
Abstract
Adrenocortical carcinoma (ACC) is a rare malignancy with a poor prognosis. Treatment options for ACC are limited, with resection the main intervention. Most cases present in late metastatic cases, and data regarding effective therapies is limited. We report a case of ACC in a 40-year-old woman with history of ACC postadrenalectomy, who presented with recurrent metastatic ACC in the left perinephric space. She was started on pembrolizumab which was added to her mitotane maintenance therapy. Complete radiological response was achieved after 4 cycles of pembrolizumab. As far as we know, this is the first case to achieve complete radiological response with mitotane and pembrolizumab in recurrent metastatic ACC, with negative prognostic markers and no prior radiotherapy. As our findings are in the setting of one clinical case, we suggest the need to perform a trial to assess the benefit of combining mitotane and pembrolizumab in treating metastatic ACC.
Keywords
Introduction
Adrenocortical carcinoma (ACC) is a rare tumor with an incidence rate of 1.26 per million person-years. 1 While the prognosis of ACC is good in early stages, it progressively worsens at later presentations.2,3 In effect, 5-year stage-dependent survival is 66% to 82% for stage I, 58% to 64% for stage II, 24% to 50% for stage III, and 0% to 17% for stage IV. 4
Nonmetastatic ACC is usually treated with surgical resection. 5 Mitotane is the only drug approved for treatment of ACC by the US Federal Drug Administration (FDA). 6 Unfortunately, it has low efficacy, a narrow therapeutic index, and can thus cause serious side effects. 7
We report a case of a 40-year-old patient with left ACC status postadrenalectomy, with recurrence several years later and invasion of the left quadratus lumborum and oblique muscles. Complete radiological response was attained after 4 cycles of pembrolizumab, in combination with mitotane. To date, we do not know of any other case of recurrent metastatic ACC that had complete radiological response to a combination therapy of mitotane and pembrolizumab.
Case Description
We present a case of a 40-year-old woman who was initially diagnosed with ACC in 2012 following left adrenalectomy that revealed a 7 × 6 × 3.5 cm soft tissue mass weighing 91 g. The presence of pleomorphism, <25% clear cells, diffuse pattern of growth, high mitotic index, hemorrhage and necrosis, large tumor weight (91 g), and foci of lymphovascular invasion was consistent with stage-II ACC. The patient had recurrent nodules in the left subdiaphragmatic space in 2016 (progression to stage IV) that were followed and increased in 2018 prompting re-exploration. Medial and lateral retroperitoneal tumors were excised, and both positive were for ACC.
Since the initial diagnosis, the patient had been maintained on mitotane with therapeutic levels achieved at a dose of 2 g (Table 1). However, as our institution lacks the capacity to determine mitotane level, the patient opted to visit an independent laboratory for testing up until 7 years since initial diagnosis. To note, her daily dose of mitotane since the start of treatment never exceeded 2 g as she was unable to tolerate higher doses. One year after re-exploration surgery, patient started complaining of left upper quadrant abdominal pain prompting repetition of magnetic resonance imaging (MRI) abdomen w/ gadolinium which showed multiple left perinephric peripherally enhancing soft tissue nodules, the largest seen along the inferior pole of the left kidney measuring 2 × 2.5 cm with probable invasion of the left quadratus lumborum and oblique muscles, highly suspicious for metastatic lesions. Follow-up with positron emission tomography computed tomography (PET CT) showed multiple fluorodeoxyglucose (FDG)-avid soft tissue nodules in the left perinephric space, consistent with local recurrence, and new FDG-avid left retrocrural soft tissue nodule likely metastatic adenopathy. Computed tomography abdomen and pelvis done 2 months after onset of symptoms showed soft tissue lesions in the left posterior pararenal/perinephric space (Figure 1). Programmed death-ligand 1 (PD-L1) testing done on the metastatic lesion showed the patient’s tumor to be negative for PD-L1. FoundationOne CDx next-generation sequencing (NGS) was subsequently done on the metastatic lesion. Next-generation sequencing allows for large-scale DNA sequencing in a parallel fashion providing full coverage of the entire genome, enabling efficient and accurate detection of novel and rare somatic mutations, and therefore, detecting potential therapeutic targets. 8 Next-generation sequencing showed the tumor to be microsatellite stable (MSS), and the tumor mutational burden to be 6 Muts/Mb (<10 Muts/Mb is considered low). Next-generation sequencing genomic findings showed CCND2 amplification, ATRX splice site 5698-2A > C, FANCC inversion exons 10-11, FGF23 amplification, FGF6 amplification, KDM5A amplification, AND TP53 Q52* alteration.
Mitotane levels taken at different intervals of time with corresponding mitotane dose.

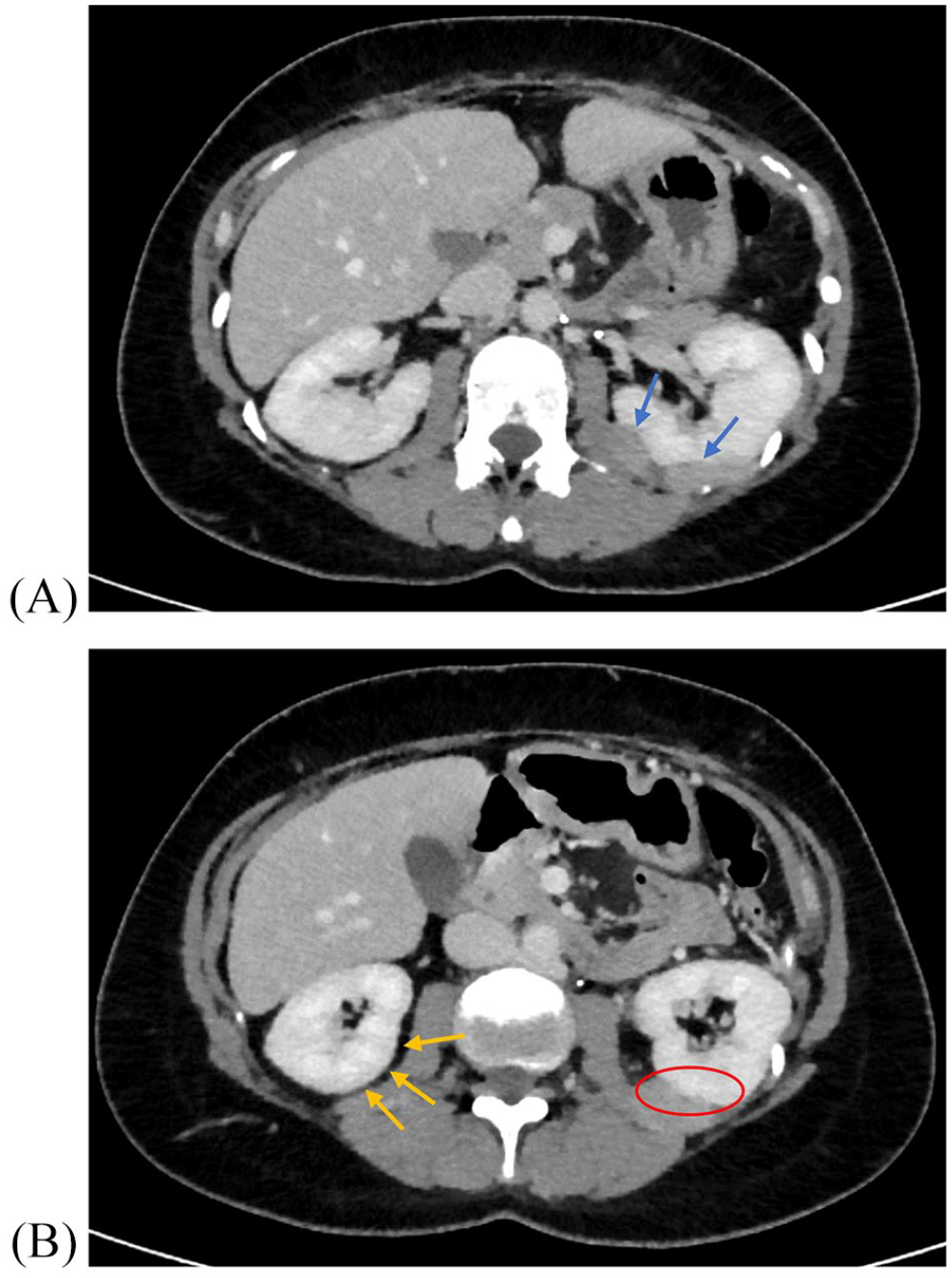
CT abdomen and pelvis showing (A) soft tissue lesions in the left posterior pararenal/perinephric space (lobulated like structures, blue arrows) (B) obstruction of fat visualization by the lesions around the left kidney as compared to the right kidney (red circle). Yellow arrows show the black space representing fat around the right kidney.
After discussion with family about a new study published by Raj et al 9 in JCO 2019 where pembrolizumab was used in ACC, it was agreed upon to start pembrolizumab while continuing mitotane and re-evaluating patient after completion of 4 cycles of pembrolizumab. Despite progression on mitotane, the drug was continued after the addition of pembrolizumab. This decision was made based on a study by Head et al that suggested a possible synergistic effect between mitotane and pembrolizumab in patients who failed mitotane monotherapy. The combination therapy was effective in both microsatellite instability-high and MSS adrenocortical tumors. 10 The tumor was not hormonally active neither at presentation nor at recurrence. Computed tomography abdomen done after 2 cycles of pembrolizumab showed marked decrease in size and number of left perinephric soft tissue masses and the decision was made to continue pembrolizumab. After 4 cycles of pembrolizumab, imaging done showed complete resolution of metastatic perinephric soft tissue (Figure 2).

CT abdomen and pelvis showing (A) complete resolution of nodular soft tissue thickening in the left posterior pararenal/perinephric space and disappearance of the lesions seen in the previous image with better visualization of the left kidney (orange arrows) and (B) better visualization of the fat surrounding the left kidney along with better overall visualization of the kidney (yellow circle).
We obtained additional markers in an attempt to find an association between a prognostic marker and the patient’s complete radiological response. Immunoscore done was found to be in the low category (38th percentile) when compared to data obtained from colorectal cancer patients, as no other data points are available in the literature. Immunoscore was performed on the retroperitoneal lesions. Paraffin sections of the tumor and invasive margin were processed by immunohistochemistry, and the densities of CD3+ and cytotoxic CD8+ T-cells in the tumor and in the invasive margin were quantified per mm2. The densities were converted into percentiles based on previously collected data from colorectal cancer patients at our institution. An immunoscore for each patient was derived from the mean of 4 density percentiles. 11 Tumor-associated macrophages (TAMs) were found to be in high density at 200/mm2 and 400/mm2 at the intratumoral site and the interface, respectively. We were only able to use CD68 in immunostaining, as CD163 was unavailable. Using CD3, CD8, and CD25 immunostains, we were able to stain for regulatory T-cells, which were found to represent only 5% of total lymphocytes (<10/mm2) (Figure 3).

Regulatory T-cells detected within the adrenocortical tumor using CD3, CD4, and CD25 immunostains at 60× (area within the circle, one of the cells pinpointed with the arrow). Tregs are CD3+, CD4+, CD25+, and FoxP3+ T-cells. Tregs were found to constitute less than 5% of the white blood cells within the tumor, favoring a good prognosis.
Discussion
Several trials focused on the use of immunotherapy but have failed to provide alternative treatments to ACC.12-15 Interestingly, the drug pembrolizumab, a programmed cell death protein 1 (PD-1) inhibitor, showed promising results with clinically significant antitumor activity, and a manageable safety profile.9,10 Two phase-II trials investigated the use of pembrolizumab in patients with metastatic ACC. Microsatellite instability, PD-L1 expression, and germline mismatch repair (MMR) alteration were also studied.9,16 The findings of these 3 studies are summarized in the tables below (Tables 2 and 3). A retrospective study done by the oncology team at the University of Colorado looked at 6 patients who received both mitotane and pembrolizumab for treatment of their ACC. 10 Two patients had a partial response and 4 had stable disease (8-19 months) with 2 of them progressing and one discontinuing pembrolizumab due to side effects. All 6 patients lived for at least 16 months after adding pembrolizumab to mitotane. 10
Baseline patient and disease characteristics of ACC patients in 2 phase-II trials.
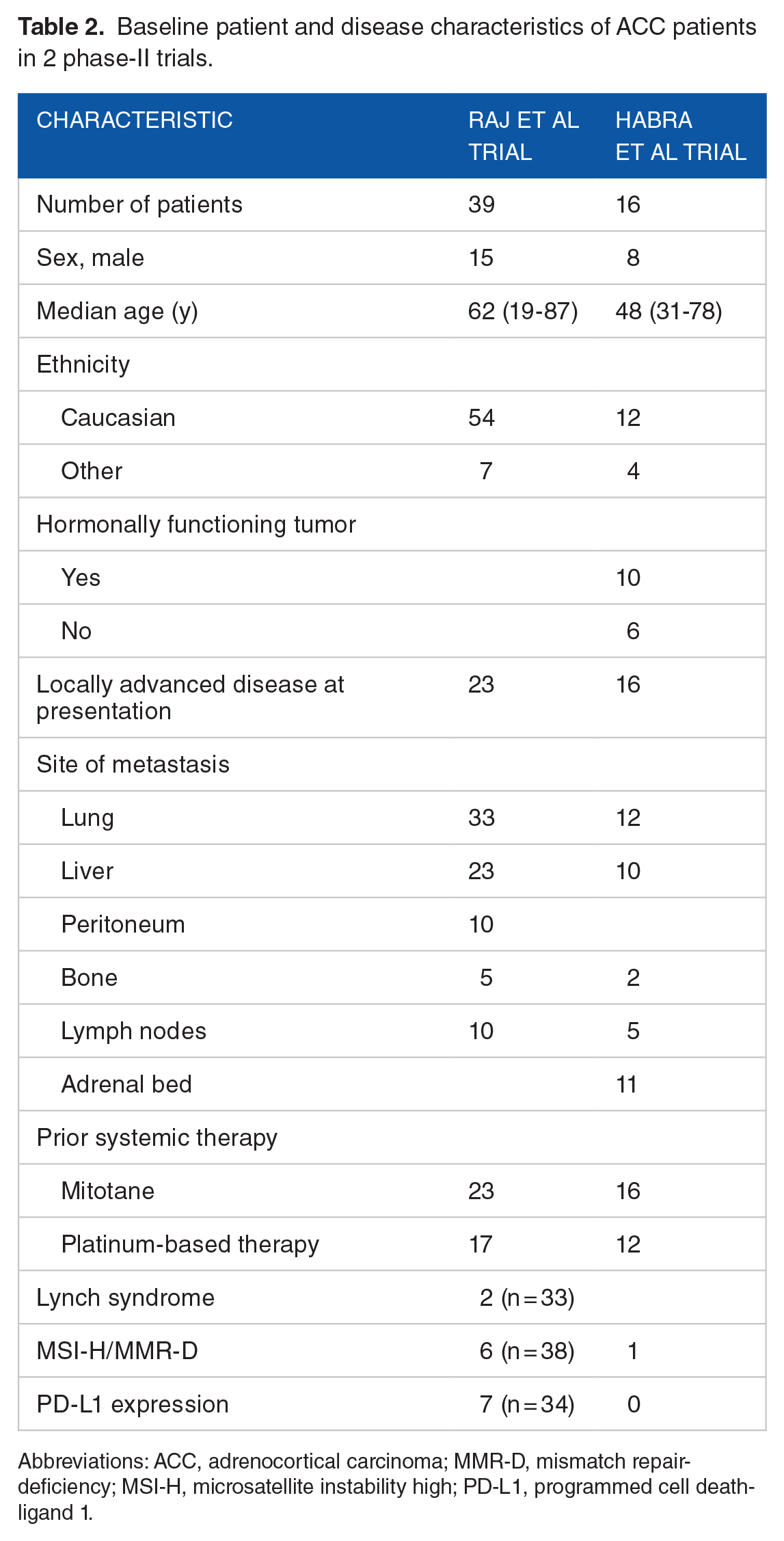
Abbreviations: ACC, adrenocortical carcinoma; MMR-D, mismatch repair-deficiency; MSI-H, microsatellite instability high; PD-L1, programmed cell death-ligand 1.
Objective response of ACC patients according to RECIST v1.1 criteria in 2 phase-II trials.

Abbreviation: ACC, adrenocortical carcinoma.
Due to the rarity of ACC, data on the effectiveness of immunotherapy in this disease has been scarce. While pembrolizumab has been gaining traction as a therapeutic option in the treatment of ACC, its use has yielded partial response in best case scenarios. 9 However, there is one case of a 40-year-old woman with ACC metastatic to the liver and lungs, with MSH2 and high tumor burden, that showed complete radiological response to exclusive therapy with pembrolizumab, after 5 cycles and was discontinued due to adverse events. To note, unlike our patient, she had favorable prognostic factors and received prior radiotherapy which could have led to abscopal effect. 17 She had 3 procedures of radiofrequency ablation, and a stereotactic body radiation therapy (SBRT) of a lung lesion before starting pembrolizumab. Evidence also suggests that a combination of radiotherapy and immune checkpoint inhibitors may boost the abscopal effect and promote greater antitumor responses. 18 To date, our patient is the only known case with negative prognostic markers (MSI-S, low tumor burden, negative PD-L1 expression) who responded to combination mitotane and pembrolizumab, with no prior radiotherapy sessions.
In addition, of the genomic findings obtained from NGS, CCND2 amplification has been linked to ACC, and has been reported in 1% to 7% of ACC in data sets.19,20 TP53 mutations have been reported in 20% to 33% of ACCs118-122, and both mutations and aberrant expression have been associated with poor outcomes and decreased disease-free survival.21-23
The negative prognostic markers combined with the unexpected complete radiological response led us to explore novel markers such as TAMs, regulatory T-cells, and the immunoscore to better predict response to therapy in future patients.
Tumor-associated macrophages are the most abundant immune cells within tumor microenvironment and have been associated with worse prognosis in many types of cancer. 24 In our patient, a high density of TAMs was found in both intratumoral site and at the interface. Nevertheless, controversy still exists over the use of TAMs as prognostic markers and further studies are needed. Regulatory T-cells (Tregs, CD3+, CD4+, CD25+, and FoxP3+) maintain tolerance to self-antigens and modulate the induction of effector T-cells. However, they hinder antitumor immunity which contributes to tumor progression in many cancers.25,26 A connection between a high number of regulatory T-cells and a worse prognosis has been described in several tumor types. 27 Less than 5% (10/mm2) of cells were regulatory T-cells in our case, which favors a good prognosis. However, limited data exists on regulatory T-cells as prognostic markers in ACC. The immunoscore, a novel prognostic marker, has been found to strongly predict overall survival in patients with cancer. 28 Immunoscore reflected time to recurrence, disease-free survival, and overall survival. A high score was associated with a lower risk of recurrence, whereas a high score was associated with a high risk of recurrence. 11 In our patient, a low score was found (38th percentile) corresponding to a high risk of recurrence. However, immunoscore data from colorectal cancer was used to calculate our score, due it being the only available data. 29 Therefore, we need to obtain more data on immunoscore in ACC, as our result might need to be interpreted differently in the setting of ACC.
Implications for Clinical Care
Adrenocortical carcinoma is one of the rarer cancers worldwide. Its late presentation makes it difficult to treat, and while surgical resection is the primary management, no therapeutic options have been proven effective to date. However, the use of pembrolizumab, either alone or in combination with mitotane, has shown a certain response in advanced ACC. In our case, after our patient presented with metastasis to the perinephric space, and after 4 cycles of pembrolizumab with mitotane, complete radiological response was attained. To our knowledge, this is the first case of recurrent metastatic ACC, with negative prognostic markers, and no prior radiotherapy, which had complete radiological response to a combination therapy of mitotane and pembrolizumab.
We therefore suggest the need for a clinical trial to study the combination of pembrolizumab and mitotane in the treatment of recurrent metastatic cases of ACC. In addition, better prognostic markers need to be identified for ACC to guide appropriate therapy. Microsatellite status, tumor burden, TAM density and type (M1/M2), immunoscore, and regulatory T-cells are all markers that have been explored in other types of cancer, but data regarding their utility in ACC is scarcely available, with immunoscore only calibrated for colorectal cancer.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Dr. Alam contributed to the data collection, data analysis, literature review and writing of the manuscript.
Dr. Bouferraa and Dr. Haibe contributed to the data collection, data analysis and writing of the manuscript.
Dr Shamseddine contributed to the design and concept of the work, writing of the manuscript and critical revision of the content.
All authors approved the final version and take public responsibility for the appropriate portions of the content.
Ethical Approval
The American University of Beirut (AUB) Institutional Review Board (IRB) does not require approval for any case reports with less than 4 clinical cases. As this case report has only one clinical case, it does not meet the definition of human subject research as defined by DHHS and USFDA regulations, and therefore, does not require approval by the institution’s Institutional Review Board. For more information, please contact
Patient Consent
Written informed consent was obtained from the patient for authorization to publish their clinical information in this case report.