
Abstract
Objectives:
Hyponatraemia represents a negative prognostic factor in patients with cancer. The aim of this study was to assess, for the first time, the role of hyponatraemia in patients undergoing radical surgery for pancreatic ductal adenocarcinoma.
Methods:
A total of 89 patients with stage I-III pancreatic ductal adenocarcinoma underwent radical surgery between November 2012 and October 2014. Relapse-free survival (RFS) and disease-specific survival (DSS) were estimated using Kaplan-Meier method. A Cox regression model was carried out for univariate and multivariate analyses. Fisher exact test was used to estimate correlation between variables.
Results:
In total, 12 patients (14%) presented with hyponatraemia at diagnosis. The median DSS was 20 months in patients with hyponatraemia and not reached in patients with eunatraemia (P < .1073), while a statistical significant difference was observed in terms of median RFS (10 months vs 17 months, respectively; P = .0233). Considering clinical features (hyponatraemia, smoke and alcoholic habit, diabetes, pain, and jaundice), patients with 4 or more of these factors had a worse prognosis (mDSS: 30 months vs not reached; hazard ratio [HR]: 0.40, 95% confidence interval [CI] = 0.16-0.80; P = .0120).
Conclusions:
The presence of hyponatraemia and its prompt correction at the diagnosis time should be considered for the correct management of patients with pancreatic carcinoma.
Introduction
Pancreatic ductal adenocarcinoma (PDAC) represents the seventh leading cause of adult cancer death with a rising incidence. In 2008, more than 270 000 new cases were diagnosed globally, 1 while Globocan estimates 458 918 new diagnoses all over the world in 2018, with an age-standardized incidence rate increase of 1.03% per year between 1973 and 2014. 2 Even though most patients present with an advanced disease and resection rate is under 20%, 3 better outcomes are seen in patients who undergo radical surgery at specialized centres. 4 Literature reports a 5-year survival for surgery alone in between 8% and 10%, 5 which can be increased up to 21% in patients receiving adjuvant chemotherapy as fluorouracil (FU) and folinic acid 6 or gemcitabine 7 or FOLFIRINOX. 8 During the last 2 decades, an improvement in terms of survival was observed, mostly due to improvement of therapies and a more accurate patient selection for surgery.9-11 As suggested by Labori et al, 10 multimodality treatment improves survival in patients with PDAC and it seems strongly associated with reduced mortality risk in patients with resectable PDAC. The most universally accepted therapy remains surgery, but it is not the only one. Moreover, the outcome of radically resected patients is influenced by many prognostic factors, such as age, pain, weight loss, splenic artery invasion, Ca19.9 preoperative value, tumour size, high tumour grading, surgical margin status, lymph node status, adjuvant therapy, and molecular features.11-14
According to recent evidences, hyponatraemia, the most common electrolyte disorder in the oncology setting, seems to be considered a negative prognostic factor in patients with cancer, especially in those with lung cancer, 15 pleural mesothelioma, 16 renal cell carcinoma, 17 gastrointestinal cancer,18-20 and lymphoma. 21 Hyponatraemia has also been reported to be an important predictor of poor response to chemotherapy and target therapy 22 and negatively correlates with performance status. 23 Recent studies also showed that an effective and timely normalization of serum sodium levels might lead to a positive effect on prognosis of patients with cancer. 24 However, the prognostic role of hyponatraemia in patients with pancreatic cancer has not been investigated yet. In this study, we aimed to assess for the first time the prognostic role of pretreatment hyponatraemia in patients with radically resected pancreatic cancer.
Materials and Methods
The study population included adult patients with histologically confirmed diagnosis of PDAC who have undergone radical pancreatoduodenectomy (PD), distal pancreatectomy (DP), or total pancreatectomy (TP) at the Department of Pancreatic Surgery of Università Politecnica delle Marche – Azienda Ospedaliero Universitaria Ospedali Riuniti ‘Umberto I – G.M. Lancisi – G. Salesi’ di Ancona between November 2012 and October 2014. For the inclusion criteria, all patients must be referred to the Department of Oncology of the same institution. For all patients, demographics, pathological examinations, operative details, and postoperative outcomes were prospectively collected in an institutional database and retrospectively analysed. In case of PD, a pylorus-preserving procedure was always performed. Reconstruction of the pancreatic remnant was always performed with end-to-side pancreatico-jejunostomy (PDPJ) and a duct-to-mucosa (PDDTM) anastomosis. All operations were performed with laparotomy. According to Italian law (resolution March 1, 2012, Gazzetta Ufficiale n.72 of March 26, 2012), ethics approval and informed consent were not required for this study owing to its retrospective nature, the use of anonymous data, and the fact that it was not associated with any change in patients’ management. All procedures performed in the study were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All patients gave their written consent to all the diagnostic-therapeutic procedures.
Perioperative management
Postoperative management of patients did not include any specific protocol. Prophylactic octreotide was administered to prevent pancreatic fistula (PF) only in those patients who underwent PD. A fistula predictive model based on amylase value in drain (AVD) measured in postoperative day 1 (POD 1) and postoperative day 5 (POD 5) was used for the management of drains. 25 Postoperative mortality was defined as any death within 90 days of resection. Pancreatic fistula was defined according to the International Study Group of Pancreatic Fistula (ISGPF) guidelines 26 and classified as grade A, B, or C. Hyponatraemia was defined as serum sodium level lower than 135 mEq/L. High cholestatic indices were defined as elevated serum bilirubin (higher than 1.2 mg/dL), elevated alkaline phosphatase (>130 U/L), elevated gamma-glutamyl transferase (>45 U/L), and elevated serum transaminases (>45 U/L). Serum Ca19.9 level is defined as elevated when higher than 35 U/mL.
Pathological report
All pancreatic specimens were sampled and examined according to an internal protocol. Initially, R margin status was defined as ‘transection margin’ (namely a margin that can be surgically enlarged). Since then, our Pathological Department proceeded to a systematic reevaluation of all specimens according to a standardized internal protocol. According to this protocol, 9 margins were evaluated microscopically: biliary, pancreatic neck, and duodenal transection margins; anterior, posterior, superior, and inferior pancreatic margins; and superior mesenteric vein (SMV) groove and superior mesenteric artery (SMA) margin, which represent together the medial margin. To date, this protocol represents our clinical practice. At histological examination, the microscopic involvement of each surgical margin was evaluated and classified as follows: presence of malignant cells directly at the inked surface (standard R1), within less than 1 mm (R1 according to Verbeke) 27 or with a distance >1 mm (R0). Perineural invasion (PNI) and nodal status (N1) were analysed and described as present/absent. Other parameters were assessed and classified according the 7th ed. AJCC staging system. 28
Follow-up
A complete follow-up, including chest and abdomen computed tomography (CT) scan and tumour markers (CEA and Ca19.9), was performed every 6 months till December 2013. Long-term outcomes were evaluated as both disease-specific survival (DSS) and relapse-free survival (RFS). Disease-specific survival was defined as the time from surgery to death, irrespective of cause. Relapse-free survival was defined as the time from surgery to tumour recurrence. Patients without tumour recurrence or death at the time of the data cut-off for the analysis were censored at their last date of tumour evaluation.
Statistical analysis
The association between categorical variables was evaluated by Fisher exact test for binomial categorical variables and by chi-square test for all other applications. Relapse-free survival and DSS were estimated using Kaplan-Meier method with Rothman 95% confidence intervals (CIs) and compared across the groups using the log-rank test. Hyponatraemia was assessed within 1 week prior and after surgery. Potential factors associated with outcome were evaluated, including patients’ age, sex, tumour stage, perineural and perivascular invasion, alcoholic and smoking history, weight loss, pain, Ca19.9 levels, anaemia and cholestasis indices, and neoadjuvant or adjuvant therapy. All other significance levels were set at a .05 value and all P values were 2-sided. Significance level in the univariate model for inclusion in the multivariate final model was more liberally set at a .2 level.29,30 Statistical analyses were performed using MedCalc version 11.4.4.0 (MedCalc Software, Broekstraat 52, 9030 Mariakerke, Belgium).
Results
Patient characteristics
A total of 89 patients met the inclusion criteria; among these, 48 (54%) were males and 41 (46%) were females. The median age was 66 years (range, 47-81), almost half of patients were concurrent or former smokers (37 patients, 42%) and 22 (25%) patients admitted alcohol abuse. Most patients (74; 84%) received adjuvant chemotherapy while 6 (7%) underwent also radiotherapy. The main characteristics of the patients are reported in Table 1.
Patients’ characteristics.

Most patients received a PD (71; 80%). Postoperative complications were observed in 28 (31%) patients, and no postoperative mortality was reported. Hospital readmission was necessary for 10 (11%) patients. Main operative procedures, postoperative complications, and pathological features are reported in Table 2. Data regarding surgical margins status referred to ‘transection margin’ and R0-rate was 96%, but we also reported the evaluation of R parameter according to Verbeke classification (R1 < 1 mm). 27
Operative procedures, postoperative complications, and main pathological data.
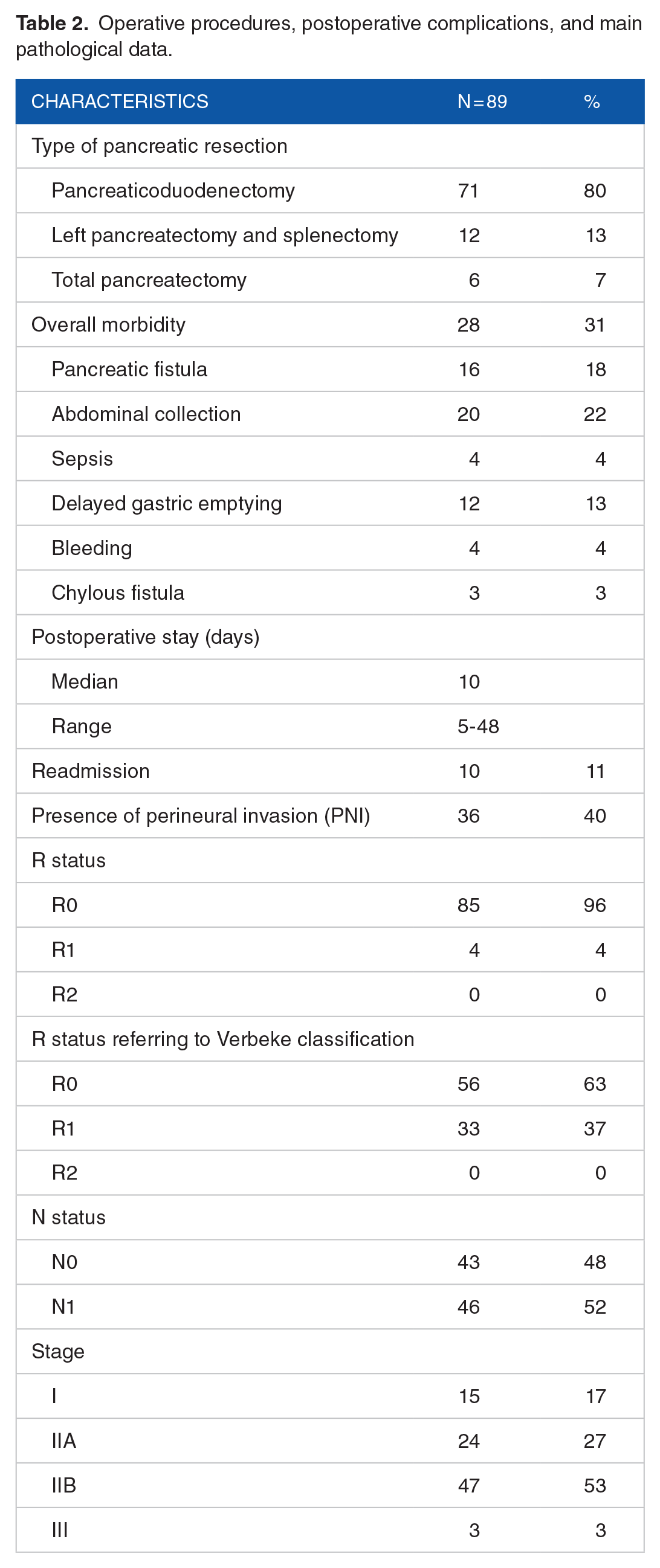
A total of 12 patients (13%) presented with preoperative hyponatraemia. No statistically significant difference was found for the incidence of preoperative hyponatraemia by dividing patients by stage. In particular, among the 15 patients with stage I, 2 of 15 (13.3%) patients had preoperative hyponatraemia. Among patients with stage II disease, respectively, 3 of 24 (12.5%) and 7 of 47 (16.7%) had preoperative hyponatraemia. None of the 3 patients with stage III disease presented the electrolyte disorder.
Most patients reported preoperative elevated serum bilirubin (55; 62%) and high cholestatic indices (46, 52%). Main laboratory data are reported in Table 3. Among the 12 patients with hyponatraemia, data regarding preoperative serum bilirubin resulted slightly lower than the value reported in total population with only 6 patients out of 12 (50%) presented elevated levels (vs 62% in total population).
Preoperative and postoperative laboratory data (normal values: AST: 0-40 U/L, ALT: 0-40 U/L, ALP < 130 U/L, total serum bilirubin < 1.2 mg/dL, serum sodium 135-145 mEq/L).

Disease-specific survival
Median DSS (mDSS) from surgery was not reached in the overall population. In total, 18 patients (20%) died during their follow-up, all of them died of tumour recurrence.
mDSS was 33 months in patients with high serum Ca19.9 and not reached in patients with normal serum level; however, the difference was not statically significant (P = .305). No statistical difference was observed in terms of mDSS between patients with preoperative hyponatraemia and patients with eunatraemia (mDSS = 20 months vs not reached, P = .1073), even if an unfavourable trend for patients with hyponatraemia was observed (Figure 1A). Based on the presence of symptoms at diagnosis, the mDSS was 22 months in patients complaining tumour-related pain and 35 months in patients without pain (hazard ratio [HR]: 0.46, 95% CI: 0.17-0.89; P = .0261) (Figure 1B). Stratified by length of hospital stay, mDSS was 29 months in patients who stayed at hospital more than 10 days and 35 months for 10 or less days (HR: 3.22, 95% CI: 1.49-6.22; P = .0022) (Figure 1C).
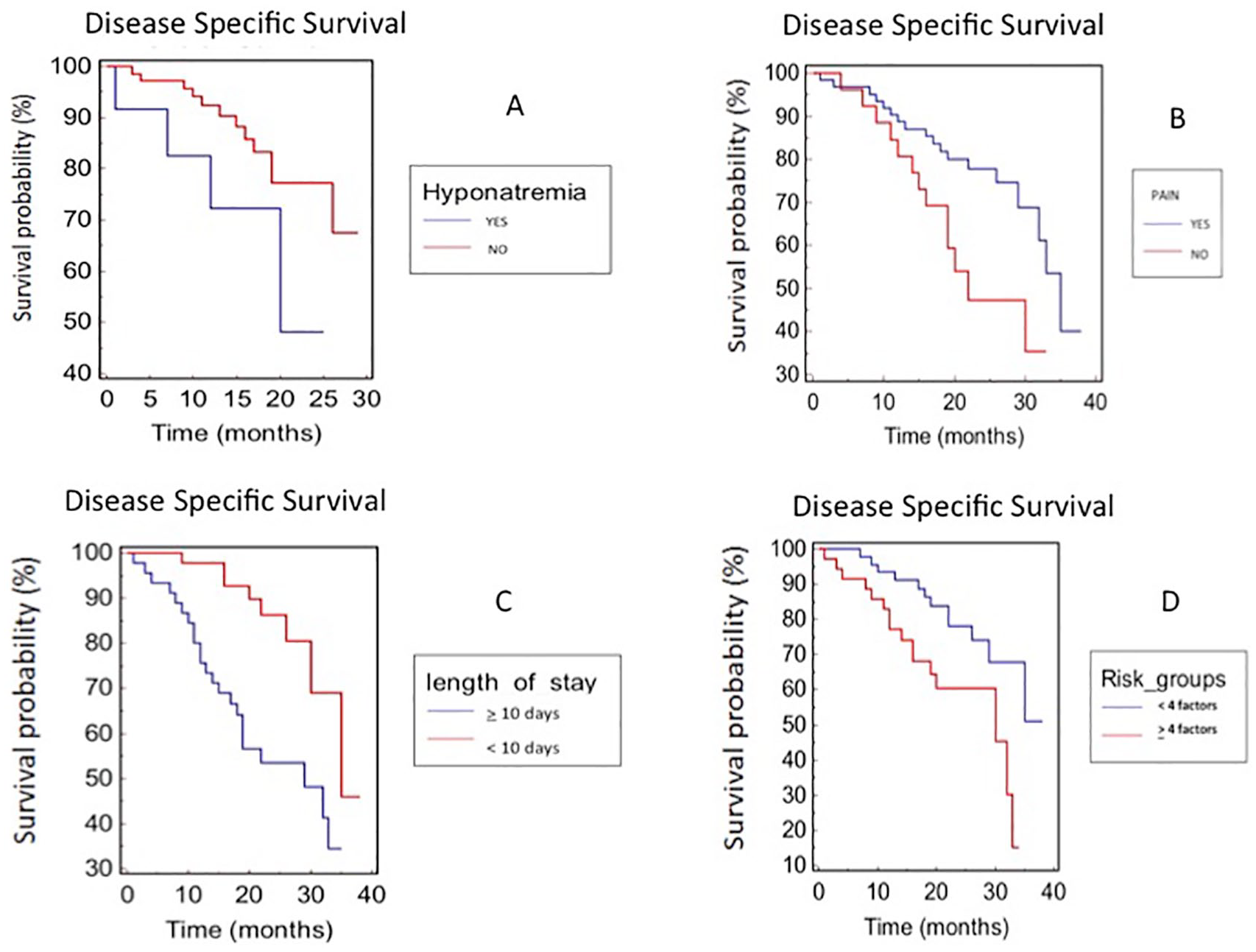
Disease-specific survival (DSS) stratified by (A) hyponatraemia, (B) pain, (C) length of stay, and (D) presence of risk factors in patients with radical resected pancreatic cancer.
Stratifying patients by sex, smoke and alcoholic habit, weight loss, diabetes, anaemia, elevated cholestatic indices, and histological tumour characteristics (nodal status, perivascular and perineural invasion, tumour stage), no statistical differences were detected.
Considering clinical features (hyponatraemia, smoke and alcoholic habit, diabetes, pain, and jaundice), patients with 4 or more of these factors had a worse prognosis (mDSS 30 months vs not reached; HR: 0.40, 95% CI: 0.16-0.80; P = .0120) (Figure 1D).
At multivariate analysis, length of hospital stay and pain at diagnosis were both predictors of worse DSS (P = .0009).
Relapse-free survival
In the overall study population, median RFS (mRFS) was not reached. Median RFS was 10 months in patients with preoperative hyponatraemia and 17 months in patients with eunatraemia (HR: 2.95, 95% CI: 1.31-42.31; P = .0233) (Figure 2A). Considering symptoms at diagnosis, patients without diabetes had a significant lower risk of tumour recurrence, 25 months vs 21 months (HR: 0.45, 95% CI: 0.11-0.76; P = .0114) (Figure 2B). Among other lab parameters, only normal alkaline phosphatase was associated with longer RFS, 29 months vs 22 months for patients with elevated alkaline phosphatase (HR: 0.46, 95% CI: 0.14-0.98; P = .0450) (Figure 2C).

Relapse-free survival (RFS) stratified by (A) hyponatraemia, (B) diabetes, (C) presence of elevated ALP, and (D) presence of risk factors in patients with radical resected pancreatic cancer.
Stratifying patients by sex, smoke and alcoholic habit, weight loss, diabetes, anaemia, elevated cholestatic indices, histological tumour characteristics (nodal involvement, perivascular and perineural invasion, tumour stage), elevated serum Ca19.9, and the presence of pain at diagnosis, no statistical differences were detected.
Considering the histopathological features (perivascular and perineural invasion, tumour stage, T, N) and lab parameters (hyponatraemia and elevated Ca19.9), patients with 3 or more of these factors had a higher risk of tumour relapse (18 months vs 25.5 months; HR: 2.52, 95% CI: 1.09-8.48; P = .0343) (Figure 2D).
At multivariate analysis, hyponatraemia, elevated alkaline phosphatase, and diabetes at diagnosis were predictors of worse RFS (P = .0052).
Correlation analysis
Using Fisher analysis, a statistical correlation between hyponatraemia and higher risk of hospital readmission was observed (P = .0063). Furthermore, statistical correlations between hyponatraemia and anaemia (P = .0016), hyponatraemia and elevated transaminases (P = .0226), and hyponatraemia and elevated alkaline phosphatase (P = .0413) were also observed.
Moreover, no correlation was observed between hyponatraemia and length of hospital stay (P = .5477) and other studied parameters (sex, smoke, alcoholic habit, weight loss, diabetes, jaundice and presence of pain at diagnosis, perivascular and perineural invasion, tumour stage, elevated serum Ca19.9).
Discussion
Hyponatraemia is the most common electrolyte disorder described in patients with cancer31,32 and emergent data seem to underline that its incidence seems to be underestimated.
33
The most common cause of hyponatraemia in patients with cancer is SIADH (syndrome of inappropriate antidiuretic hormone secretion), often due to ectopic production of arginine vasopressin (AVP) by tumours. Moreover, chemotherapy or other medications such as painkillers might precipitate this condition. In a retrospective study, hyponatraemia was described in approximately 50% of patients with advanced pancreatic carcinoma, but no data are available in earlier stages.
34
Some rare cases of ectopic antidiuretic hormone production were described in patients with pancreatic adenocarcinoma.35-37 We observed hyponatraemia in 14% of patients with early stages of pancreatic adenocarcinoma. Hyponatraemia has been identified as a negative prognostic and predictive factor in a number of different malignancies16,22,38-41 and a prompt and rapid normalization of this electrolyte disorder seems to improve the outcome of patients with hyponatraemic cancer.
42
Furthermore, hyponatraemia seems to be negatively associated with length of stay.
43
The role of preoperative hyponatraemia was investigated in patients with ovarian cancer, showing an increased risk of hospital stay of
However, this study has some limitations. First, it is a retrospective analysis of a small sample, which is therefore susceptible to bias in data selection and analysis. The strict selection of operated patients could explain the small number of the enrolled subjects. These aspects led to the selection of a study population with more favourable pathological features, as shown by the high rate of R0 (63% according to Verbeke), 27 high rate of N0 (48%), and low rate of perineural invasion (40%). Furthermore, hyponatraemia still remains an uncommon finding although it represents the most common electrolyte disorder in patients with cancer. Unfortunately, the small sample size does not allow us to validate our results and make concrete conclusions; therefore, our study might be considered as a hypothesis-generating research. Furthermore, no data concerning the management of hyponatraemia were available and therefore it is not possible to assess whether the normalization of serum sodium could have a reflection on the outcome of patients. Finally, concurrent drugs cannot be fully accounted to measure their influence, the origin, and the course of hyponatraemia.
Nevertheless, our results further suggest prognostic and predictive value of low serum sodium associated with other factors, in patients with pancreatic cancer who underwent radical surgery.
The presence of hyponatraemia along with other factors at the diagnosis should be considered for the correct management of patients with pancreatic cancer. Although further prospective studies are needed to assess its prognostic role, a prompt and effective correction of hyponatraemia should always be evaluated.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
RB and MF conceived the original idea and supervised the project. SR, GB, SP, SC and MT processed the experimental data, performed the analysis, drafted the manuscript and designed the figures. All authors reviewed the final manuscript.