberrations), or unknown mechanisms. Evidence from preclinical models and clinical sample studies suggests that patients may re-acquire sensitivity to first- or second-generation TKIs, albeit transiently, following disease progression on osimertinib, and that allelic conformation affects the response to subsequent TKI therapy.113 -116 Three possible scenarios have been described in the literature for patients with antecedent osimertinib treatment: (a) T790M loss + C797S mutation, where tumor cells re-acquire sensitivity to first- and second-generation EGFR TKIs; (b) T790M + C797S mutations in trans, where tumor cells become transiently sensitive to a combination of osimertinib and first-generation EGFR TKIs that target the alleles with T790M and C797S, respectively; and (c) T790M + C797S mutations in cis, where tumor cells are resistant to all three generations of EGFR TKIs, novel fourth-generation EGFR TKIs are needed.113 -116 Further research in clinical settings is required to explore the impact of allelic conformation on the response to subsequent EGFR TKIs in patients with antecedent osimertinib treatment. Currently, subsequent treatment options for patients following osimertinib involve combination therapy or chemotherapy, depending on whether they developed clear or unknown resistance mechanisms.

Different treatment strategies for patients with EGFR mutation-positive NSCLC after treatment with a first-line EGFR TKI inhibitor.
Factors Influencing the Selection of Frontline Therapy in Asian Patients With EGFR Mutation-Positive NSCLC
Predictors of acquired EGFR T790M in patients with NSCLC
Optimizing EGFR TKI sequencing strategies will require improved patient selection that incorporates clinical and molecular characteristics. In this regard, the T790M mutation status following first-line therapy is the most important factor driving the treatment sequence. Therefore, identification of patients who are likely to acquire T790M-positive mutation before commencing first-line therapy can inform decisions about appropriate first-line treatment. Currently, clinical evidence on the strong, independent predictors of T790M mutation is limited, which makes it difficult to identify patients who are likely to develop this mutation. In the multivariate analysis of molecular and clinical predictors, the presence of EGFR Ex19del mutations (vs Ex21 L858R mutations), younger age (< 65 years), the absence of metastases (brain or intrathoracic lymph nodes), and lower fluorodeoxyglucose (FDG) uptake on FDG-PET/CT imaging (indicative of lower metabolic rate of viable tumor cells) were independently associated with a higher probability of acquiring T790M mutation following treatment failure on first- or second-generation EGFR TKIs.117 -120 In addition, Chua et al conducted an in-depth analysis of genetic and transcriptome alterations shaping the EGFR TKI resistance trajectories. The study results showed that the presence of TP53 wild-type, aging mutational signatures, and the absence of whole-genome doubling were predictive for the emergence of T790M-positive resistance. 118 These molecular and clinical characteristics can help in the selection of patients who potentially can derive the maximum benefit from first-line afatinib followed by osimertinib treatment sequencing.
A T790M mutation is required for use of osimertinib in second line, which means that tumors showing the first signs of progression should be screened for mutations. Therefore, detection of T790M following progression on afatinib therapy must be optimized, where possible, using the most sensitive detection method(s) available.121 -123 While tissue biopsies allow histological analysis of the tumor and typically the most sensitive method of detection, they are often challenging to conduct in clinical practice due to factors such as tumor inaccessibility, requirement of invasive procedures, insufficient tissue availability, and tumor heterogeneity, all of which can result in missed mutations. In contrast, liquid biopsies are faster, easier to perform and a non-invasive alternative to tissue biopsies; however, they have low sensitivity and specificity, often resulting in false-negative results.121,123,124 A tissue re-biopsy is therefore recommended to confirm negative results from a liquid biopsy. 123 In addition, the guidelines recommend highly sensitive assays with a lower limit of detection of 5% mutant allele fraction for detecting the EGFR T790M mutation in post-treatment biopsies from patients who progress or relapse following initial response to EGFR TKIs. Sanger sequencing is not sufficiently sensitive to detect EGFR T790M mutations, so allele-specific PCR or NGS are recommended, the latter being the more common method.125,126
Other factors
While prolonging OS is the most important goal for patients with advanced NSCLC, the choice of the EGFR TKI should be based on certain drug-related factors, such as safety, tolerability, and efficacy against specific mutation types.
Tolerability is an important factor in treatment selection as it influences medication compliance and patient outcomes. Furthermore, the safety properties of EGFR TKIs differ, despite some similarities. The most common adverse events (AEs) with first- and second-generation EGFR TKIs include serious skin reactions, diarrhea, hepatotoxicity, and stomatitis; however, the incidence may vary across different agents. Most of the AEs can be managed by reducing the treatment dosage without affecting efficacy, which renders treatment plans more flexible. Third-generation EGFR TKIs bind irreversibly to mutant forms of EGFR and spare the wild-type; hence, AEs are relatively mild with these agents.
Even the 2 most common EGFR TKI-activating mutations, Ex19del and Ex21 L858R, have variable sensitivities to different EGFR TKIs. Patients harboring Ex21 L858R mutations have a shortened PFS with erlotinib compared with other regimens, and patients with uncommon mutations also have a shorter PFS with gefitinib than with other regimens. 127 Compared with first-generation EGFR TKIs, second-generation TKIs are broader inhibitory agents; afatinib, in particular, was effective against all EGFR mutations, including compound or common (Ex19del/Ex21 L858R) mutations and uncommon variants. 80
Future Perspectives
With the availability of various TKIs for EGFR in the frontline setting, it is critical that treatment strategies are developed to maximize treatment benefits. The clinical effectiveness and superiority of afatinib over first-generation TKIs in the first-line setting have been established by recent findings from real-world studies. Osimertinib has also shown superiority over first-generation TKIs and has been approved in the frontline setting; however, no prospective data are available comparing second- and third-generation EGFR TKIs, thus leaving uncertainty regarding the optimal treatment sequence. A better understanding of the impact of clonal evolution in response to different therapies may help to address this question. While the resistance mechanisms for second-generation TKIs are well defined, resistance to osimertinib is mediated by a diverse range of mechanisms and, currently, no targeted agents are available that specifically address these resistance mechanisms.
Consequently, a treatment sequencing strategy, where osimertinib is reserved for second-line use following afatinib treatment failure, would maximize the net survival benefit in patients who develop T790M-positive tumor. Data from post-progression analysis of the LUX-Lung trials and real-world studies support this treatment strategy, and have demonstrated long-term PFS and OS benefit with sequential afatinib and osimertinib treatment. Clinical characteristics such as EGFR Ex19del mutations, younger age (< 65 years), and the absence of metastases have been shown as strong independent predictors of T790M resistance following first-line EGFR TKI therapy, and thus can help patient selection in clinical practice.
However, this strategy would not be beneficial for patients who develop T790M-negative tumor, for whom treatment options are less well defined. As a standard of care in the second-line setting, platinum-based chemotherapy is recommended for patients with EGFR T790M-negative NSCLC. Early trials of immunotherapy plus chemotherapy have shown promising antitumor effects, but confirmatory Phase III trials have yet to be completed. Therapies targeted against underlying mechanisms of resistance are also being explored among patients with EGFR T790M-negative NSCLC.
To develop an appropriate sequential treatment approach that optimizes clinical benefit in patients with EGFR mutation-positive NSCLC, it is imperative that targetable mutations can be precisely detected, and the most suitable TKIs selected at each stage of sequential treatment. In addition, clinical decision-making should take into account the mechanisms and clinical factors that contribute to various mutations. Hence, further research into mechanisms of resistance to EGFR TKIs is needed to determine sequential therapy strategies.
Footnotes
Acknowledgements
Editorial support was provided by Syed Abdul Haseeb (MediTech Media Shanghai), and funded by Boehringer Ingelheim in accordance with the Good Publication Practices.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Zhejiang Province Medical and Health Science and Technology Project (2018KY048).
Declaration of Conflicting Interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RL and JZ have no conflict of interest to declare. XL is an employee of Boehringer Ingelheim.
Author Contributions
All authors contributed to the study conception, design, literature search, and analysis. In addition, all authors contributed to the preparation of the manuscript, provided critical feedback, and approved the final version of the manuscript.
Data Sharing Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Ethical Disclosure
No ethics approval was required for this review article as all data originated from previously published studies.