
Abstract
Introduction
Large cell neuroendocrine carcinoma of the cervix (LCNEC), a rare and aggressive malignancy, has poor survival. Due to the scarcity of specific treatment guidelines and the limitations of small retrospective studies, this study aims to assess prognostic factors and treatment outcomes in cervical LCNEC using data from both the SEER database and a Chinese multicenter registry.
Methods
This retrospective multicenter cohort study included 130 patients diagnosed with cervical LCNEC between 2004 and 2021, including 87 from the SEER database and 43 from the Chinese registry. We compared clinicopathological variables, treatment approaches such as surgery, chemotherapy, radiotherapy and survival outcomes. Kaplan-Meier and Cox regression analyses were employed to identify prognostic factors.
Results
The Chinese cohort exhibited a lower proportion of metastatic cases (13.95% compared to 49.43%, p<0.001), earlier disease stages (AJCC IV: 13.95% vs. 49.43%, p<0.001), and higher rates of surgery (76.74% vs. 56.32%, p=0.023) and chemotherapy (93.02% vs. 83.91%, p=0.147). The median overall survival was 22.0 months (95% CI: 17.0–29.5), with the Chinese cohort demonstrating superior 5-year survival (44.0% vs. 27.3%, p<0.001). Surgery was found to reduce the risk of mortality in both cohorts, particularly for locally advanced disease. Chemotherapy improved survival in the SEER cohort, while radiotherapy showed no significant benefit. Advanced T-stage and nodal involvement were identified as predictors of poor prognosis.
Conclusion
Surgery and chemotherapy remain cornerstone interventions for survival improvement, with surgical resection showing particularly pronounced benefits in locally advanced cases. Prospective studies are needed to optimize guidelines.
Keywords
Introduction
Cervical cancer remains a considerable global health concern, with an estimated 661,021 new cases and 348,189 deaths in 2022, even with advances in HPV vaccination and screening. 1 Among its histological varieties, neuroendocrine carcinomas (NECs) of the cervix are exceptionally uncommon and aggressive, comprising less than 2% of invasive cervical cancers.2-4 Large cell neuroendocrine carcinoma of the cervix (LCNEC), a distinct NEC subtype, is notable for its high mitotic rate, rapid progression, and early lymphovascular invasion and distant metastasis.5,6 Compared to more prevalent squamous cell carcinoma or adenocarcinoma, LCNEC has a significantly poorer prognosis, with reported 5-year survival rates below 25% even in early stages.7,8
Current treatment approaches for LCNEC are often based on guidelines for neuroendocrine carcinoma or other aggressive cervical cancers. The NCCN guidelines recognize the distinctiveness of neuroendocrine tumors but offer limited stage-specific therapy guidance for LCNEC. 9 Currently, the prevailing treatment approaches include surgery, chemotherapy, and radiotherapy.4,10 Radical surgery combined with chemotherapy stands as the prevalent choice, particularly for patients with resectable tumors in the early stage.10,11 However, their precise impact on prognosis remains unclear, with conflicting findings reported in current studies.12-15
The scarcity of LCNEC has impeded the conduct of prospective clinical trials, resulting in significant evidence-based management gaps. Existing studies are often single-center, small-scale, or variably designed, limiting their broader applicability.8,11 Additionally, LCNEC’s biological behavior and treatment response may differ from other neuroendocrine subtypes, necessitating targeted research. 16 Large-scale, multi-institutional studies are urgently required to clarify prognostic factors, refine treatment algorithms, and validate stage-specific interventions.
In this study, we undertook a retrospective analysis, integrating data from the SEER database and a Chinese multi-center registry. Our aim was to assess the influence of different factors on survival outcomes in cervical LCNEC. By combining two geographically distinct patient groups, we hoped to identify tailored treatment strategies and contribute evidence to enhance clinical guidelines for this underserved malignancy.
Methods
Patient Selection
In this retrospective study, we utilized data from a multi-center registry in China and the Surveillance, Epidemiology, and End Results (SEER) database. The Chinese registry comprised data on patients with LCNEC diagnosed between January 1, 2004, and December 31, 2021, at Fujian Cancer Hospital and Shandong Cancer Hospital. Inclusion criteria were a pathological diagnosis of primary LCNEC (based on the WHO Classification of Tumors of Female Reproductive Organs, with ICD-O-3 code 8013/3). Exclusion criteria were non-primary tumors (such as metastatic carcinomas) and cases without complete survival information.
Using the SEER database of the National Cancer Institute (NCI) (SEER*Stat Database: Incidence - SEER Research Data, 22 Registries, Nov 2023 Sub [2000-2021] - Linked To County Attributes - Time Dependent [1990-2022] Income/Rurality, 1969-2022 Counties, National Cancer Institute, DCCPS, Surveillance Research Program, released April 2024, based on the November 2023 submission), we selected patients diagnosed with cervical LCNEC between January 1, 2004, and December 31, 2021, to form the SEER cohort. Cases were limited to those with a primary site of the cervix (ICD-O-3 codes: C53.0, C53.1, C53.8, C53.9) and a histologic code (ICD-O-3 code) of 8013/3 (large cell neuroendocrine carcinoma). All patients required pathological confirmation and complete survival data. Patients without primary tumors were excluded.
Statistical Analysis
Descriptive statistical analysis was used to analyze the data. The baseline categorical characteristics were compared between different groups (SEER database group and Chinese registry group, surgery group and non-surgery group) using the χ2 test or Fisher’s exact test. The overall survival (OS) from diagnosis to death from any cause or last follow-up was evaluated. The final follow-up date for survival analyses was April 10, 2025. Kaplan-Meier method was used to construct survival curves, and the log-rank trend test was employed to determine the statistical significance of differences in Kaplan-Meier survival.
The Cox proportional hazards model was utilized for both univariate and multivariate survival analyses. All variables (Year of diagnosis, Age, Marital status, Tumor size, AJCC 8th stage, FIGO 2018th stage, Surgery, Radiation, Chemotherapy) were included in the univariate Cox regression analyses. Variables that significant in the univariate analyses or clinically considered to affect patient prognosis were incorporated into the multivariate Cox regression analyses. Hazard ratios (HR) were reported with 95% confidence intervals (CI). All tests were two-sided, and a p-value < 0.05 was considered statistically significant. All statistical analyses were performed using R (version 4.3.2).
Ethics Statement
This retrospective multicenter cohort study was conducted in accordance with the Declaration of Helsinki as revised in 2024. The reporting of this study conforms to the STROBE guidelines. 17 Ethical approval was obtained from the Institutional Review Board at Fujian Provincial Cancer Hospital (approval No. K2024-206-01; approval date: June 12, 2024). Written informed consent was obtained from all patients in the Chinese multi-center registry. The SEER database contains de-identified publicly available data and therefore did not require additional institutional ethics approval or informed consent for secondary analysis. All patient details were de-identified before analysis. Patients from the Chinese multi-center registry were included consecutively during the study period.
Results
Clinicopathological Features
Patient Demographics and Baseline Characteristics From the SEER Database and Chinese Registry

1n (%); Mean ± SD; Median (IQR).
2Pearson’s Chi-squared test.
3Welch Two Sample t-test.
4Fisher’s exact test.
Survival and Prognostic Factor Analyses
The Median Survival Rate of Patients From the SEER Database and Chinese Registry
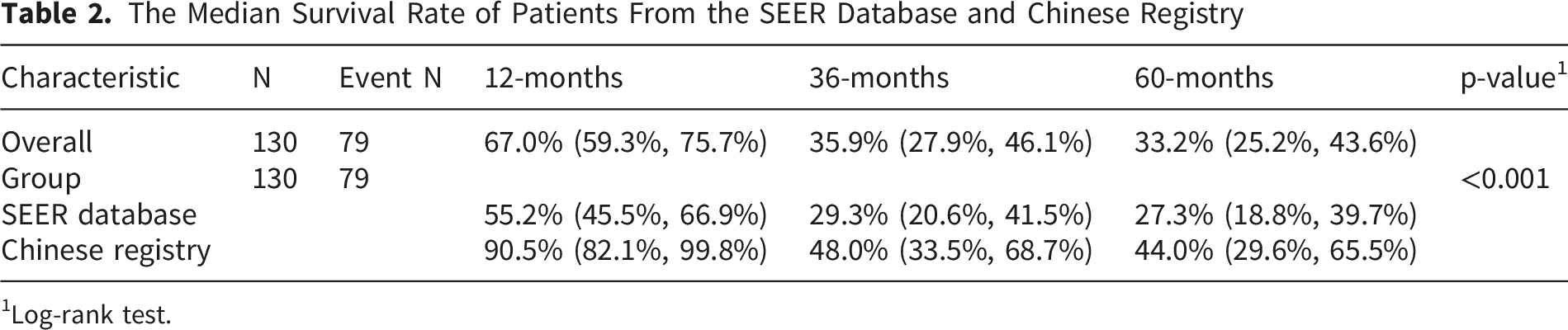
1Log-rank test.
In the univariate Cox regression analyses, tumors exceeding 40 mm in size were tied to a heightened mortality risk in the SEER cohort (HR 4.30; 95% CI 1.64–11.29; p=0.003), though not in the Chinese cohort. Advanced T stages (T2, T3, T4) indicated a poorer prognosis in both groups. In the SEER cohort, nodal involvement (N1 vs N0) was associated with a higher mortality rate (HR, 3.43; 95% CI, 1.98–5.94; p<0.001). FIGO 2018th stages II, III, and IV demonstrated notable or marginally significant correlations with mortality compared to stage I in the SEER cohort. Surgery proved to be a significant protective factor in both cohorts, reducing mortality risk. Chemotherapy showed a marginally beneficial effect in the China cohort and a significant one in the SEER cohort. Radiation therapy, however, had no significant impact on mortality in either group.
In the multivariate analyses, after adjusting for confounders, no factors were significantly associated with mortality in the Chinese registry. However, in the multivariate analyses of SEER database, patients with higher T stage exhibited substantially increased mortality risk, with T3 (HR, 6.18; 95% CI, 2.70-14.15, p<0.001), T4 (HR, 13.30; 95% CI, 4.03-43.93, p<0.001) showing progressively greater hazards compared to T1. Surgical intervention significantly reduced mortality risk (HR, 0.30; 95% CI, 0.16-0.57, p<0.001), as did chemotherapy receipt (HR, 0.30; 95% CI, 0.13-0.68, p=0.004). The forest plots of the results of the multivariate analyses are shown in Figures 1 and 2. The results of univariate Cox regression analyses are shown in Table 3 and Table 4. Forest plot of multivariate cox regression analyses in the SEER database Forest plot of multivariate cox regression analyses in the Chinese registry Univariate and Multivariate Analysis of Patients From SEER Database 1HR = Hazard Ratio, CI = Confidence Interval. 2*p<0.05; **p<0.01; ***p<0.001. n = 87.0; N events = 60.0; statistic.log = 83.1; p.value.log = 0.000; statistic.sc = 94.5; p.value.sc = 0.000; statistic.wald = 67.5; p.value.wald = 0.000; statistic.robust = NA; p.value.robust = NA; R2 = 0.615; r.squared.max = 0.995; c-index = 0.824; c-index SE = 0.022; Log-likelihood = -190; AIC = 402; BIC = 425; No. Obs. = 87. Univariate and Multivariate Analysis of Patients From Chinese Registry 1HR = Hazard Ratio, CI = Confidence Interval. 2*p<0.05; **p<0.01; ***p<0.001. n = 43.0; N events = 19.0; statistic.log = 30.7; p.value.log = 0.001; statistic.sc = 32.8; p.value.sc = 0.001; statistic.wald = 16.1; p.value.wald = 0.138; statistic.robust = NA; p.value.robust = NA; R2 = 0.510; r.squared.max = 0.943; c-index = 0.842; c-index SE = 0.044; Log-likelihood = -46.1; AIC = 114; BIC = 125; No. Obs. = 43.



Surgical Intervention on Survival
Baseline Characteristics of Patients Stratified by Surgery Status

1n (%); Mean ± SD; Median (IQR).
2Pearson’s Chi-squared test; Welch Two Sample t-test; Fisher’s exact test; Wilcoxon rank sum test.
3Fisher’s exact test; Welch Two Sample t-test; Wilcoxon rank sum test.

(A) Kaplan-Meier Survival Curves Stratified by Surgery Status in Locally Advanced patients of SEER Database; (B) Kaplan-Meier Survival Curves Stratified by Surgery Status in Locally Advanced patients of Chinese Registry
To further explore the prognostic value of surgery across disease stages, Kaplan–Meier survival analyses were performed stratified by FIGO 2018 stage (I–II vs. III–IV) in both the SEER and Chinese multi-center cohorts (Figures 4 and 5). Kaplan–Meier overall survival curves comparing surgical vs. non-surgical treatment in SEER patients stratified by FIGO 2018th stage: (A) Stage I–II; (B) Stage III–IV Kaplan–Meier overall survival curves comparing surgical vs. non-surgical treatment in the Chinese registry stratified by FIGO 2018th stage: (A) Stage I–II; (B) Stage III–IV

In the SEER cohort, no significant survival difference was observed between surgical and non-surgical patients with stage I–II disease (P=0.350). However, in stage III–IV patients, surgical treatment was associated with a markedly improved overall survival (P<0.001). A similar pattern was observed in the Chinese cohort: surgery did not confer a significant survival benefit in early-stage patients (P=0.560), while a significant improvement in overall survival was noted among stage III–IV patients (P=0.035).
Discussion
SCNEC accounts for only a very small proportion of cervical cancers, whereas SCC remains the predominant histologic subtype. Consistently, survival outcomes of cervical neuroendocrine carcinomas, including SCNEC, are substantially worse than those of SCC in database-based analyses. 8 Current evidence for cervical LCNEC is limited, its clinical management is largely derived from the broader experience with cervical neuroendocrine carcinoma, especially small cell neuroendocrine carcinoma. However, LCNEC is not completely interchangeable with SCNEC and may differ in clinicopathological features, biological behavior, and therapeutic responsiveness. This highlights the importance of LCNEC-specific studies.8,18 This study represented the systematic evaluation of prognostic factors and therapeutic strategies for LCNEC through integration of the SEER database with multi-center registry data from China. The results demonstrated that surgery and chemotherapy served as pivotal interventions for survival improvement, with surgery demonstrating particularly significant benefits in locally advanced patients.
The Chinese cohort demonstrated significantly superior survival outcomes compared to the SEER cohort. This disparity may stem from multiple factors. The predominant determinant was likely the higher proportion of metastatic cases in the SEER cohort. This between-cohort difference should be interpreted cautiously because the baseline stage distribution differed markedly between the two datasets. This observation aligned with findings from multinational comparative studies on small cell cervical carcinoma, further underscoring the clinical imperative for early detection and intervention. 19
Our study demonstrated that surgery significantly reduced the mortality risk in patients with LCNEC. This finding was consistent with previous studies on cervical neuroendocrine carcinoma.20,21 In the SEER cohort, locally advanced patients accepted surgery exhibited markedly prolonged median survival, supporting the pivotal role of surgery in disease control. Notably, although NCCN guidelines favored non-surgical approaches for locally advanced cervical cancer, our findings suggested that LCNEC may possess distinct biological behaviors, and its aggressive nature might be effectively controlled through surgery.9,18 Our stage-stratified analyses indicate that the survival benefit of surgery is concentrated in patients with FIGO stage III–IV LCNEC. This pattern reflects a well-established principle from advanced epithelial ovarian cancer, in which reducing macroscopic tumor burden improves outcomes when combined with systemic therapy. Randomized trials (EORTC 55971 and CHORUS) demonstrated that neoadjuvant chemotherapy followed by interval debulking is non-inferior to primary debulking followed by chemotherapy, underscoring that the extent of residual disease—rather than the sequence of surgery—determines prognosis; the primary objective of cytoreduction is to achieve no macroscopic residual disease.22,23 By analogy, LCNEC is a highly proliferative tumor with early metastatic potential, and debulking surgery may augment systemic therapy by reducing total tumor burden and chemo-resistant subclones, removing poorly perfused or sanctuary sites less accessible to chemotherapy or radiation, and improving performance status and symptom control to facilitate timely administration of full-dose multi-agent chemotherapy. 24 Contemporary retrospective evidence in cervical neuroendocrine carcinoma, including LCNEC, supports multimodal therapy and suggests an association between surgery—particularly when combined with platinum/etoposide—and improved survival, although effect sizes vary across series and stages. Given the rarity of LCNEC and the absence of randomized trials, the current evidence derives from retrospective cohorts, registries, and multicenter series. We therefore propose a conditional recommendation to consider aggressive cytoreductive surgery in carefully selected stage III–IV LCNEC patients as part of multimodal therapy, typically with platinum-based chemotherapy.25,26
The survival advantage of chemotherapy was validated in the multivariate analyses, which aligned with the findings reported by Embry et al 2 27 Platinum-based agents suppressed tumor proliferation by inducing DNA crosslinking, while etoposide enhanced their cytotoxicity. The synergistic effect of these agents may improve distant metastasis control. 28 In the Chinese cohort, the majority of patients were subjected to chemotherapy, which may partially account for the observed survival benefit. Notably, radiotherapy did not demonstrate significant survival benefits in this study, potentially due to insufficient sample size or suboptimal timing of radiotherapy. Further research is warranted to optimize the role of radiotherapy in multimodal treatment strategies.
We found that T stage and lymph node metastasis were identified as independent prognostic factors, which was consistent with the highly aggressive nature of neuroendocrine carcinoma, characterized by its propensity for early invasion into parametrial tissues and the vascular system. 29 Notably, even in early-stage patients, the median survival time was only 19 months, significantly lower than that of conventional cervical cancer, highlighting the distinct malignant biological behavior of LCNEC. The associations of tumor size and stage with survival appeared less stable in the Chinese cohort than in the SEER cohort. This discrepancy should be interpreted cautiously and is likely related to the relatively small sample size and limited number of outcome events in the Chinese registry, which may have reduced statistical power and widened confidence intervals. Therefore, the absence of consistent significance in the Chinese cohort should not be interpreted as evidence of no prognostic effect, but rather as an indication that these estimates require validation in larger multicenter datasets. Further exploration of molecular biomarkers to guide risk stratification is warranted. Bellone et al 3 30 revealed through integrated genomic analyses that high-frequency alterations in high-grade neuroendocrine carcinoma of the cervix (HGNECC) include activation of the PI3K/AKT/mTOR pathway, EGFR amplification, and mutations in ATR/ATM pathway-related genes. Preclinical models demonstrated that copanlisib (a PI3K inhibitor) combined with afatinib (an EGFR inhibitor) or elimusertib (an ATR inhibitor) significantly suppressed tumor growth, likely through synergistic blockade of DNA damage repair and pro-proliferative signaling pathways. This finding suggested that molecular subtype-based drug combination strategies may overcome drug resistance associated with conventional chemotherapy.
The synergistic effects between PARP inhibitors and immunotherapy are equally noteworthy. Carroll et al 3 31 demonstrated that the expression rates of PARP1/2 reached 89% in cervical neuroendocrine carcinoma, whereas the PD-L1 positivity rate was merely 21%. In PD-L1-negative patients, PARP inhibitors could enhance tumor cell sensitivity to DNA damage by inducing the “synthetic lethality” effect while simultaneously promoting tumor antigen release. The combination with PD-1/PD-L1 inhibitors may elicit an “abscopal effect.” Animal studies revealed that the combination of olaparib and pembrolizumab resulted in a reduction in tumor volume. 32 Additionally, the “molecular signature-driven therapy” strategy proposed by Manchana et al 3 33 emphasized that targeting specific molecular features such as MYC amplification and RB1 deletion with CDK4/6 inhibitors or EZH2 inhibitors may provide precise therapeutic options for rare subtypes.
Despite utilizing the largest sample size to date for LCNEC, this study had several limitations. The retrospective nature of the study introduced inherent selection biases, as evidenced by the surgical cohort comprising younger patients with smaller tumors, potentially leading to overestimation of surgical efficacy. Furthermore, the SEER database lacked detailed chemotherapy regimen information (e.g., platinum dosage, number of cycles), which limited the assessment of chemotherapy intensity. The relatively short follow-up duration in the Chinese cohort may result in underestimation of long-term recurrence risk.
Conclusion
In summary, this study suggests that surgery and chemotherapy remain important components of treatment for cervical LCNEC, while surgical intervention may provide survival benefit in selected patients within a multimodal treatment framework. However, these findings should be interpreted cautiously given the retrospective design, the marked between-cohort differences in stage distribution, and the limited number of advanced-stage cases in the Chinese cohort. Further large-scale prospective studies are warranted to validate these findings and refine treatment strategies.
Supplemental Material
Supplemental material - The Prognosis of Patients With Large Cell Carcinoma of the Cervix: A Retrospective Study of the SEER Database and a Chinese Multi-Center Registry
Supplemental material for The Prognosis of Patients With Large Cell Carcinoma of the Cervix: A Retrospective Study of the SEER Database and a Chinese Multi-Center Registry by Yaxin Kang, Liangwu Zhuang, Lele Chang, Jing Liu, Cong Wang and Qin Xu in Cancer Control.
Footnotes
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki as revised in 2024. Ethical approval was obtained from the Institutional Review Board at Fujian Provincial Cancer Hospital (approval No. K2024-206-01; approval date: June 12, 2024).
Consent to Participate
Written informed consent was obtained from all patients in the Chinese multi-center registry. For the SEER cohort, informed consent was not required because all data were de-identified and publicly available.
Consent for Publication
All the authors agreed to publish this work.
Author Contributions
YK and LZ proposed the main idea and drafted the initial version of the manuscript. LC and YK conducted the data analysis and data interpretation, while LZ and JL were responsible for data collection and validation. JL and CW conducted the data visualization and validation. QX and CW provided guidance on the methodology and structure of the article. QX and JL contributed to funding acquisition. QX and CW has carefully polished and revised the overall article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Fujian Cancer Hospital High-Level Talent Training Program (Grant number: 2023YNG09), Joint Funds for the innovation of science and Technology, Fujian province (Grant number: 2023Y9449), Natural Science Foundation of Fujian Province (Grant number: 2024J011099 and 2023J011273).
Declaration of Conflicting Interests
The authors declare that there were no potential conflicts of interest in this research.
Data Availability Statement
The data supporting this study’s findings are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.