
Abstract
Here, we reported the rare case of primary pleural squamous cell carcinoma (PPSCC) in a 71-year-old male patient. After chemo and targeted therapies, the patient showed continuous tumor progression and clinical deterioration. Fortunately, the patient had a high expression level of PD-L1 (80%) in the tumor tissues. Ultimately, the patient survived for additional 6 months with camrelizumab treatment. In summary, camrelizumab may be a good candidate for the treatment of PPSCC, especially in tumors with high PD-L1 expression.
Introduction
Primary pleural tumors are rare tumors and classified as mesothelial, lymphoproliferative, and mesenchymal neoplasms by the World Health Organization classification. 1 Primary pleural squamous cell carcinoma (PPSCC) is extremely rare and has been described in only few case reports. Due to its rarity, the diagnosis and treatment of PPSCC is a serious challenge to clinicians. 2
Based on previous case reports, PPSCC responds poorly to drug treatment. A PPSCC case misdiagnosed as localized mesothelioma exhibited a good response to operation and local radiotherapy. 3 However, a PPSCC case diagnosed by thoracic fine-needle aspiration, cytology progressed after four cycles of gemcitabine mono-chemotherapy. 4 In another case report, the death of a SMARCB1(INI1)-defective PPSCC case was reported as a result of the disease progression even after receiving six cycles of cisplatin plus gemcitabine and tegafur alone. 5 Current therapy recommends that early detection, diagnosis, and surgery are essential for the management of PPSCC. Targeted therapy, chemotherapy, and radiotherapy could largely be utilized as the final therapeutic option when patients cannot receive surgery due to tumor recurrence or distant metastasis. 3 Immune checkpoint inhibitors (ICIs) provided a new hope when tumor progresses after radiotherapy, chemotherapy, and targeted therapy. Camrelizumab (AiRuiKa™), a programmed cell death protein 1 (PD-1) inhibitor being developed by Jiangsu Hengrui Medicine Co. Ltd., Jiangsu, China, recently received conditional approval in China for treatment of relapsed or refractory classical Hodgkin lymphoma and was also expanding the therapeutic repertoire for other malignant tumors. 6 Here, we reported the case of PPSCC managed with chemoradiotherapy, targeted therapy, and ICIs. Our case report may contribute to a further understanding of the beneficial effects of camrelizumab, thereby suggesting it as an effective drug for PPSCC and thus providing new insights into the treatment of PPSCC.
Case Presentation
A 65-year-old man was referred to the department of oncology with complaints of right chest and back pain, cough, expectoration, and dyspnea for more than 9 months and had been diagnosed with PPSCC by another hospital. He was also diagnosed with type 2 diabetes for 7 years, with a past history of varicose veins in both lower extremities. No other family history of cancer was reported.
A review of the patient’s medical history showed that the initial symptoms of the patient were pain in the right chest and back, with cough and expectoration; however, subsequently, the patient was inadvertently found to have multiple lymph nodes of different sizes in the left neck, which was neglected by the patient. With progressive enlargement of the lymph nodes and aggravation of the cough, sputum, and chest pain, he visited a local hospital. After paracentesis of the pleura, immunohistochemistry revealed that the tumor tissue (TT) was a poorly differentiated squamous cell carcinoma, and the final pathological diagnosis was PPSCC. No abnormality was found in head magnetic resonance imaging and bone scan. Computed tomography (CT) scan showed extensive inhomogeneous thickening of the right and interlobar pleuras that invade the right pericardial invasion with mediastinal lymph nodes surrounding the superior vena cava. Therefore, he received radiotherapy for mediastinum as well as chemotherapy. The treatment of cisplatin plus paclitaxel systemic chemotherapy was terminated after two cycles of the chemotherapy, since the patient could not tolerate severe gastrointestinal distress. L858R mutation in epidermal growth factor receptor (EGFR) exon 21 and EML4-anaplastic lymphoma kinase (ALK) fusion gene mutation was found in genetic testing. Due to economic reasons, the patient first chose gefitinib instead of the ALK inhibitor. Tumor progression was observed after the patient received gefitinib as the targeted therapy for 4 months. However, both lung and liver metastasis were detected by CT scan. During the treatment, the patient’s dyspnea was not alleviated, and the general condition of the patient was exacerbated with a weight loss of 10 kg within 6 months.
Subsequently, the patient was transferred to our hospital for further treatment. On examination, vital signs of the patient were within normal limits at the time of admission. Following physical examination of the patient, multiple enlarged lymph nodes were found (approximately 4 cm) in the left neck with partial fusion, hard texture, irregular shape, smooth surface, poor mobility, but no tenderness. The patient had obvious dyspnea, cough, expectoration, and laboratory tests (Table 1) (Figure 2) showed platelet aggregation, hypoproteinemia, and abnormal coagulation function. The CT scan showed (Figure 1) bilateral pleural thickening with bilateral pleural effusion, which were consistent with pleural malignant tumor. The family members of the patient showed a strong willingness for active treatment. We decided to detect the expression of PD-L1 by needle biopsy again. However, after evaluation by an anesthesiologist, various factors, such as severe pulmonary infection and pleural effusion with dyspnea precluded transthoracic fine needle biopsy, were considered. Moreover, the patient was accompanied by coagulation dysfunction and platelet aggregation. It was considered that the risk of malignant thrombosis in perioperative period was extremely high, and the pulmonary function was poor, which could be life threatening. Therefore, only the left cervical lymph node biopsy was performed. The immunohistochemical results supported the neuroendocrine function of squamous cell carcinoma (Figure 3): Ki67 (+, 70%), CD56 (−), Syn (++), P40 (+++), P63 (++), CD20 (−), Vim (−), EMA (++), TTF1 (++), NaspinA (−), CD99 (−), and PD-L1 (+, 80%). After retesting the hematological samples, no mutations were observed in the EGFR and ALK genes of the patient. Hence, targeted therapy was not selected. Fortunately, the tumor had a high expression of PD-L1; thus, we decided to administer camrelizumab according to the recommended intravenous dose of 200 mg (once every 3 weeks) for a total of six times from October 20, 2019 to February 11, 2020 (Figure 4).
Patient abnormal laboratory values on admission.


Comparison of chest CT scans before and after treatment, bilateral pleural and interlobar pleural thickening with pleural effusion (arrow).

Changes in serum tumor markers (CYFRA 21-1 reference: 0–3.3 ng/ml; NSE reference: 0–16.3 ng/ml; CA125 reference: 0–35 U/ml; CEA reference: 0–5.2 ng/ml; CA724 reference: 0–6.9 U/ml; Ferritin reference: 24–336 ng/ml).

Histopathological examination results of cervical lymph nodes. (a, b) Hematoxylin and eosin-stained shows squamous cell carcinoma with neuroendocrine function. (c, d) Tumor cells staining positive for p40. (c) 200×, (d) 400×, (e) Tumor cells staining positive for p63.
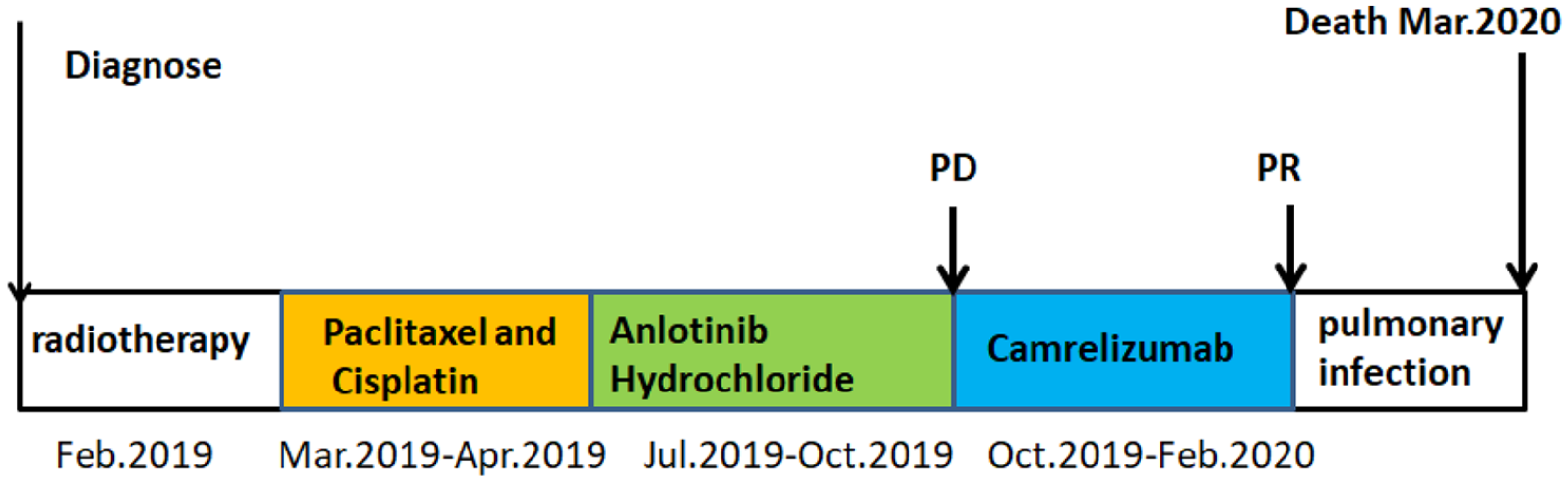
Treatment timeline of the patient.
After the first administration of camrelizumab, the symptoms of dyspnea were significantly relieved, which boosted our confidence in continuing the treatment. Re-examination of CT after the fifth treatment showed that the pleural effusion, pleural nodules, pulmonary lesions, and lymph nodes were smaller than before. The patient developed cough, expectoration, and dyspnea 1 month after the end of the treatment. However, the novel coronavirus (COVID-19) outbreak delayed the patient’s access to treatment. The patient had massive pericardial effusion. Laboratory tests on the last admission showed that the infection was serious and that cardiac function deteriorated. We observed that a number of elevated cytokines revealed that the patient’s immune system was destroyed due to ICIs (Table 2). Eventually, the patient died as result of respiratory and circulatory failure.
The patient has severe infection with deterioration of cardiac function.

Discussion
The coexistence of EGFR and ALK-EML4 gene mutations in cancer patients
The EGFR mutation and ALK rearrangement, as the two most important driving genes of non-small cell lung cancer (NSCLC), are considered as independent molecular events and are mutually exclusive in most cases. 7 The coexistence of EGFR and ALK-EML4 gene mutations remains as a rare event in patients with NSCLC. The gene testing report of this patient showed the coexistence of EGFR and ALK-EML4 gene mutations. In previous reports, the EGFR mutation and ALK rearrangement were linked to lung adenocarcinoma in nonsmoking or light-smoking individuals. EGFR mutations occur mainly in adenocarcinomas, females, nonsmokers, and Asian patients, whereas for the ALK rearrangement, the racial and gender differences were not significantly different, but patients with the ALK rearrangement were observed to be younger with more mucous pathological types. 8 This patient had a 40-year history of smoking, and the pathological diagnosis did not support adenocarcinoma. Therefore, the gene detection results of the patient posed challenges to the diagnosis. However, it should be noted that the patient’s two hematological samples for the genetic test were completely different. The patient’s genetic test sample came from the patient’s plasma and circulating tumor DNA (ctDNA), instead of the TT. Some researchers speculated that due to the small number of biopsy specimens, the heterogeneity and sampling deviation in the tumor may lead to the real existence of TT negative/ctDNA positive EGFR mutation status. 9 Therefore, the possibility of false positive cannot be totally ruled out. The diagnosis and pathological results of PPSCC are still the gold standard for diagnosis. The pleural biopsy of this patient showed that it was a poorly differentiated squamous cell carcinoma and immunohistochemical biopsy of cervical lymph nodes of the patient’s metastatic lesions was the same. The nuclear staining of P63 and P40 antibodies was strongly positive and diffusely positive in squamous cell carcinoma, which confirmed the diagnosis of PPSCC. Differential diagnosis with pleural mesothelioma was made in this case. The patient has no history of exposure to asbestos. Hence, the differential diagnosis may be readily made because of pathognomonic diagnostic markers. The immunohistochemical markers reflected in the IMIG and WHO guidelines for tumors of mesothelial origin were calretinin, CK5/6, WT1, D2-40, and mesothelin. Epithelial markers include claudin 4, CEA, MOC31, TAG-72, Ber-EP4, and MUC4.1,10,11 The CT examination of the patient found no tumor in the mediastinum and other organs, which further supported the diagnosis of a primary pleural tumor. This case illustrated the clinical complexity, which may be due to the inconsistency of EGFR mutation status between TT samples and ctDNA due to intratumoral heterogeneity and relatively low sensitivity of amplification refractory mutation system. The ctDNA/TT model may be a reasonable clinical procedure for determining the EGFR mutation. 12 However, it is undeniable that the gene test results also provide another attempt for the treatment of this patient.
Consideration on the treatment of primary pleural tumor
Pleural squamous cell carcinoma is characterized by malignant tumor growth, invasion of surrounding tissues or organs, and metastasis. Therefore, delay of diagnosis and proper treatment will culminate in serious clinical consequences and lead to poor prognosis. At present, early detection and resection of PPSCC is recommended. Guanbao 13 believed that total surgical resection was one of the best treatments for PPSCC. If the tumor invades the lung, partial lobectomy may be required; however, if the tumor is malignant and diffuse, pleural lobectomy can be considered. Some scholars suggest that early PPSCC can also be resected by video-assisted thoracoscopic surgery (VATS). If VATS cannot guarantee a clear resection margin, thoracotomy is recommended. For pleural nodules with unclear boundaries and suspected malignant pleural nodules, intraoperative freezing examination should be used to determine whether extended resection should be performed to reduce the risk of recurrence and improve the prognosis. Radiotherapy and chemotherapy can be considered for patients with multi-course recurrence who cannot be completely resected; however, the specific scheme of radiotherapy and chemotherapy needs to be explored. This patient was not diagnosed and treated in time at the early stage and was referred to the department of oncology of our hospital for treatment more than 9 months after the onset of the disease, which delayed the best time for treatment. The patient had multiple metastases all over his body, and the patient’s nutritional status was poor, having missed the best time for surgery and radiotherapy, and the tumor was still progressing after chemotherapy and targeted therapy, which made the treatment difficult. Fortunately, the patient showed a high expression of PD-L1 by immunohistochemistry, and finally we decided to administer immune checkpoint blocking therapy. At present, the main bottleneck of immune checkpoint blocking therapy is its low response rate in most cancers. More and more studies have shown that high expression of PD-L1 may be one of the important factors affecting the efficacy of anti-PD-1/PD-L1 therapy. 14 The expression of PD-L1 in this patient was as high as 80%, and the treatment was effective after using camrelizumab for six cycles. It was proven that the response rate of PD-1 monoclonal antibody is related to the high expression of PD-1 ligand in tumor cells. In summary, it was shown that ICIs are good choice for treatment, especially in tumors with high expression of PD-L1.
The patient’s lungs had been infected throughout, observed due to the elevated inflammation markers, such as C-reactive protein, various interleukins, procalcitonin, white blood cells, and neutrophils. We first considered the exacerbation of the patient’s lung infection and upgraded the antibiotic to meropenem. Although the inflammatory index of the patient decreased, symptoms such as dyspnea were still aggravated. Therefore, we considered the immune-related adverse events (irAEs); however, the symptoms did not alleviate after treatment with methylprednisolone. During the treatment, CT scan showed only pulmonary infection with no sign of interstitial pneumonia caused by camrelizumab (Figure 5). Hence, using viral nucleic acid testing and chest CT, it was reported that the patient was not infected with COVID-19 pneumonia. In conclusion, the patient’s condition became complicated at the end stage of the disease. Hence, we believe that the patient might have died due to systemic inflammatory response syndrome and respiratory with circulatory failure caused by ICIs.

Pulmonary infection changes in the patient.
Conclusions
We describe an interesting case with multidisciplinary therapy, including camrelizumab, to manage PPSCC. Due to the rarity of PPSCC and the short observation time of all previously reported cases, the treatment plan and curative effect need to be further investigated. Camrelizumab has shown a beneficial effect and the indications for this drug should be extensively explored in the future.
Footnotes
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Provincial Developmental Fund of Traditional Chinese Medicine—Key Discipline of TCM (Oncology of TCM); Project Number: 2100601.
Author Contributions
YW and YG contributed equally, conceived the idea, conceptualized the study, and drafted the manuscript. HC collected the data. HL analyzed the data. XF and RY reviewed the manuscript. All authors read and approved the final draft.
Informed Consent
The patient’s legal representative provided consent for publication of the patient information and images included in this manuscript.