
Abstract
The clinical benefit of adding platinum to adjuvant chemotherapy for patients with triple-negative breast cancer (TNBC) has not been well investigated, although it was associated an improved response rate in neoadjuvant setting. We retrospectively analyzed the time to tumor progression (TTP) and overall survival (OS) of patients with resected stage I-III TNBC who were treated with or without cisplatin-containing chemotherapy (CisCT or noCisCT) during 2004 and 2010. Of 129 patients, 25 received CisCT. In univariate analysis, the mean TTP for CisCT and noCisCT was 4.42 and 5.88 years, respectively (P = .004). The mean OS for CisCT and noCisCT was 6.76 and 9.63 years, respectively (P = .24). After adjusting for other clinicopathologic factors, only clinical stage II/III disease was independently associated with worse OS. The adjusted hazard ratio for CisCT was 1.48 (P = .46) and was not statistically significant. In this small retrospective study, adding cisplatin to adjuvant chemotherapy for early TNBC with unknown BRCA mutation status did not benefit OS.
Introduction
Triple-negative breast cancer (TNBC) is characterized by the lack of expression of estrogen receptors (ER), progesterone receptors (PR), and human epidermal growth factor receptor 2 (HER2) and comprises approximately 15% of all breast cancers.1,2 When compared with non-TNBC, patients with resected early-stage TNBC have a higher incidence of recurrence within 3 years after surgery and a higher risk of distant metastasis with an increased likelihood of metastasis to visceral organs rather than to bone.2–6 Once metastases develop, the median time from relapse to death is often shorter than that of other subtypes of breast cancer. 7 Therefore, adjuvant chemotherapy for resected early-stage TNBC (stage I-III) is considered for tumors larger than 0.5 cm or node-positive disease.8,9 However, there is no specific chemotherapeutic regimen specifically recommended for patients with these disease subtypes. 7
The molecular signature of TNBC generally overlaps with that of basal-like (BL) breast cancer, which is approximately 80% concordant with TNBC based on immunohistochemistry. 10 Preclinical models of breast cancer indicated that BL1 and BL2 cell line subtypes, which have higher expression of cell cycle and DNA damage response genes, were sensitive to cisplatin. 11 Recently, the addition of platinum to neoadjuvant chemotherapy for women with TNBC has been shown to improve rate of pathologic complete response (pCR) in several clinical trials. 12 Although pCR is a valuable surrogate end point for prognosis, 13 none of these trials published longer-term outcomes, such as progression-free survival or overall survival (OS). The clinical benefit of incorporating platinum into adjuvant chemotherapy has not been well investigated. In this study, we retrospectively reviewed the use of cisplatin in the adjuvant setting for early breast cancer and compared the survival outcome with other cisplatin-naïve chemotherapy.
Materials and Methods
Patient characteristics
A total of 2647 patients were diagnosed with invasive breast cancer at Mackay Memorial Hospital, Taipei, Taiwan, between January 2004 and December 2010. A total of 221 patients of these patients (8.3%) were diagnosed with TNBC and were recruited to this study. The diagnosis of TNBC was defined as immunohistochemically ER-negative, PR-negative, and HER2-negative disease. Hormone receptor negativity was defined by less than 1% staining of tumor cells using immunohistochemistry (IHC). 14 HER2-negativity was defined by an IHC score of 0 to 1+ or as no amplification following fluorescent in situ hybridization. Patients who had double or multiple cancers at diagnosis (n = 9), de novo metastatic disease at diagnosis (n = 3), insufficient information at diagnosis (n = 3), were lost to follow-up (n = 23), had received neoadjuvant chemotherapy (n = 27), had received no adjuvant chemotherapy (n = 20), or who did not complete the planned chemotherapy (n = 7) were excluded. Among the 7 patients who were medically unfit for adjuvant chemotherapy, 1 stopped chemotherapy because of hepatitis flares and 1 because of uncontrolled underlying psychiatric disease. Therefore, 129 patients were included for analysis.
TNM (tumor-node-metastasis) staging was evaluated based on the TNM Classification of Malignant Tumors, UICC Seventh Edition. 15 Histopathologic differentiation and clinical information, including demographic data, date of surgery, TNM stage, chemotherapy regimen, time to initiation of chemotherapy following surgery, time to tumor progression (TTP), and OS were collected from the medical charts. Time to tumor progression was defined as the time from surgery to the first documented progression identified using imaging studies. Overall survival was defined as from the time of surgery to the last follow-up or time of death. Breast cancer–specific survival was determined from the time of surgery until death from breast cancer. All patients were monitored until death or January 23, 2015. The median follow-up period was 5.9 years. About 73% of the 129 patients were followed over 4 years. The study was approved by the Ethics Committee of Mackay Memorial Hospital (approval number: 15MMHIS192e).
Statistical analysis
Statistical analysis was performed to determine the association of exposure to platinum in adjuvant chemotherapy with TTP and OS. Categorical data were reported as numbers and percentages. Continuous data were reported as medians and ranges. Their means were compared using the Student t test. Categorical variables were compared using the χ2 or Fisher exact test. Both TTP and OS were estimated using Kaplan-Meier survival analysis and compared using the log rank test. Univariate analysis was used to test the association between treatment subgroup or tumor characteristics and survival time. Significant associations were further tested in the multivariate analysis using Cox proportional hazards model adjusted for known prognostic covariates, including age, tumor/nodal status, stage, and adjuvant treatment. All statistical tests were 2-sided, and significance was defined as a P value of <.05.
Results
Patient demographics
The characteristics of the 129 patients with early TNBC who received surgery and adjuvant chemotherapy are listed in Table 1. Of 129 patients (76%), 98 underwent total mastectomy and 31 (24%) underwent breast conservative surgery and adjuvant radiotherapy. In all, 40 patients (31%) were aged more than 60 years. Most patients had stage I and II disease (n = 115, 89.1%). In all, 25 patients (19.4%) received cisplatin-containing adjuvant chemotherapy (CisCT). The dose ranges of chemotherapeutic agents used in the study are listed in Table 1. The clinical characteristics of patients treated with a cisplatin-containing regimen versus those treated with a no cisplatin regimen (noCisCT) are listed in Table 2. In the CisCT group, there were more patients with stage II/III disease (80%) than in the noCisCT group (59%), although this did not reach statistical significance (P = .07 using Fisher exact test). There was no statistically significant difference between the 2 groups in average age, follow-up times, time to initiation of chemotherapy, and number of chemotherapy cycles received. Although not significant, there appeared to be a high number (9.6%) of non-IDC (infiltrating ductal carcinoma) in the NoCisCT group compared with 0% in the CisCT group. Among the 10 patients with non-IDC histology, 4 patients had medullary carcinoma, 1 had metaplastic carcinoma, 1 had papillary carcinoma, 1 had adenoid cystic carcinoma, 1 had background with apocrine ductal carcinoma in situ, and 2 had squamous cell carcinoma.
Patients’ characteristics (n = 129).
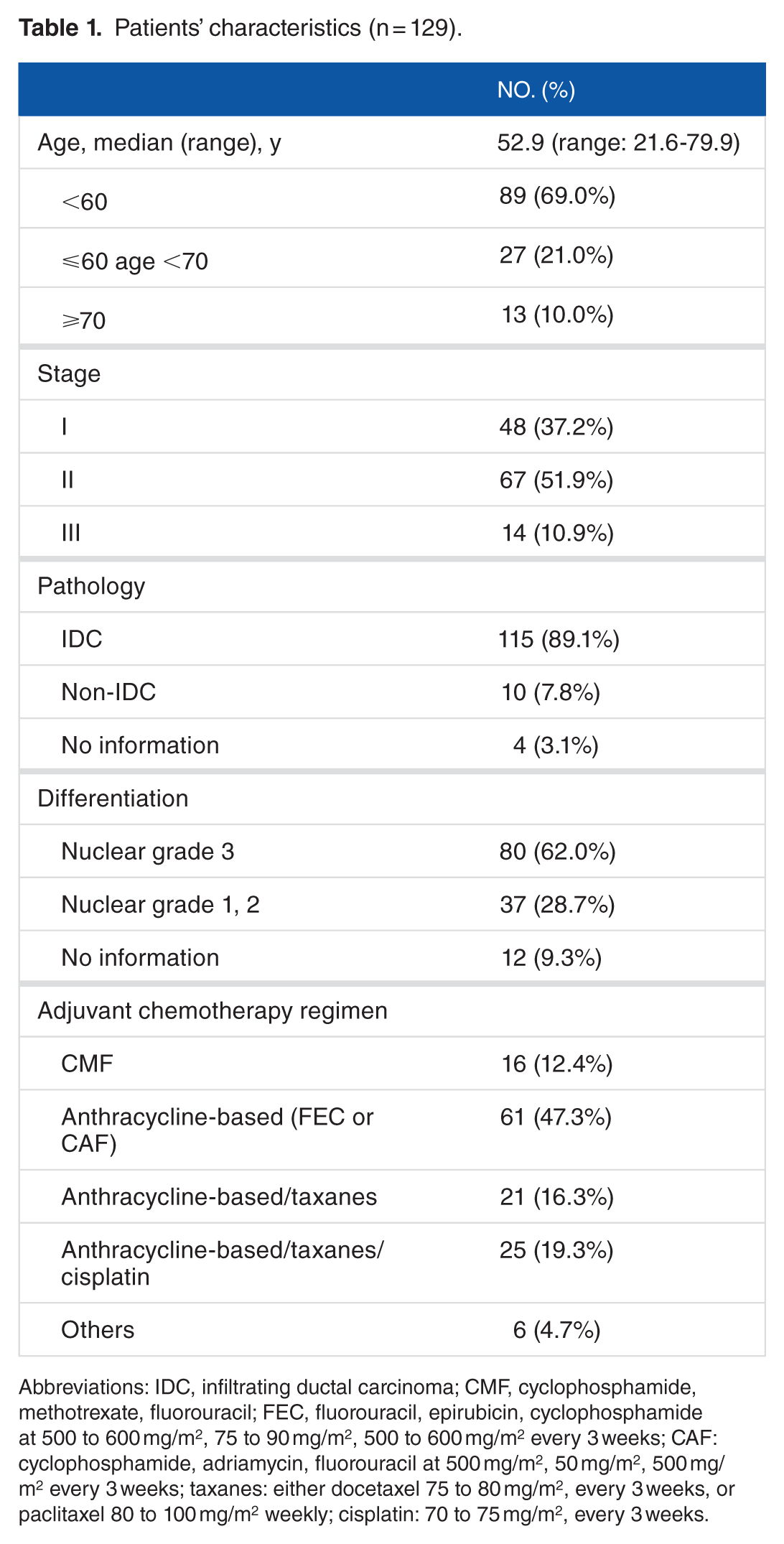
Abbreviations: IDC, infiltrating ductal carcinoma; CMF, cyclophosphamide, methotrexate, fluorouracil; FEC, fluorouracil, epirubicin, cyclophosphamide at 500 to 600 mg/m2, 75 to 90 mg/m2, 500 to 600 mg/m2 every 3 weeks; CAF: cyclophosphamide, adriamycin, fluorouracil at 500 mg/m2, 50 mg/m2, 500 mg/m2 every 3 weeks; taxanes: either docetaxel 75 to 80 mg/m2, every 3 weeks, or paclitaxel 80 to 100 mg/m2 weekly; cisplatin: 70 to 75 mg/m2, every 3 weeks.
Characteristics of patients receiving cisplatin-containing adjuvant treatment (CisCT) versus no cisplatin adjuvant chemotherapy (noCisCT).
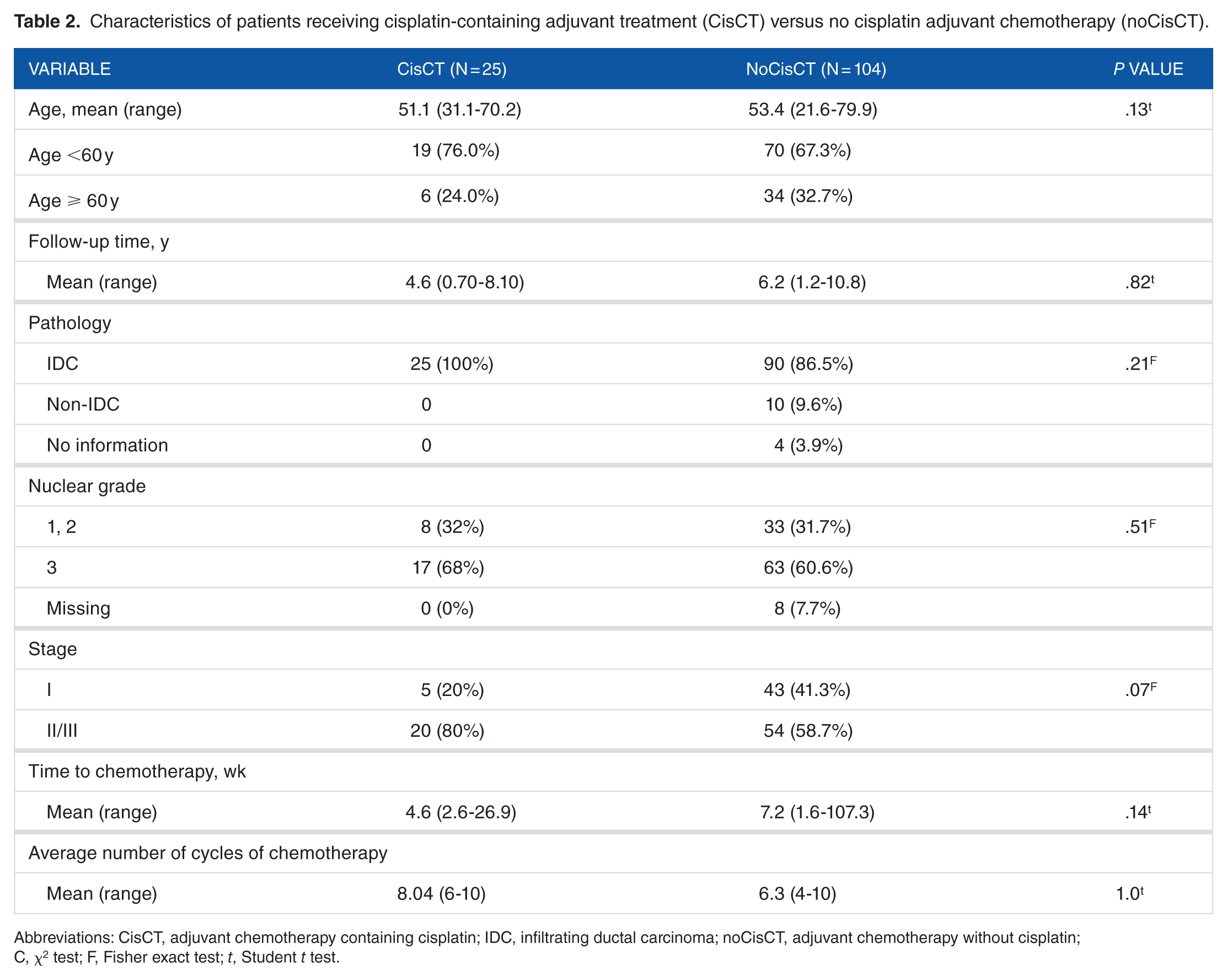
Abbreviations: CisCT, adjuvant chemotherapy containing cisplatin; IDC, infiltrating ductal carcinoma; noCisCT, adjuvant chemotherapy without cisplatin; C, χ2 test; F, Fisher exact test; t, Student t test.
Association of chemotherapy regimen and other clinicopathologic factors with survival
Kaplan-Meier survival curves (TTP and OS) for the CisCT and noCisCT groups are shown in Figure 1. The mean TTP in the noCisCT group was 5.88 years (SE: 0.28, 95% confidence interval [CI]: 5.33-6.44), which was significantly longer than that in the CisCT group (mean: 4.42 years, SE: 0.50, 95% CI: 3.44-5.39, P = .004 using a log rank test). The mean TTP for patients with stage I disease was also significantly longer than that for patients with stage II/III disease (6.22 years, SE: 0.45 years, 95% CI: 5.33-7.11 versus 5.24 years, SE: 0.30, 95% CI: 4.66-5.82, P = .013 using a log rank test). The mean OS was 9.63 years (SE: 0.29 years, 95% CI: 9.06-10.20) for the noCisCT group and 6.76 years (SE: 0.57, 95% CI: 5.64-7.87) for the CisCT group. There was no statistical significance according to a log rank test (P = .24). The survival times for patients with stage I and II/III disease were 9.95 (SE: 0.39) and 8.54 (SE: 0.35) years, respectively, and there was no significant difference between the 2 groups (P = .11; log rank test).

Kaplan-Meier survival curves ([A]: TTP; [B]: OS) for patients with stage I-III TNBC treated with adjuvant chemotherapy with a cisplatin-containing regimen (CisCT) and no cisplatin-containing regimen (noCisCT) (patient groups compared using the log rank test [L]).
Univariate analysis for other clinicopathologic factors, such as age older than 60 years, nuclear grade 3, and time to initiation of adjuvant chemotherapy showed no statistically significant correlation with either TTP (Table 3) or OS (Table 4).
Univariate analysis of clinical characteristics and time to tumor progression (TTP).

Abbreviations: CisCT, adjuvant chemotherapy containing cisplatin; noCisCT, adjuvant chemotherapy without cisplatin; OS, overall survival; SE, standard error.
P < .05.
Univariate analysis of clinical characteristics and OS time.
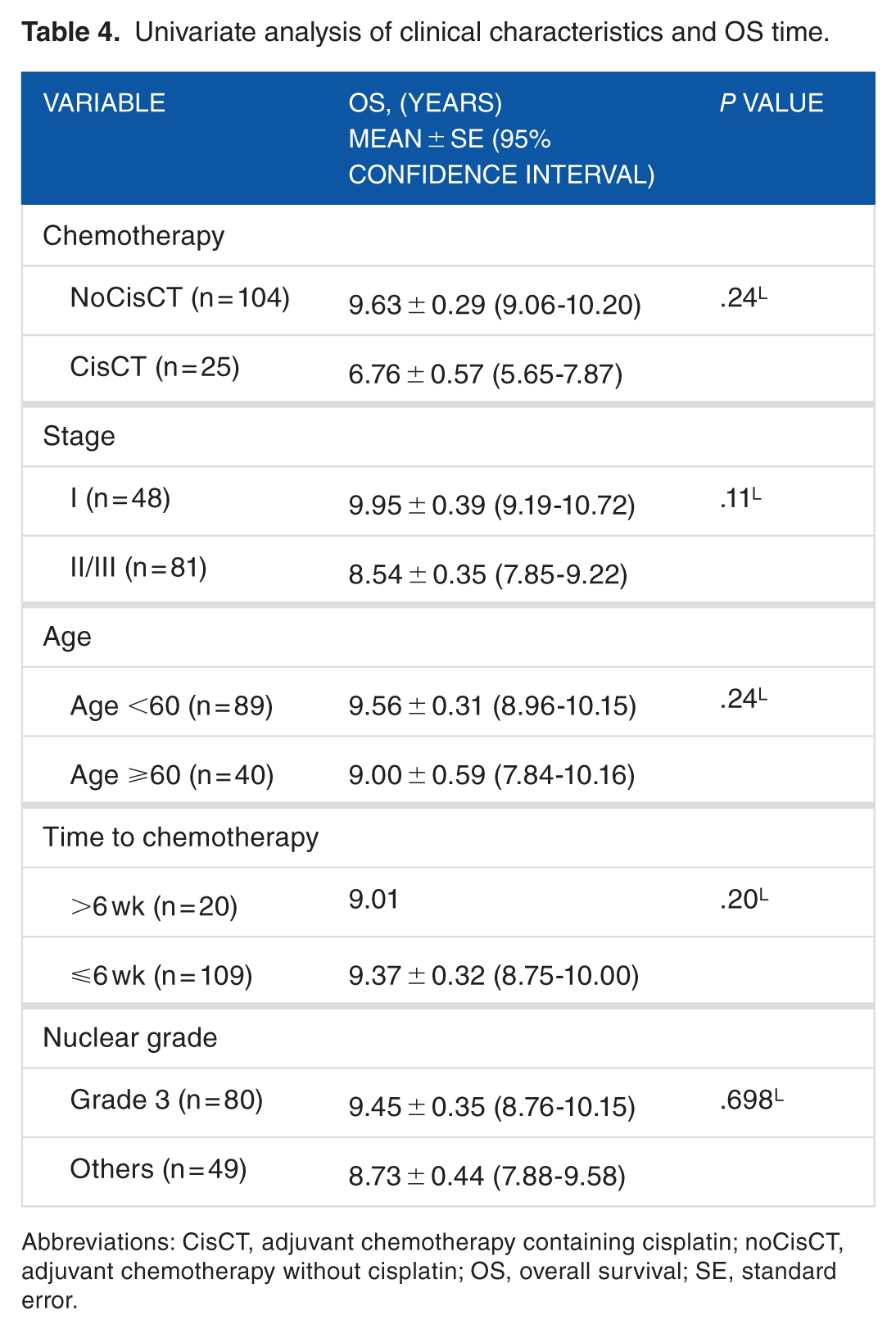
Abbreviations: CisCT, adjuvant chemotherapy containing cisplatin; noCisCT, adjuvant chemotherapy without cisplatin; OS, overall survival; SE, standard error.
Multivariate analysis using Cox proportional hazards models was performed to determine the prognostic significance of the clinicopathologic variables, which were age ⩾60 years, advanced (stage II/III) tumor stage, >6 weeks to initiation of chemotherapy, nuclear grade 3, and adjuvant chemotherapy containing cisplatin (CisCT), on TTP (Table 5) and OS (Table 6). After adjusting for these covariates, only clinical stage II/III disease was independently associated with worse OS, with an adjusted hazard ratio [HR] of 3.61 (95% CI: 1.02-12.79; P = .047). The HR of CisCT was 1.01 (95% CI: 0.64-1.60; P = .95) for TTP and 1.48 (95% CI: 0.52-4.18; P = .46) for OS, and no statistical significance was observed.
Multivariate analysis of TTP.
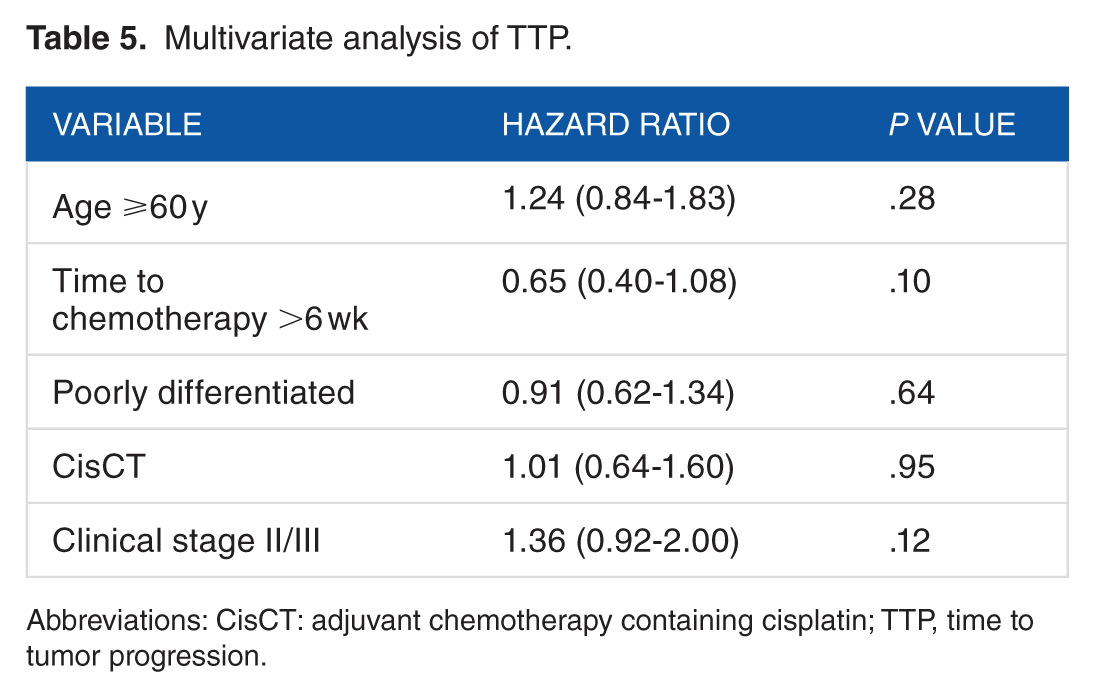
Abbreviations: CisCT: adjuvant chemotherapy containing cisplatin; TTP, time to tumor progression.
Multivariate analysis of OS.

Abbreviations: CisCT, adjuvant chemotherapy containing cisplatin; OS, overall survival.
P < .05.
Discussion
Triple-negative breast cancer generally has a poorer clinical outcome. Recently, adding platinum to neoadjuvant chemotherapy was associated with an improved response rate but its clinical benefit in adjuvant chemotherapy has not been well investigated. We retrospectively analyzed the survival of patients with resected early TNBC who were treated with or without cisplatin-containing chemotherapy. In this small, single institution experience, no survival benefit was achieved by adding cisplatin to the current standard adjuvant chemotherapy regimen in unselected patients TNBC.
In past decades, anthracycline/taxane-based systemic therapy has formed the backbone of the treatment for patients with TNBC,16,17 and there has been no substantial progress to date. Because chemotherapy is the only systemic option to prevent relapse, and patients with TNBC are usually at high risk of early relapse and poorer clinical outcomes, there is a clinical need to improve the current chemotherapy regimen in this subgroup of patients.
The use of platinum salts, such as cisplatin or carboplatin, in the treatment of early breast cancer did not receive much attention until 2010 when an increased response rate was observed by adding platinum to neoadjuvant chemotherapy. 18 A small study using single-agent cisplatin in neoadjuvant chemotherapy for TNBC was reported to achieve a pCR in 6 out of 28 patients (22%). 19 An increased pCR with the addition of another platinum drug, carboplatin, was also observed in 2 randomized phase 2 and 1 randomized phase 3 clinical trials in patients with stage II-III TNBC. In the GeparSixto trial, 12 the pCR rate increased from 36.9% without carboplatin to 53.2% with carboplatin; in the CALGB 40603 trial, 20 the pCR rate increased from 41% without carboplatin to 54% with carboplatin, and in the BrighTNess trial, 21 the pCR rate increased from 31% without carboplatin to 58% with carboplatin. However, in addition to the clinical benefit, these trials also showed a high incidence of adverse events and an increased discontinuation rate. While awaiting for the outcome of BrighTNess trial, the early survival analyses of GeparSixto and CALGB 40603 were reported simultaneously at the San Antonio Breast Cancer Symposium in December 2015. 22 In the GeparSixto study, the improved pCR rate translated into a significant increase in 3-year disease-free survival from 76.1% to 85.8% (HR: 0.56; 95% CI: 0.33-0.96; P = .035); however, in the CALGB 40603 study, no statistical difference in either 3-year event-free survival or OS was reported. The discrepancy of the results, although not well established, may partly reflect the different synergies between carboplatin and other chemotherapeutic agents, as well as a heterogeneous response to carboplatin because of tumor heterogeneity.
With increasing understanding of the molecular subtype of TNBC, tumors harboring BL gene signatures, BRCA1/2 mutation or “BRCAness” may have a better response to platinum treatment.18,19,23 However, BRCA1 mutation carriers (germline or somatic) comprise only 10% to 25% of patients with TNBC.24,25 The heterogeneity of TNBC suggests that a variable response could be expected if platinum salts were used in unselected patients.
To date, it is unclear whether there is a clinical benefit of adding platinum salts in the adjuvant setting.26,27 An ongoing randomized phase 3 clinical trial (EA 1131, NCT 02445391) is designed to look at the efficacy of adjuvant cisplatin or carboplatin on patients with residual triple-negative BL breast cancer following neoadjuvant chemotherapy. In our retrospective analysis, the average OS for early TNBC with CisCT was inferior to that of noCisCT and the HR was 1.29 in patients treated with CisCT. Although the results were not statistically significant, our experience did not support the routine use of cisplatin in patients with early TNBC who undergo resection.
Our study is limited by its small sample size, retrospective nature, and patient treatment selection bias. The study to evaluate the role of CisCT in adjuvant setting for resected TNBC was not powered to show statistically significant OS benefit.
In conclusion, investigations to identify biomarkers for platinum-sensitive subgroups, 26 as well as research to identify whether adjuvant cisplatin administration will benefit patients with stage II/III breast cancer and BRCA mutations are ongoing. 26 However, clinical evidence to support benefit from adding platinum salts to current standard adjuvant is weak and should not be recommended until a sufficiently powered prospective trial proves otherwise.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Mackay Memorial Hospital grant MMH-105-71 and MMH-CT-105-08.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Su YW and Yang PS contributed to the conception and design of the work; Su YW drafted the manuscript; Su YW and Hung CY collected and analyzed the data; Lam HB and Chang YC helped to draft the manuscript; all authors read and approved the final manuscript.