
Abstract
Background:
In palliative care settings, collusion or “conspiracy of silence” frequently interferes with communication and interpersonal relationships among patients, caregivers, and healthcare professionals. The “Caregiver Collusion Questionnaire” is the only tool available for assessing caregiver collusion. The purpose of the study is to translate and adapt the English version of this instrument into Bengali, followed by standard validation.
Methods:
The study was carried out in two stages. Four independent translators conducted forward and backward translations of the English version of the “Caregiver Collusion Questionnaire” into Bengali. The Bengali version of the instrument was finalized following expert committee reviews, pre-testing, and cognitive debriefing. The final validation was carried out among 71 caregivers of patients with advanced incurable illnesses admitted to the palliative medicine and internal medicine departments of two Bangladeshi hospitals. In the final phase, the validity (content, face, and construct validity) and reliability (interclass item-wise correlation coefficient) of the translated tool were assessed.
Result:
60% of the participants fully understood 19 items, whereas 40% struggled with one or more items. The expert committee expressed their satisfaction with the face and content validity of the translated version. The Bengali version also had quite good reliability (α = 0.62). Seven components were identified using principal component analysis with the distribution of Varimax Rotation distribution. Items under each factor had adequate factor loading, ranging from 0.4 to 0.8.
Conclusion:
The Bengali version of the “Caregiver Collusion Questionnaire” was found valid reliable and culturally acceptable for measuring caregiver collusion among the Bengali-speaking people. Based on the scale, the reasons for collusion can be identified and measures can be taken for breaking the collusion.
Keywords
Introduction
Collusion is an unconscious interaction between patients, family members, and healthcare professionals. It involves concealing crucial information from the patient, such as the diagnosis, prognosis, or specific medical facts, by someone close to him or her. It can lead to intense feelings, unreflective actions, and a detrimental effect on patient treatment.1,2 Twycross described collusion as a “conspiracy of silence” or “source of tension” that blocks conversation about the future and interferes with interpersonal relationships and communication. 3 In the context of palliative care, where interpersonal relationships are crucial, collusion holds significant importance.
When a patient is diagnosed with an incurable illness, relatives often try to keep the diagnosis and prognosis hidden from the patient. They also try to include healthcare providers in this process. 4 Family psychodynamics are affected by the diagnosis of an incurable illness, either positively or negatively. The majority of families deal with the ongoing tension between the impulse to protect their loved ones from the emotional distress caused by reality and the desire to reveal the truth. 5 Patients diagnosed with terminal illnesses usually want to know their diagnosis but caregivers are not interested in disclosing the truth. 6
According to majority of the healthcare providers, a diagnosis should be revealed to patients suffering from life-threatening illnesses.7,8 An Iranian study found that it is better to disclose the diagnosis and prognosis to the person suffering from the incurable illness. 9 In India, almost 50% of patients with cancer are unaware of their diagnosis and treatment. Even doctors often feel comfortable to reveal the diagnosis to the family rather than to the patients. Sometimes, they succumb to the extreme pressure of their relatives. 7
Communication is an important component of palliative care and management of collusion is a challenging aspect of communication. Collusion has several bad effects: poor doctor–patient relationship, poor symptom management as well as the development of mistrust causing sour relationships with relatives. On the other hand, honest and open communication with patients and relatives is often beneficial for both parties. 9
Although it is difficult to detect collusion due to the way collusion is expressed, the tools for collusion are scarce and lack theoretical strength. As a result, collusion among the caregivers of a terminally ill patient is not fully evaluated or understood properly. For effective communication and patient management, it is very important to measure the caregiver’s collusion about the diagnosis. 5
There is only one questionnaire available for measuring caregiver collusion which is the “Caregiver Collusion Questionnaire” which was developed by the Indian Institute of Technology, Hyderabad, India. It detects and measures collusion among caregivers using 20 items, where possible scores range from the presence of no collusion to high collusion. 5
Collusion prevails among one-third of the caregivers of patients with terminal illnesses. 7 There is no established evaluation instrument for the assessment of collusion among Bengali-speaking people. So palliative care providers in Bengali-speaking areas often face problems establishing proper communication with them and encounter difficulty while managing the patients. So, the study aims to translate the English version of the “Caregiver Collusion Questionnaire” into Bengali and then validate it according to standard procedure.
Methods
Caregiver Collusion Questionnaire
James, 2014, developed this scale to assess the level of collusion among patients’ caregivers who are terminally ill. It evaluates the caregivers’ intent to withhold or partially disclose the disease’s diagnosis or prognosis from the patients, attempts to conceal the information, worries about the patient’s mental state after learning of the condition, disruptions to their regular routines, and interpersonal interactions with both the patient and others. There are a total of 20 items. Each item is answered with “yes” or “no” responses. All positive answers are scored as “1” and negative answers are scored as “0,” except items 4, 7, 9, 10, 13, 19, and 20. These items are reversely scored. The highest possible score is “20” and the lowest possible score is “0.” Higher scores represent a higher level of collusion. The measure can be adjusted to evaluate collusion in different contexts. 5
Translation procedure
The translation from English to Bengali was carried out in accordance with the rules given by Beaton et al. 10 Two different translators who spoke Bengali carried out the forward translation; one was knowledgeable about the concept of the scale (T1), while the other was not (T2). While both translators had medical backgrounds, T2 also specialized in English literature. A third, unbiased person then integrated the two versions to create a combined one (Ts). The Ts version of the questionnaire was back-translated into English by two independent translators (BT1 and BT2), one with a background in medicine and the other not. Both had an excellent grasp of the English language. To avoid information bias, these two back translators were kept uninformed about the tool’s concept. An expert committee consisting of three palliative medicine specialists, an internist, and a psychiatrist was formed. The expert committee assessed and compared all translations and the original scale. After reaching a consensus among all committee members, the final Bengali version was prepared for pilot testing (Table 1).
Translation procedure of Bengali version of Caregiver Collusion Questionnaire.

Cognitive debriefing
In all, 10 caregivers of terminally ill patients participated in cognitive debriefing at the Internal Medicine Department of Sher-E-Bangla Medical College Hospital (SBMCH), Barisal. The objective of the study was explained to each participant, and they were all questioned before and after completing the questionnaire to check for any difficult, perplexing, or unpleasant words. The researchers tried a number of different wordings and explanations for the difficult or perplexing terms until they found adequate replacements. Information on these participants was just used for this procedure and not in the main research. The expert group then reviewed and approved the final version of the updated questionnaire, and decided that no further pilot testing was necessary.
Setting and participants for the final validation phase
The cross-sectional study was conducted at Sher-E-Bangla Medical College Hospital, Barishal, and Bangladesh Cancer Society and Welfare Home in the department of internal medicine and palliative care unit. The caregivers of the patients with advanced incurable diseases (e.g., cancer, end-stage heart failure, end-stage liver failure), age ⩾18 years, who could understand Bengali were considered illegible for this final validation stage. The caregivers with suspected collusion were asked two screening questions: “Does your patient know about his or her diagnosis or prognosis” and “Do you want to reveal the diagnosis or prognosis to your patient.” Those who answered negatively to both questions were included in the study. Occasional caregivers (caregiving days ⩽5 days/week) were excluded.
A surprisingly high proportion (almost one-sixth) reported factor analysis based on sample-to-item ratios of only 2:1 or more.11,12 Also, to detect a sizable level of interclass item-wise correlation coefficient, the minimum sample size requirement is 60–63. 13 Although the prevalence of collusion among caregivers of patients with cancer is 37% in the literature, in our practical experience, most of the adult patients had already known or guessed their diagnosis and/or prognosis with the advancement of the disease. So, collusion at the advanced stage is not very common, especially in palliative care settings. 7 Initially, we considered a sample-to-item ratio of 5:1 to calculate the minimum sample size. As the total item number is 20, a total of 100 samples were considered. We approached 105 caregivers with collusion within our study period but only 71 of them were able to complete the whole questionnaire. Five of them skipped items 5, 8, and 19 because they felt uncomfortable, and the rest of them gave up in the middle due to sensitive questions (non-response rate: 32.4%). So, our final sample size was 71 (sample-to-item ratio 3.5:1).
Data collection
The period of data collection was June to September 2023. A consecutive sampling technique was used to collect the samples. Eligible caregivers were asked to fill out the questionnaire on their own. For those who were unable to read or write, one of the investigators read the questions aloud for them word by word without any alteration and filled up the questionnaire for them based on their verbal responses. The lead investigator provided the participants with brief explanations of each item as needed to clarify any confusion. Every questionnaire took 5–10 min to complete.
Statistical analysis
Face validity was evaluated in the course of the standard translation procedure. The content validity was also evaluated during translation, back translation, and expert committee review. Factor analysis with Principal Component Analysis with Varimax Rotation was used to evaluate the construct validity. Items loading <0.30 was rejected. Cronbach’s alpha (interclass item-wise correlation coefficient) was used to assess reliability, with a cutoff point of ⩾0.50. Sociodemographic variables (age, sex, educational status, relationship with the patient) were expressed in frequency and percentage. The continuous variable (age) was also expressed in mean ± SD. The statistical package for social science, IBM Inc., version 26, was used to analyze the data.
Ethical considerations
Ethical approval for both the research and consent procedure (Approval no: CeNoR/EA/2301; Date: 07/05/2023) was obtained from the Ethical Review Committee, Center for Noncommunicable Diseases Prevention Control Rehabilitation and Research. Before taking part in this study, all eligible individuals were asked to provide written and/or verbal informed consent. For those who could not read or write, the consent paper was read out to them word by word without any alteration, and a thumbprint of the right hand was taken in the consent paper after obtaining their verbal consent. All information was kept anonymous. No information or images used in this study led to the identification of the study participants.
Results
Validity analysis
Linguistic validation: Face validation and clinical review were included in the translation and adaptation procedure. The expert committee members agreed that the test’s objective was clear and that it should assess collusion among caregivers of patients with terminal conditions. During cognitive debriefing, 60% of the participants fully understood 19 items, whereas 40% had trouble comprehending one or more items. Regarding item no. 1, the participants could not understand the synonyms used for “stressful condition.” So, we opted for the explanation rather than using the word-for-word translation. Regarding items 2 and 3, we used the word “worry” rather than “anxiety.” Items 1, 5, 6, and 9 needed a brief explanation, as they were too lengthy.
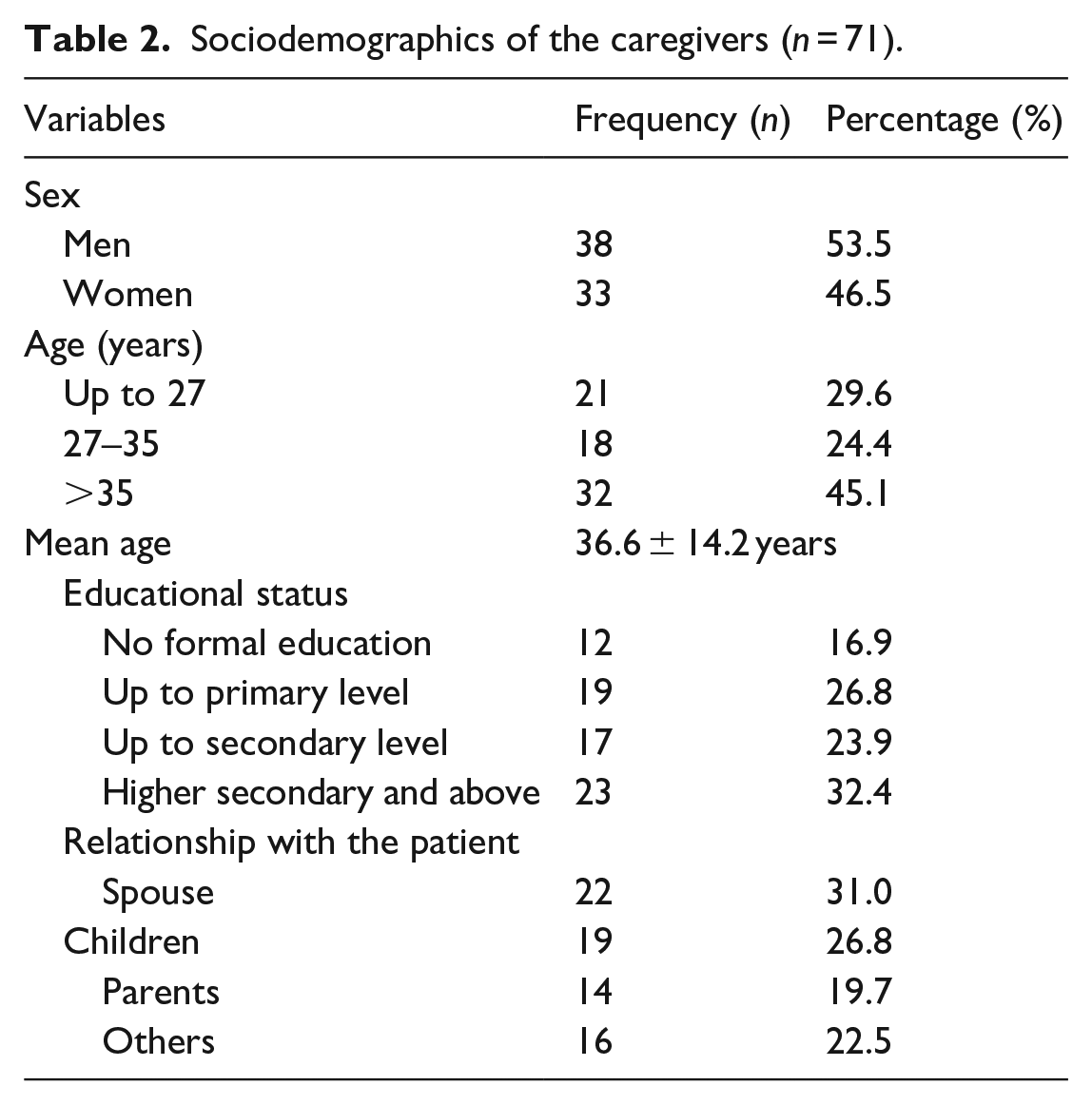
Construct validity: The final validation procedure included a roughly equal number of participants from both sexes (38 men and 33 women), with a mean age of 36.6 ± 14.2 years. Their educational status ranged from no formal education (16.9%) to higher secondary level or above (32.4%) (Table 2). Exploratory factor analysis with principal component and Varimax rotation was used to test the construct validity of the final version. The observed Kaiser-Meyer-Olkin value of 0.6 indicates that the current data were sufficient for factor analysis. Bartlett’s sphericity test (2 = 393.28, df = 190, p = 0.001) demonstrated that the sample was appropriate for factor analysis. 14 Based on eigenvalues, a seven-component structure was found in the Bengali version. Items 4, 5, 8, 12, 13, and 17 were loaded into component 1. Item 3 is loaded in Component 2. Items 6 and 14 were loaded in component 4. Item 7 was loaded in Component 5. Items 1 and 19 were loaded in component 6. And item 2 was loaded in Component 7. Items under each factor had adequate factor loading, ranging from 0.4 to 0.8 (Table 3).
Sociodemographics of the caregivers (n = 71).
Principal component analysis with the distribution of Varimax rotation.

Extraction method: principal component analysis; Rotation method: Varimax with Kaiser normalization.
Reliability analysis
A Cronbach’s alpha (interclass item-wise correlation coefficient) score of 0.4 or higher is regarded as quite reliable. The “Caregiver Collusion Scale—Bengali” had a Cronbach’s alpha score of 0.62 and a score based on standardized items of 0.61.
Discussion
An essential step in adapting an instrument to a new culture is translation. Sometimes, it is very difficult and a great challenge for the translator to find appropriate words in the translated language. We translated and validated the “Caregiver Collusion Questionnaire” in this study, which is the only tool available for assessing collusion in palliative care.
During the construction of the original scale, reliability was assessed by administering the instrument to 30 caregivers (20 females and 10 males) ranging in age from 18 to 60 years. Using “The Rational Equivalency Method” by “Kuder Richardson,” the internal consistency of the original scale was calculated at 0.74.5,15 The Cronbach’s alpha (α) score of the Bengali version of the scale was 0.62, which is considered quite reliable.
We also assessed the face validity and construct validity of the translated instrument which was also assessed in the original instrument. 5 Face validity was assessed during linguistic validation. It was assessed by the expert committee members during the review process. They also concluded that this instrument is capable of measuring the collusion among caregivers of patients with life-limiting conditions.
During cognitive debriefing, some changes were made because, out of 10 participants, 40% had difficulty understanding one or two items. Regarding item 1, there is difficulty in understanding the synonyms used for “stressful condition.” We explained the phase by using “previous disease or any other worrisome condition.” We also decided on the explanatory translation for the word “anxiety” in items 2 and 3, and replaced them with the word “worry.” As the word “anxiety” is often synonymous with “restlessness,” which is not appropriate to the context of this question, we went for contextual translation. Items 1, 5, 6, and 9 needed a brief explanation as they were too lengthy. Some of the caregivers also admitted that they never thought about these contexts consciously before, although they were using them regularly while handling their patients.
After cognitive debriefing, a revised version was prepared. The final version of the instrument was accepted as accurate by the expert committee for assessing collusion among the Bengali-speaking group. There was no need for a second validation group to test the revised version.
A seven-component structure was found in the Bengali version, which was not previously explored during the construction of the original scale. 5 Six items were loaded into Component 1, which mainly measures the caregiver’s concerns about the patient’s mental condition regarding knowing the truth. Item 3 is loaded in Component 2, which measures the caregiver’s anxiety regarding the patient’s ability to accept the truth. Items 6 and 14 are loaded in Component 4, which indicates the caregiver’s fear of revealing the truth. Item 7 is loaded in Component 5, which measures the effect of collusion on the caregiver’s daily routine. Items 1 and 19 are loaded in Component 6, which indicates the caregiver’s anxiety and view of their patient’s independence in choosing end-of-life care. Finally, Item 2 is loaded in Component 7, which measures the caregiver’s view of the patient’s behavioral pattern. Items under each factor had adequate factor loading. During the formation of the original scale, no such test was done to determine the component. 5
One limitation of the study was that the convergent validity of this tool could not be assessed, as there is no other tool in Bengali to assess collusion among caregivers of patients with terminal diseases. This tool is not translated into any other languages, so we could not compare reliability with other versions. Another limitation was that we had a fairly small sample size. As mentioned earlier, most of the patients as well as their caregivers either guessed or were informed about the diagnosis and prognosis at the advanced stage, so we could not find our intended sample size within the period of the study. Also, we could not perform the test–retest reliability because caregivers were not comfortable with repeating some of the sensitive questions. They were often distressed about the conditions of their patients too. So, only limited aspects of validity and reliability could be assessed.
Conclusion
The Bengali version of the “Caregiver Collusion Questionnaire” was found valid reliable and culturally acceptable for measuring caregiver collusion among the Bengali-speaking people. Based on the scale, the reasons for collusion can be identified and measures can be taken for breaking the collusion. Proper communication about collusion will aid in the improvement of interpersonal relationships between caregivers, patients, and healthcare professionals, potentially increasing the quality of life for both patients and their families.
Footnotes
Acknowledgements
The authors would like to express their gratitude to Tajib Adnan Chowdhury for his assistance in translating the Bengali version of the Caregiver Collusion Scale.
Author contributions
Jheelam Biswas: Conceptualization, data curation, methodology, formal analysis, funding acquisition, investigation, methodology, project administration, resources and software, validation, writing original draft, editing, and review. Nahid Afsar: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources and software, validation, writing original draft, editing, and review. Salma Ahsan Khanam: Conceptualization, data curation, investigation, project administration, editing, and review. Shima Rani Sarker: Conceptualization, data curation, investigation, project administration, editing, and review. Shamsudduha Tauhid: Conceptualization, data curation, investigation, project administration, editing, and review. Nashid Islam: Conceptualization, data curation, investigation, project administration, editing, and review.
Data sharing statement
All data relevant to the study are accessible in Mendely data doi: 10.17632/8pw5t5cy8d.1.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This study was performed following the Declaration of Helsinki, and no invasive procedures were involved.
Trial registration
Not applicable.