
Abstract
Background:
Access to palliative care has been associated with improving quality of life and reducing the use of potentially aggressive end-of-life care. However, many challenges and barriers exist in providing palliative care to residents in northern and rural settings in Ontario, Canada.
Aim:
The purpose of this study was to examine access to palliative care and associations with the use of end-of-life care in a decedent cohort of northern and southern, rural and urban, residents.
Design:
Using linked administrative databases, residents were classified into geographic and rural categories. Regression methods were used to define use and associations of palliative and end-of-life care and death in acute care hospital.
Setting/Participants:
A decedent cancer cohort of Ontario residents (2007-2012).
Results:
Northern rural residents were less likely to receive palliative care (adjusted odds ratio [OR] = 0.90, 95% confidence interval [CI]: 0.83-0.97). Those not receiving palliative care were more likely to receive potentially aggressive end-of-life care and die in an acute care hospital (adjusted OR = 1.20, 95% CI: 1.02-1.41).
Conclusions:
Palliative care was significantly associated with reduced use of aggressive end-of-life care; however, disparities exist in rural locations, especially those in the north. Higher usage of emergency department (ED) and hospital resources at end of life in rural locations also reflects differing roles of rural community hospitals compared with urban hospitals. Improving access to palliative care in rural and northern locations is an important care issue and may reduce use of potentially aggressive end-of-life care.
Introduction
A palliative care approach for cancer patients facing life-threatening disease is essential and a critical component of the cancer control continuum. 1 Timely and comprehensive palliative care for patients and their caregivers offers many direct benefits including improving patient and family quality of life, mood, patient satisfaction, supporting preferred place of death, and possibly extended survival.2–5 In the past, palliative care was often initiated at end-stage disease and when life expectancy was short; however, recent research studies have demonstrated that the introduction of early comprehensive palliative care was associated with reducing or avoiding the use of potentially aggressive care at the end of life.5,6 Often considered less than ideal, aggressive end-of-life care has been characterized through system-level indicators such as administration of chemotherapy within the last 14 days of life, intensive care unit (ICU) admissions, multiple emergency department (ED) visits, and hospitalizations within the last 30 days preceding death.6,7 Although aggressive end-of-life care may be potentially increasing in occurrence, 7 this type of care is often not the preference of patients and their families 8 and can be associated with substantial costs to the health care system. 9
Many challenges exist for providing palliative care in a rural Canadian setting both for health care delivery and at the level of the palliative care recipient. 10 Previously published research references inequity issues of access to resources, lengthy travel to urban centers to obtain palliative services, as well as a lack of available health care professionals and health care resources.11–17 Furthermore, many rural residents often wish to receive care in their community with their families to avoid travel-related issues and costs. 18 Some additional barriers to accessing palliative care in rural areas also included lower socioeconomic status, a misunderstanding of what palliative care treatment is, and health care providers feeling ill-equipped to manage the care needs of patients nearing their end of life. 10 Moreover, the barriers that exist to access palliative care are not exclusive to rural Canada.10,19,20 A published literature review that included palliative care research studies from Australia, USA, Canada, and Europe indicated that barriers to access palliative care are all inclusive with the main distinguishing criteria being rurality. 10
There are more than 13 million residents in Ontario, Canada, and they receive universal health care delivered through a system of Local Health Integration Networks (LHINs). The 2 Northern LHINs contain more than 80% of the provincial land mass but only 6% of the Ontario population; approximately 30% of the Northern residents reside in rural areas (see Figure 121,22).
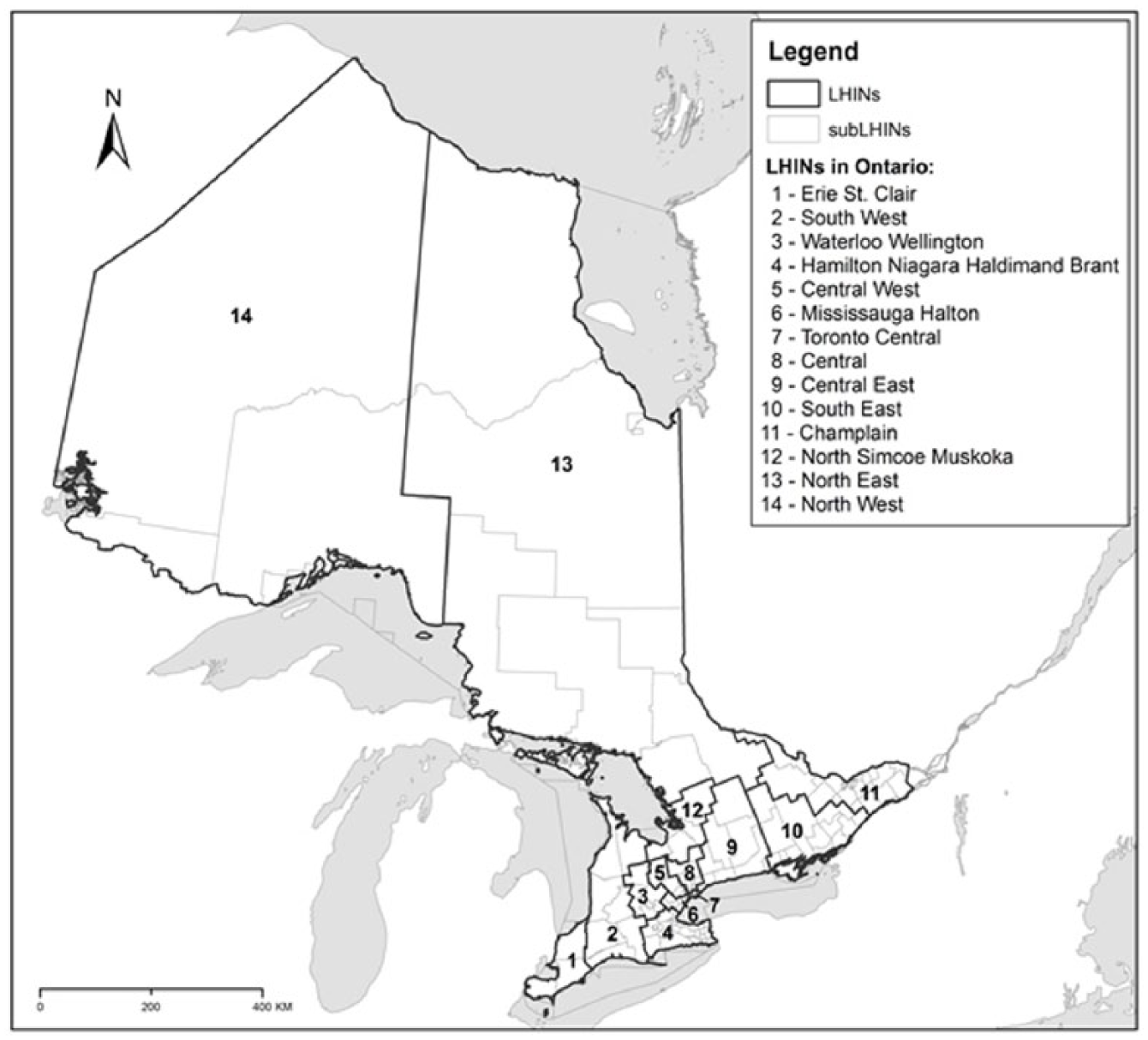
Map of Ontario Local Health Integration Networks (LHINs). The 2 Northern LHINs depicted in the map are 13-North East and 14-North West. All else constitutes southern Ontario LHINs.
There are a number of disparities related to health and health care for residents of northern and rural regions in Ontario that include shorter life expectancies, multiple long-term illness, premature death (before the age of 75 years) due to causes such as suicide, heart attack, stroke, pulmonary disease, and lung cancer—at rates much higher than the Ontario average for these diseases. 22 In addition, limited access to a primary care physician, increased travel to see a specialist when sick, as well as increased expense if required to travel out of town may result in people choosing not to seek care. 22
Using comprehensive administrative data available on all residents of Ontario, Canada, the primary purpose of this study was to describe access to palliative care and associations with the use of potentially aggressive end-of-life care in a decedent cancer cohort of Ontario residents with reference to rurality and location of residence.
Methods
Study design and cohort selection
This population-based retrospective study used administrative data to define a decedent cohort of all residents of Ontario, Canada who died from any cancer cause during 2007-2012. Ethics approval for this study was granted by the Research Ethics Board of Health Sciences North, project number 16-001 (January 2016 to present).
Data sources
We used administrative health databases managed by ICES to define the study cohort and variables of interest. Data were made available through the Ontario Cancer Data Linkage Project (“cd-link”). The cd-link is an initiative of the Ontario Institute for Cancer Research/Cancer Care Ontario Health Services Research Program, whereby risk-reduced coded data from the ICES Data Repository are provided directly to researchers with the protection of a comprehensive Data Use Agreement. 23 The Ontario Cancer Registry (OCR), a comprehensive population-based cancer registry,24,25 was used to identify residents of Ontario with a valid cancer diagnosis who had died of any cancer cause of death at least 30 days after initial diagnosis during 2007-2012. Diagnosed cancer cases were linked to the following administrative information sources: (1) the Ontario Health Insurance Plan (OHIP) to obtain information on physician services administered to Ontario residents, 26 (2) the Registered Person’s Database (RPDB) for demographic information on OHIP-eligible residents of Ontario, 27 (3) Statistics Canada 2006 Census profile for selected demographic information for residents of Canada, (4) the Canadian Institute for Health Information (CIHI) National Ambulatory Care Reporting System (NACRS) for information on all hospital-based ambulatory care ED visits, 28 (5) the CIHI Discharge Abstract Database (DAD) for information on hospital discharges, 29 and (6) the Home Care Database (HCD) for information on the use of home care services.
Main outcome measures
For each identified index case, we created a timeline of all codes and associated services from the date of primary cancer diagnosis through to death. Palliative care was defined following Cheung et al., 9 as the occurrence of two or more relevant billing codes located within the OHIP, HCD, and DAD databases, occurring at least 30 days apart and within the final year of life. Variables defined as potentially aggressive end-of-life care focused on events occurring within the last 30 days of life and included the use of chemotherapy within the last 14 days of life, an intensive care admission within the last 30 days of life (ICU), more than 1 ED visit within the last 30 days of life (ED), or more than one hospitalization in the last 30 days of life. 7 We also defined whether death had occurred in an acute care hospital through hospital discharge disposition codes.
Study variables
Time from diagnosis to death, cancer cause of death, and year of death data were provided by the OCR. Duration of disease was calculated as the time (in years) from primary diagnoses to death. Age and sex were provided from the RPDB. Income quintile was derived ecologically through a link of median income from Statistics Canada 2006 Census to patient postal codes defined from the RPDB using the PCCF+ version 5E. Rural or urban residence was defined according to Statistics Canada’s definition of rural which defines “rural” as communities with less than 10 000 people and not located near commuting zones of metropolitan areas. 30 We defined “urban” as all other areas. Northern residents were designated as those people residing within the 2 northern (North East and North West Ontario) LHINs, and all others as southern (which included densely populated areas located within Southern Ontario, such as Toronto, Ontario). We adopted this designation based on the recent health status report for Ontario’s North. 22 Cancer type was defined following the International Classification of Disease (ICD-10) listed for cause of death and included the following: breast (C50), lung (C34), colorectal (C18, C19, and C20), prostate (C61), and hematologic cancer (C91, C92, C93, C94, and C95). Unclassified cancers were grouped as “other.” We used the Deyo adaptation of the Charlson comorbidity index.31,32
Statistical analysis
Cohort characteristics were defined using descriptive statistics and frequencies. For each outcome variable, percentages were computed. Cross-tabulations were calculated using chi-square tests. Non-parametric Wilcoxon 2-sample tests were used to compare continuous variables, including duration of disease and Charlson index. Univariate and multivariate logistic regression models were used to determine crude and adjusted odds ratios (OR) and 95% confidence intervals (CI) for factors associated with having palliative care and with receiving any potentially aggressive end-of-life care. We assessed northern residence as a potential effect modifier of rurality using a likelihood ratio test. Trends over time were examined using Cochran-Armitage test for trend. All statistical analyses were conducted using STATA v12.1 33 and SAS v9.3 software. 34
Results
There were 129 107 Ontario individuals who died from cancer within the 6-year period from 2007 to 2012. From date of diagnosis through to death, almost 3 quarters (n = 95 685 or 74.11%) of the cohort received palliative care with 73.51% receiving a service in 2012. In a main effects model that included both rurality and geography, neither variable was significantly associated with palliative care when the results were fully adjusted (rurality adjusted OR = 0.98, 95% CI: 0.94-1.02; North adjusted OR = 0.99, 95% CI: 0.95-1.04). However, there was a significant interaction between these variables, which improved the overall model fit when included (likelihood ratio test
Associations of receipt of palliative care with demographic and clinical characteristics of Ontario residents who died from cancer (2007-2012).
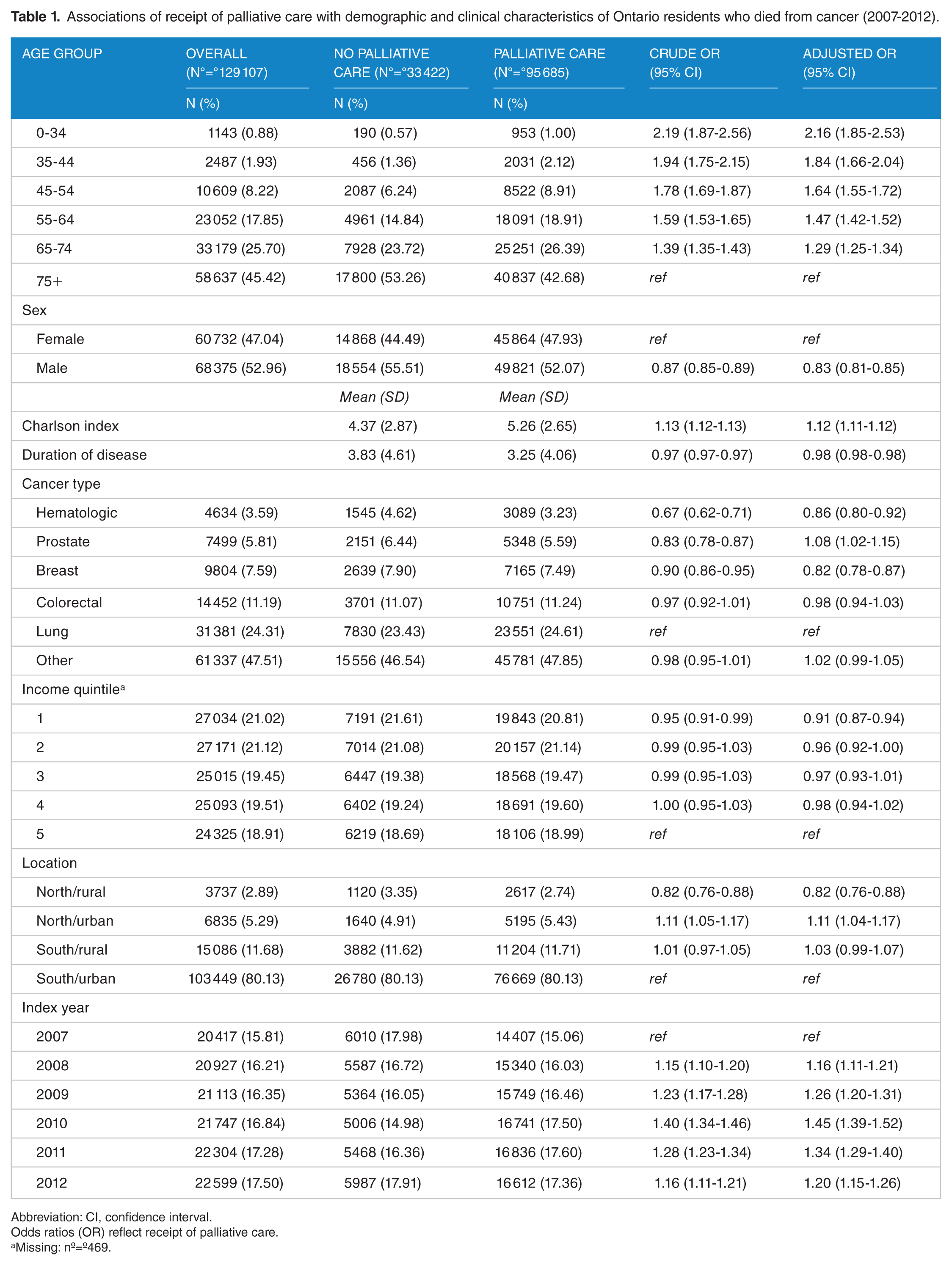
Abbreviation: CI, confidence interval.
Odds ratios (OR) reflect receipt of palliative care.
Missing: nº=º469.
Few cohort members (nº=º3737, 2.89%) resided in the north rural area of Ontario. A larger number (nº=º6835, 5.29%) resided in north urban areas; however, being from either northern residence only represented 8.18% of the cohort overall. North/Rural residents had significantly decreased odds of receiving palliative care compared with the referent group of South/Urban residents (adjusted OR = 0.82, 95% CI: 0.76-0.88). In adjusted analyses, other sociodemographic risk factors associated with decreased likelihood of receiving palliative care included male sex (adjusted OR = 0.83, 95% CI: 0.81-0.85), shorter duration of disease (adjusted OR = 0.98, 95% CI: 0.98-0.98), and lowest income quintile (adjusted OR = 0.91, 95% CI: 0.87-0.94). Younger age was associated with increased likelihood of receiving palliative care (adjusted OR = 1.29, 95% CI: 1.25-1.34 for the age group of 65-74 years compared with the referent age group of 75+ years; Table 1).
These persons not receiving palliative care were at significantly increased risk of receiving potentially aggressive end-of-life care (Table 2). For example, cohort members who had not received palliative care were significantly more likely to have multiple hospitalizations or ED visits within the last 30 days of life (adjusted OR = 1.71, 95% CI: 1.64-1.78 and adjusted OR = 1.66, 95% CI: 1.60-1.72, respectively) or to die in an acute care hospital (adjusted OR = 2.01, 95% CI: 1.96-2.07; Table 2, for North/Rural residents adjusted OR=1.20, 95% CI: 1.02-1.41).
Associations of receipt of potentially aggressive end-of-life care or death in acute care hospital.

Abbreviations: CI, confidence interval; ED, emergency department; ICU, intensive care unit.
Odds ratios (OR) reflect lack of palliative care.
Adjusted for all variables in Table 1.
Trends through time (2007-2012), and stratified analyses by geography, illustrate that decedents who did not receive palliative care had higher percentages of chemotherapy administered in the last 14 days of life (4.03%-5.61% compared with 2.90%-3.21% for the palliative group (Figure 2A); adjusted OR range 1.29 North/Rural to 2.36 North/Urban), ED visits (16.94%-19.98% compared with 12.62%-14.08% for the palliative group (Figure 2D); adjusted OR range 1.47 South/Rural to 1.72 South/Urban), and hospitalizations (10.15%-10.78% vs 7.37%-8.18% who received palliative care (Figure 2C); adjusted OR range 1.49 North/Rural to 1.77 South/Urban) in the last 30 days of life. The largest difference was seen with increased ICU admissions in the last 30 days of life (12.31%-14.49% vs 4.12%-5.66% for those who received palliative care (Figure 2B); adjusted OR range 2.64 North/Rural to 4.36 North/Urban). Furthermore, these trends appeared stable over the time frame examined from 2007 to 2012.

Indicators of aggressive end-of-life care in northern and rural Ontario cancer patients with (solid line) or without (dashed line) a palliative designation between 2007 and 2012: (A) delivery of chemotherapy in the last 14 days, (B) admission to an intensive care unit in the last 30 days of life, (C) more than one hospitalization in the last 30 days of life, and (D) more than one visit to the emergency department (ED) in the last 30 days of life.
North/Rural cohort members received the highest percentages of potentially aggressive end-of-life care overall (Figure 3A) and were more likely to die in an acute care hospital than all other Ontarians (Figure 3B).

Aggressive end-of-life care and death in acute care between rural and urban residences within northern or southern Ontario from 2007 to 2012: (A) percentage of cancer patients who received any aggressive end-of-life care who had a northern or southern rural or urban residence. (B) Percentage of cancer patients who died in an acute care setting who had a rural or urban residence.
When individual indicators of potentially aggressive end-of-life care were examined, rural locations (irrespective of north or south location) had increased ED visits and hospitalizations in the last 30 days of life (Figure 4D and C). This pattern was not evident for the other individual indicators of receiving chemotherapy in the last 14 days of life or receiving intensive care in the last 30 days, with both northern and southern areas (either rural or urban) displaying similar percentages of care received (Figure 4A and B).

Indicators of aggressive end-of-life care between rural and urban residences located within either northern or southern Ontario. Percentage of cancer patients with a rural or urban residence in northern or southern Ontario who (A) received chemotherapy within the last 14 days of life, (B) were admitted to an intensive care unit within the last 30 days of life, (C) had more than one hospitalization in the last 30 days of life, and (D) had more than one emergency department visit in the last 30 days of life.
Discussion
Main findings of the study
The main findings in this study are that northern rural residents in Ontario were less likely to receive palliative care, more likely to receive some form of potentially aggressive end-of-life care, and similarly, more likely to die in an acute care hospital when compared with other Ontario residents. While the northern population represents about 6% of the population of Ontario, barriers to providing health care in this area are numerous and include geography, health care system eligibility criteria, limitations of the available workforce, palliative care educational deficits, as well as differences in cultural competencies.22,37 There is substantial variation and inequity of palliative care services across the province of Ontario, 38 although there is consensus around a recognized need for the development and implementation of a comprehensive palliative care strategy initiated earlier in the disease trajectory. 39 Combined with the strong overall association between palliative care and decreased use of potentially aggressive end-of-life care or death in an acute care hospital, our findings are in agreement with Jang et al. 6 and Cheung et al., 9 who also report these associations in a cohort of pancreatic cancer patients in an earlier (although overlapping) time period of Ontario decedent cancer cases. We expect that improving access to palliative care in this area could improve pain and symptom management and provide better patient and caregiver satisfaction and provide moderate relief on the use of potentially aggressive end-of-life care and potentially reduce hospital admissions and stays.40–43
While southern rural residents did not demonstrate decreased likelihood of palliative care, rurality itself is a substantial barrier to care. Rural residents in general demonstrated higher use of ED and hospitalizations, as well as death in acute care hospital. Rural residents, however, did not demonstrate higher use of chemotherapy or ICU admissions. Some authors report that cancer patients in rural areas of Ontario are less likely to have access to cancer care resources,17,44,45 which could contribute to rural residents being more likely to have aggressive end-of-life care.6,7 In addition, high use of ED and hospital resources by rural residents may have occurred as a result of resource access or availability in rural areas—where EDs are being used for situations that may be addressed within ambulatory settings in urban areas.46–48 Other independent risk factors associated with not receiving palliative care included being older, male, and residing in a lower income quintile area. These findings have been demonstrated previously by others using similar data sources, variable definitions, and overlapping time periods.6,45,49
Study strengths and limitations
Our study has advantages. Many of the data sources have been assessed as feasible, reliable, and valid for measuring end-of-life care in Ontario. 50 The retrospective cohort design is an important study type for assessing end-of-life care 51 and has allowed us to report population-based estimates. We adopted variable definitions that have been published by others using these administrative data sources,7,9 and the palliative care designation (defined as at least 2 palliative consultation codes occurring greater than 30 days apart within the last year of life) ensured that palliative care would have preceded end-of-life care.
Important limitations of our study include that the registration of cancer cases and determination of a cancer cause of death results in time delays, and therefore, our results may not reflect recent trends. Also, the administrative nature of the data does not allow us to assess the appropriateness or quality of the palliative care received. Furthermore, additional variables that could have helped to better define the cohort and the cancer treatment they received were not available for analyses. For example, cancer stage at diagnoses or cancer care activity level was not available for our analyses, and we are unable to characterize our data using these criteria.
Our study found that northern and rural residents of Ontario were less likely to have received palliative care and we suggest that improving access could also reduce the use of some inappropriate resources at the end of life. How to improve access in northern and rural areas remains an important issue, and while many recognize that care delivery may look different in the rural environment,16,18,52–54 and that transplanting urban models to rural settings may be problematic, 53 there are developed frameworks47,48 and evolving strategies such as telehealth, community-academic partnerships, and training for rural health professionals that can contribute to the provision of palliative care to all residents of Ontario.43,55–57
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/ or publication of this article: This study was funded by the Northern Cancer Foundation through a principal investigator grant awarded to M Conlon. This study made use of de-identified data from the ICES Data Repository, which is managed by the Institute for Clinical Evaluative Sciences with support from its funders and partners: Canada’s Strategy for Patient-Oriented Research (SPOR), the Ontario SPOR Support Unit, the Canadian Institutes of Health Research and the Government of Ontario. This study was supported through provision of data by the Institute for Clinical Evaluative Sciences and Cancer Care Ontario (CCO) and through funding support to ICES from an annual grant by the Ministry of Health and Long-Term Care (MOHLTC) and the Ontario Institute for Cancer Research (OICR). The opinions, results and conclusions reported in this paper are those of the authors. No endorsement by ICES or any of its funders or partners is intended or should be inferred.
Parts of this material are based on data and information compiled and provided by CIHI. However, the analyses, conclusions, opinions and statements expressed herein are those of the author, and not necessarily those of CIHI.
Parts of this material are based on data and information provided by Cancer Care Ontario (CCO). The opinions, results, view, and conclusions reported in this paper are those of the authors and do not necessarily reflect those of CCO. No endorsement by CCO is intended or should be inferred.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MC was involved in study design, statistical analysis, data interpretation, and execution of the study as well as drafting, editing, and manuscript revision. JC was involved in statistical analysis, data interpretation, and manuscript preparation. SS was involved in data interpretation, drafting, editing, and revisions of the manuscript. BB, MM, AK, CE, and MH were all involved in the execution of the study. All authors provided critical review of the final manuscript.
Ethics and Consent
The study was approved by the Research Ethics Board of Health Sciences North, project number 16-001, January 2016 to present.