
Abstract
Background:
The aim of this study was to clarify the features and prognostic significance of isolated para-aortic lymphatic metastasis of endometrial cancer.
Methods:
A retrospective study of patients with stage IIIC endometrial cancer was performed based on the Surveillance, Epidemiology, and End Results (SEER) database. A total of 2767 patients were divided into three groups according to the lymphatic metastasis patterns: isolated pelvic lymphatic metastasis, isolated para-aortic lymphatic metastasis and dual lymphatic metastasis. The clinic-pathological characteristics and prognosis of patients were compared among the three groups.
Result:
The proportion of patients with isolated para-aortic lymphatic metastasis was 13.70%. Patients with isolated pelvic lymphatic metastasis or isolated para-aortic lymphatic metastasis shared similar histological characteristics, except that patients with isolated para-aortic lymphatic metastasis had a lower proportion of tumors over 5 cm in diameter than patients with isolated pelvic lymphatic metastasis (35.1% versus 45.7%, p = 0.001). Compared with patients with dual lymphatic metastasis, isolated para-aortic lymphatic metastasis was more common in patients with endometrioid tumors (78.6% versus 67.3%, p < 0.001), grade 1–2 cancers (53.3% versus 36.3%, p < 0.001) and negative peritoneal cytology (76.2% versus 61.1%, p < 0.001). Dual lymphatic metastasis was an independent predictive factor for the poor outcomes of patients at stage IIIC. However, in stage IIIC endometrioid tumors, patients with isolated pelvic lymphatic metastasis and those with isolated para-aortic lymphatic metastasis shared similar prognosis. Patients at stage IIIC with nonendometrioid tumors and patients at stage IV could not be further divided into subgroups according to lymphatic metastasis patterns in terms of prognosis.
Conclusion:
Endometrioid patients with isolated pelvic lymphatic metastasis and isolated para-aortic lymphatic metastasis share similar clinical pathological characteristics and prognoses.
Introduction
Endometrial cancer (EC) is the most common gynecological malignancy, with an increasing incidence in developed countries. 1 Patients with early stage cancer have good outcomes, with a 5-year survival rate of over 90%. Once lymphatic metastasis (LM) occurs, the prognosis is very poor. 2 According to the International Federation of Gynecology and Obstetrics (FIGO) 2009 staging system, the proportions of stage IIIC1 and IIIC2 tumors in patients with EC are 2.3% and 1.2%, respectively. The 5-year survival rates for patients with stage IIIC1 and IIIC2 tumors are 57.0% and 49.4%, respectively. 3 However, in the FIGO 2009 staging system, stage IIIC2 includes patients with para-aortic lymphatic metastasis (PALM) with or without pelvic lymphatic metastasis (PLM). Isolated PALM is not separated from either pelvic or para-aortic lymph node metastases. According to research from the Mayo Clinic, 67% of patients with lymphatic dissemination have PALM, and 16% of patients have isolated PALM. 4 Unfortunately, the characteristics of isolated PALM are still unclear. The aim of our study was to clarify the clinicopathological features and prognostic significance of isolated PALM compared with other lymphatic invasive patterns.
Materials and methods
With permission from the Surveillance, Epidemiology, and End Results (SEER) program of the United States National Cancer Institute, clinicopathological and survival information of women diagnosed with EC between 1 January 2010, and 31 December 31 2015, was collected. The SEER program includes 18 population-based cancer registries that collect cancer demographic, clinic, and outcome information on approximately 28% of the US population. Eligibility criteria included the following: (a) a primary diagnosis of EC with LM by surgical-pathological staging (including hysterectomy, pelvic lymphadenectomy and para-aortic lymphadenectomy) between 2010 and 2015; (b) a histological diagnosis of endometrioid adenocarcinoma, mucinous adenocarcinoma, serous adenocarcinoma, clear cell adenocarcinoma or Mullerian mixed tumor (MMT); and (c) all diagnoses were confirmed by positive histology. Patients with lymph node metastasis status unknown or survival time unknown were excluded.
A total of 2767 patients met the eligibility criteria. The recorded information included age at diagnosis, histology, grade, LM, cause of death and overall survival (in months). Age at diagnosis was classified into three groups: less than 50 years, 50–60 years, and over 60 years. Histologically, tumors were described as two types: endometrioid adenocarcinoma and others, including mucinous adenocarcinoma, serous adenocarcinoma, clear cell adenocarcinoma and MMT. Grade was recorded with a three-grade system: grade 1 (well differentiated), grade 2 (moderately differentiated) and grade 3 (poorly differentiated, undifferentiated or anaplastic). Peritoneal cytology was recorded with two categories: positive or negative. The pattern of LM was proposed and reported with a three-way system: isolated PLM, isolated PALM and dual LM (including both PLM and PALM). Furthermore, survival was calculated as the number of months from cancer diagnosis to death, and the cause of death was recorded for each patient.
Clinical and pathological characteristics were compared using Pearson’s Chi-square tests. A Cox regression model was used to analyze the independent risk factors for prognosis in patients diagnosed with stage IIIC tumors. Kaplan–Meier analysis was used to estimate the survival of patients with EC while stratifying by histology, and log-rank tests were used to evaluate differences in survival according to the pattern of LM. A p value less than 0.05 was considered statistically significant.
Results
The average numbers of pelvic lymph node and para-aortic lymph node removed were 14.58 and 7.08, respectively. The ratios of the three patterns of LM (isolated PLM, isolated PALM and dual metastases) were 40.73%, 13.70% and 45.57%, respectively. Therefore, 59.27% of patients with LM had PALM, and 23.11% of patients with PALM suffered from isolated PALM. Differences in the clinicopathological characteristics of patients with EC with lymphatic dissemination based on the three patterns of LM are listed in Table 1. The patterns of LM were not related to the age at diagnosis or depth of myometrial infiltration. Patients with isolated PLM or isolated PALM shared similar histological characteristics, including histological type, differentiation and peritoneal cytology. There was less isolated PALM in stage IV disease compared with patients with stage IIIC disease (3.4% versus 11.0% and 6.8%, p < 0.001 and p = 0.016). Patients with isolated PALM had a lower proportion of tumors over 5 cm in diameter than patients with isolated PLM (35.1% versus 45.7%, p = 0.001). Compared with patients with dual LM, isolated PALM was more common in patients with endometrioid tumors (78.6% versus 67.3%, p < 0.001), grade 1–2 cancers (53.3% versus 36.3%, p < 0.001) and negative peritoneal cytology (76.2% versus 61.1%, p < 0.001). A tumor size over 5 cm in diameter was more common in patients with dual LM compared with patients with isolated PALM (55.6% versus 35.1%, p < 0.001).
Comparison of clinicopathological features among three patterns of LM.

LM, lymphatic metastasis; MI, myometrial infiltration; PALM, para-aortic lymphatic metastasis; PLM, pelvic lymphatic metastasis; unk, unknown.
P1 value indicates the difference between patients with isolated PALM and those with dual LM; P2 value indicates the difference between patients with isolated PALM and those with isolated PLM.
Age at diagnosis over 60 years, grade 3 cancer, stage IV disease and positive peritoneal cytology were significantly associated with the poor prognosis of patients with EC. In the Cox regression models adjusted for the above factors (Table 2), dual LM remained an independent predictive factor for the poor outcomes of patients with lymphatic dissemination [hazard ratio (HR) = 1.625, 95% confidence interval (CI) 1.379–1.915, p < 0.001]. The prognosis of patients with isolated PALM and those with isolated PLM was similar (HR = 1.033, p = 0.811). In patients with endometrioid tumors, those with isolated PLM and those with isolated PALM shared a similar prognosis and showed better outcomes than those with dual lymphatic dissemination in stage IIIC disease [Figure 1(a)]. However, in stage IIIC disease with other tumors histologically and stage IV disease, there were no significant differences in the prognosis among patients with isolated PLM, isolated PALM or dual LM [Figure 1(b] and c).
Multivariate survival analysis in patients with endometrial cancer with LM.

CI, confidence interval; LM, lymphatic metastasis; PALM, para-aortic lymphatic metastasis; PLM, pelvic lymphatic metastasis.
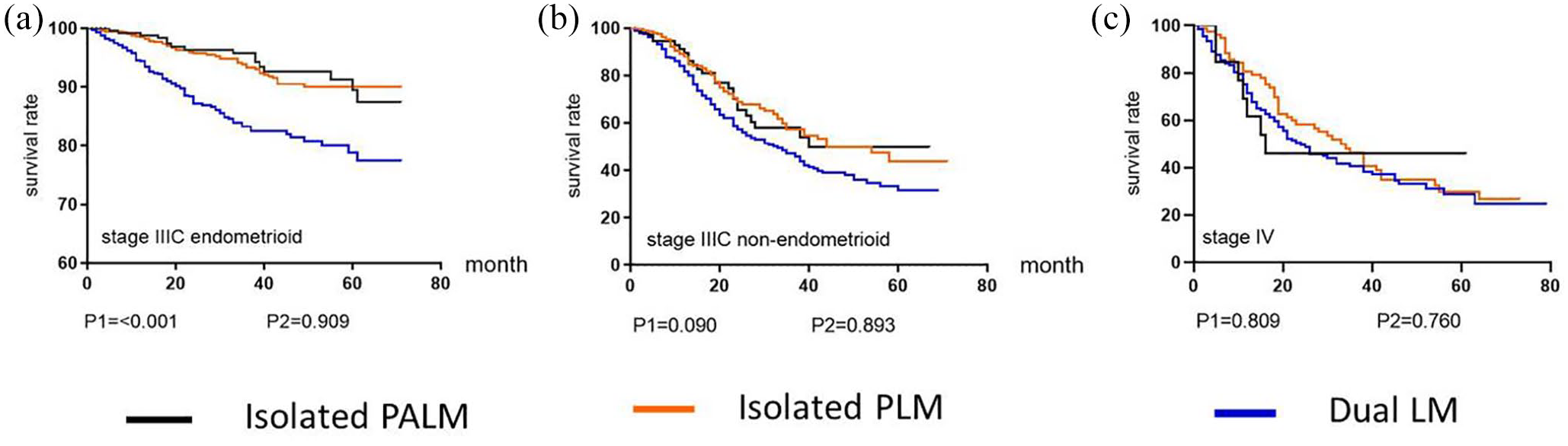
(a) Survival comparing among three patterns in endometrioid patients with stage IIIC disease. (b) Survival comparing among three patterns in nonendometrioid patients with stage IIIC disease. (c) Survival comparing among three patterns in patients with stage IV disease.
Discussion
It has been reported that stage IIIC2 tumors are associated with high all-cause and EC-specific mortality compared with stage IIIC1 tumors. 5 However, approximately 16% of patients with stage IIIC2 tumors have no pelvic lymphatic involvement. 4 There has been no study focusing on the prognostic significance of EC patients with isolated PALM. We compared stage IIIC1 and stage IIIC2 tumors with and without pelvic lymphatic dissemination, respectively. In our research, isolated PALM accounted for 13.70% of all tumors with lymphatic dissemination and 23.11% of all stage IIIC2 cancers. The incidence was variable in previous studies from 2% to 17%.4,6–11 Our results show that isolated PALM is similar to stage IIIC1 tumors in both clinical features and prognosis.
The exact mechanism of isolated metastasis is uncertain. Several possible reasons may explain the presence of this extraordinary metastasis pattern. First, pelvic low-volume metastases, including micrometastases (MMs, 0.2–2 mm) and isolated tumor cells (ITCs, <0.2 mm), are common in EC. In stage I–II EC with moderate risk factors, the detection rate of low-volume metastases is as high as 15%. 12 When only MMs or ITCs exists in pelvic lymph nodes, routine pathological examination is negative. In current, surgical-pathological staging and treatment strategy are based on routine pathology, the significance of ultrastaging for treatment and prognosis is still controversial. Second, direct spread to para-aortic lymph nodes via ovarian vessels is a possible route of lymphatic spread.13,14 Lymph nodes at the fundus of the uterus often return to para-aortic lymph nodes along the pelvic funnel ligament. 15 In theory, tumors in the fundus and corners of the uterus are more likely to migrate to higher levels through ovarian blood vessels, leading to isolated metastases. Third, aberrant and newly formed complicated lymphatic networks may result in more traffic branches connecting primary tumors to extrapelvic areas directly.16,17 Research from Chang indicated that lymphovascular space involvement is the only independent risk factor for isolated para-aortic lymphatic dissemination in patients with EC. 18
In our research, the factors associated with isolated PALM included endometrioid tumors, grade 1–2 tumors, negative peritoneal cytology and a tumor size less than 5 cm. Contrary to our traditional wisdom, these factors are low risk for EC and even para-aortic lymph node metastasis. Compared with patients with dual LM, endometrioid tumors and grade 1–2 tumors were more common in patients with isolated PALM, but there was no difference between patients with isolated PLM and those with isolated PALM. Although no sentinel lymph node mapping was performed, it is conjectural that both isolated PLM and isolated PALM are manifested as LM of the first site. There is no direct evidence that the isolated metastasis of cancer cells will further invade distant areas. One suggested possibility is that it is relatively difficult for endometrioid and well-differentiated tumors to metastasize further to other sites (through PLM or PALM) due to their low invasiveness. 19 Therefore, a special metastatic pattern, isolated PALM, guided by bypass or ovarian vessels, is highlighted in endometrioid and well-differentiated tumors compared with more invasive tumors. The positive rate of ascites cytology is significantly higher in dual LM compared with isolated PLM. Similarly to dual LM, malignant ascites is often caused by aggressive tumors. 20 Similar rates of positive peritoneal cytology of isolated PALM and isolated PLM support the conjecture that isolated PALM and isolated PLM are the first sites of LM. Isolated PALM is more common in patients with tumors smaller than 5 cm in diameter, which may be explained as follows. The proportion of tumors larger than 5 cm in diameter showed a gradient increase from isolated PALM to isolated PLM and then to dual LM. As mentioned above, isolated PALM is largely related to the vascular anatomy, such as an aberrant collateral reflux network and ovarian vessels. However, abnormal lymphatic reflux driven by a mechanical pressure gradient can be blocked by proximal lymphedema, which is more common in larger tumors. 21 On the other hand, cells of larger tumors are more invasive to metastasize to PALM through PLM. 22 Therefore, tumors larger than 5 cm in diameter are a risk factor for dual LM.
According to the FIGO 2009 staging system, patients with para-aortic lymphatic invasion with or without PLM were classified as stage IIIC2 with poor outcomes (relative to patients limited to PLM). 23 However, the analysis of the risk factors for isolated metastasis showed that isolated PALM was not associated with traditional high-risk factors for EC, such as the depth of muscle invasion and grade 3 tumors. In fact, patients with isolated PLM and isolated PALM share the same prognosis. Both isolated PALM and PLM are first-site metastases, which differ only in the location of metastasis mediated by anatomical factors. We speculate that LM at the first site does not affect the prognosis, regardless of whether the first-site metastasis is the pelvic lymph node or the para-aortic lymph node. In endometrioid cancer with stage IIIC disease, only when the second lymphatic station is invaded further can it be indicated that the tumor has a strong invasive ability and a poor prognosis. Therefore, the prognosis of patients with dual LM is worse than those with LM limited to the first site, including isolated PLM and isolated PALM. This phenomenon only exists in patients limited to lymphatic dissemination. Actually, based on our study, dual LM is related to more disseminated disease, which is different from isolated PALM. There is no difference among patients with three LM patterns in survival when the tumor breaks through the first site of metastasis and distant metastasis occurs, just as in stage IV, the type of lymphatic metastasis has no effect on prognosis. However, an analysis of 722 nonendometrioid patients with LM showed that stage IIIC tumors could not be further divided into subgroups according to the site of lymphatic dissemination. Patients with metastases to pelvic and/or para-aortic lymph nodes share the same outcomes, which is similar to staging of uterine sarcomas. 24
We believe that resection of solid tumors is necessary for patients with EC, and the same is true for those with isolated metastatic para-aortic lymph nodes. Many experts have recommended aortic node dissection based on frozen sections of the primary tumor, assessing for high-risk factors (depth of invasion/lymphovascular space involvement/grade/histology) and positive pelvic nodes (selective frozen section of enlarged or suspicious lymph nodes).25,26 However, as confirmed above, isolated PALM was not associated with traditional high-risk factors for endometrioid cancer. A sentinel lymph node biopsy is recommended for lymph node assessment, especially in patients with low-risk EC. 27 Sentinel node mapping is performed by the injection of indocyanine green into the cervical stroma in the clinic, and the range of assessment includes mainly the pelvic lymphatic reflux area. 28 Patients with isolated PALM are probably neglected because of negative sentinel lymph nodes or absence of high-risk factors. Considering that isolated PALM is not relatively uncommon, imaging techniques used for para-aortic lymph nodes as sentinel lymph nodes should be emphasized, such as injection at the bottom of the uterus and deep cervical injection. 29
There are two main shortcomings to our study. The use of retrospective design from a large national database could not control for the range and quality of the lymphadenectomies and adjuvant therapies. First, information about adjuvant treatment as a protective factor is not available on an individual level. However, according to the guidelines, radiotherapy and/or chemotherapy are recommended for patients with advanced EC. Due to the maturity of adjuvant therapy for EC, individual differences in large databased research will not cause errors in results theoretically. Second, there is lack of quality control for lymphadenectomy. Although the average number of pelvic lymph nodes removed in our study is basically consistent with the current routine operation mode, there must be insufficient lymphadenectomy in some cases due to the wide resources and large number of patients retrospectively. If there were a large number of cases with insufficient pelvic lymphadenectomy or missed diagnosis of metastatic pelvic lymph nodes in this study, it would directly lead to the increase of the rate of isolated PALM. Therefore, it can be speculated that the prognosis of these patients with isolated PALM will be similar to that of cases with dual LM in clinical. However, our results show that the prognosis of patients with isolated PALM is significantly better than that of patients with dual LM. From another point of view, the incidence of isolated PALM in our study is 13.7%, which is roughly equivalent to the result reported from Mayo Clinic, and it can indirectly reflect that the quality and quantity of lymphadenectomy and the quality of pathological examination in this study are reliable. Our results are sufficient to show that there is an objective subgroup with isolated PALM in patients with EC, and it should reflect the nature of the disease. However, the significance of the isolated PALM for survival still needs higher quality clinical data to verify, in order to provide enough support for the revision of clinical assessment and treatment.
In conclusion, isolated PALM and isolated PLM share similar clinical pathological characteristics and prognoses, and the outcomes of patients with endometrioid cancer with isolated PALM are superior to those with dual LM in patients with stage IIIC2 disease. The significance of the existence in patients with EC with isolated PALM needs further study.
Footnotes
Acknowledgements
We acknowledge the fund support provided by Beijing High-level Health Personnel Training Program (2015-3-090).
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Beijing High-level Health Personnel Training Program (2015-3-090).