
Abstract
Background:
Abiraterone acetate is an androgen synthesis inhibitor approved for the treatment of castration-resistant prostate cancer (CRPC). Although co-administration of either prednisone or prednisolone at 10 mg/d has been recommended to reduce the risk of abiraterone-induced hyperaldosteronism (notably hypokalemia) and to give adjunctive pain relief effects, whether these glucocorticoids can be substituted by dexamethasone remains unknown.
Methods:
We performed a retrospective review of medical records of patients who were given abiraterone for the treatment of CRPC with either prednisolone (ABI/PSL) 10 mg/d or dexamethasone (ABI/DEX) 0.5 or 1 mg/d between 2014 and 2017 in Juntendo University Nerima Hospital. Demographic and biochemical data including prostate-specific antigen (PSA) level were retrieved from the electronic medical records.
Results:
Fifty-three eligible patients (27 in ABI/PSL group and 26 in ABI/DEX group) were extracted from the records. Both groups showed no significant changes in serum potassium level before and after starting treatment. In the ABI/PSL group, 12 patients (46%) showed elevations of PSA and 7 patients (27%) discontinued treatment within 3 months. In contrast, in the ABI/DEX group, only 6 patients (25%) showed elevations of PSA and 3 patients (13%, all were given dexamethasone 1 mg/d) discontinued treatment.
Conclusions:
Dexamethasone and prednisolone may be equally effective in preventing abiraterone-induced hypokalemia.
Introduction
Abiraterone acetate (Zytiga) is a new androgen synthesis inhibitor that has been approved for the treatment of androgen-dependent prostate cancer, particularly metastasized castration-resistant prostate cancer (CRPC). 1 The drug inhibits 17α-hydroxylase/C17,20-lyase (CYP17) that catalyzes the conversion of pregnenolone and progesterone to testosterone precursors, dehydroepiandrosterone and androstenedione, respectively, in testes, adrenal glands, and prostate cancer cells. 2 Although surgical or pharmacological castration effectively abolishes androgen production in the testes, thereby reducing serum testosterone levels to less than 5% compared with control value, the procedure does not eliminate androgen production in adrenal glands and prostate cancer cells.3,4 As a result, combined androgen blockade with an androgen synthesis inhibitor (such as abiraterone acetate) plus castration may provide more extensive androgen deprivation than castration alone, with better therapeutic response for patients with CRPC.
In early clinical trials, abiraterone acetate was administered alone to patients with CRPC. Although the drug showed favorable antitumor effects in these studies, many participants experienced adverse reactions compatible with hyperaldosteronism (hypokalemia [48%-88%], fluid retention [5%-31%], and hypertension [17%-40%]).5–7 These adverse drug reactions were attributed to the augmented secretion of adrenocorticotropic hormone that was caused by the disruption of negative feedback by serum cortisol after the administration of abiraterone. Abiraterone inhibits CYP17 which is responsible for the synthesis of not only androgens mainly in the testes but also cortisol in the adrenal glands. 8 As a result, abiraterone was recommended to be administered with either prednisolone or prednisone 10 mg/d in later clinical trials.9–11 However, it remains unclear whether glucocorticoids other than prednisolone or prednisone may also be co-administered with abiraterone. Theoretically, dexamethasone may be superior to prednisolone or prednisone for preventing abiraterone-induced hyperaldosteronism because dexamethasone has no mineralocorticoid effects, whereas prednisolone has some. Nevertheless, at present, only prednisolone or prednisone 10 mg/d is recommended to be used with abiraterone for preventing secondary hyperaldosteronism according to the prescribing information of the drug.
Administration of a glucocorticoid in patients with advanced prostate cancer may have beneficial effects by itself. Tannock et al 12 reported that the administration of low-dose prednisone (7.5-10 mg daily) gave symptomatic relief of pain in 38% of patients with advanced prostatic cancer in their retrospective study. In subsequent clinical trials, dexamethasone was most extensively investigated in patients with CRPC, and some promising outcomes have been reported.13–15 Consequently, clinical trials of nonhormonal therapies against CRPC often included concomitant use of glucocorticoids for facilitating comparisons with previous studies where various antineoplastic agents were co-administered with low-dose prednisone or prednisolone. In this context, we undertook a retrospective, observational study to address whether the co-administration of dexamethasone (0.5 or 1 mg/d) or prednisolone (10 mg/d) with abiraterone in patients with CRPC would have different effects on serum potassium levels and time courses of serum prostate-specific antigen (PSA).
Methods
Data collection
We retrieved the clinical data of all patients with CRPC who were treated with abiraterone 500 or 1000 mg/d and either prednisolone 10 mg daily (ABI/PSL group) or dexamethasone 0.5 or 1 mg once daily (ABI/DEX group) at Juntendo University Nerima Hospital between November 2014 and August 2017. We adopted no exclusion criteria for patients as far as their clinical courses of the abiraterone therapy were monitored from the beginning to 3 months thereafter. However, patients who had initiated the abiraterone therapy at other hospitals before they were referred to our institution were excluded from the study because no data about baseline and initial responses in laboratory tests were available. We did not perform any statistical considerations for sample size before the study had begun because this study was retrospective in design and performed in a single center. All clinical data were handled carefully for protection of privacy according to the guidelines for epidemiologic studies and clinical studies issued by the Ministry of Health, Labour and Welfare. We collected demographic data (age and body weight) as well as metastatic sites (bone, lymph node, and other organs) prior chemotherapeutic agents for prostate cancer and laboratory data (serum PSA, potassium, sodium, and creatinine levels) from the electronic medical records. Severity of adverse reactions observed from serum biochemistry and electrolytes was graded according to the criteria of Common Terminology Criteria for Adverse Events (CTCAE) version 4.0. 16 Time course of serum PSA concentration was also monitored as a surrogate biomarker of therapeutic response for 3 months after the commencement of abiraterone therapy. A relative elevation of serum PSA level of 25% or greater, or an absolute elevation of 2 ng/mL or greater from the baseline value was considered clinically significant. 17 The research protocol was approved by the institutional review board before the study was begun (approval number: 27-13).
Statistical analysis
The primary outcome of interest was to compare the mean changes in serum potassium levels after initiation of abiraterone therapy with either dexamethasone or prednisolone. The secondary outcomes of interest were to compare (1) the severity of hypokalemia induced by abiraterone acetate, (2) the time course of PSA levels, and (3) the treatment failure assessed by clinically significant PSA increase between the patients receiving abiraterone with dexamethasone and prednisolone.
Comparisons of mean values between 2 groups were conducted by either Student t test or Mann-Whitney U test for continuous variables. Either χ2 test or Fisher exact test for categorical variables was employed where appropriate. Comparisons of mean serum potassium levels obtained before and after abiraterone administration were conducted either using paired t test or Wilcoxon rank sum test where appropriate. We also performed a statistical analysis on whether abiraterone dose (500 or 1000 mg/d) was associated with changes in serum potassium or PSA levels in the ABI/DEX group. We used JMP Pro 11 (SAS Institute Inc., Cary, NC, USA) for all statistical analyses. P value less than .05 was considered statistically significant.
Results
Patient background
We retrieved 55 patients with CRPC who were treated with abiraterone from our medical records. After excluding 2 patients who had initiated the abiraterone therapy at other hospitals, we identified a total of 53 eligible patients for this study: 27 in the ABI/PSL group and 26 in the ABI/DEX group. Although most of the patients received abiraterone 1000 mg/d, 4 patients (3 in ABI/PSL group and 1 in ABI/DEX group) received abiraterone at 500 mg/d. It is difficult to identify specific reasons why the dose reduction was undertaken in these patients. It could have been attributed to the attending physicians’ comprehensive judgment based on body size, ages, and performance status. In the ABI/PSL group, prednisolone was administered concurrently with abiraterone from treatment initiation in 23 patients, prednisolone was switched from dexamethasone 0.5 mg/d (n = 1) or 1 mg/d in 1 patient, or prednisolone had been administered before abiraterone was started in 2 patients. In the ABI/DEX group, dexamethasone was administered concurrently with abiraterone from treatment initiation in 4 patients or it had been administered before abiraterone was started in 22 patients. In the ABI/DEX group, 21 patients received 0.5 mg/d and 5 received 1 mg/d of dexamethasone. The standard dose of dexamethasone for patients with prostate cancer was 0.5 mg/d in the hospital, whereas the dose was sometimes increased to 1 mg/d by attending physicians’ judgment on subjective or objective improvement in patients.
Table 1 shows the relevant demographic and laboratory data obtained from patients before abiraterone therapy was initiated. There were no significant differences between the ABI/PSL and ABI/DEX groups in most clinical and biochemical variables (Table 1). However, the median value for the time elapsed from the patients who received ABI/DEX was significantly (P < .05) longer than those received ABI/PSL. Although the median serum PSA level at baseline obtained from the ABI/DEX group appeared higher than that in the ABI/PSL group, no significant difference was observed between 2 groups (Table 1). There was no relationship between baseline PSA level and the time elapsed after initiation of first chemotherapy for prostate cancer.
Demographic and clinical characteristics of patients with castration-resistant prostate cancer.

Abbreviations: ABI/DEX, abiraterone plus dexamethasone group; ABI/PSL, abiraterone plus prednisolone group; LHRH, luteinizing hormone–releasing hormone; NS, not significant; PSA, prostate-specific antigen.
Data are expressed as mean ± standard deviation, median (interquartile range), or number (percentage).
P values were obtained from Student t test for parametric variables, Mann-Whitney U test for nonparametric variables, and χ2 test or Fisher exact test for categorical variables.
Leuprorelin acetate, goserelin acetate, or degarelix acetate.
Data were calculated from 26 patients because no complete information on prior maximum androgen blockade therapy was obtained in 1 patient.
Effects of ABI/PSL and ABI/DEX therapies on laboratory data
Table 2 summarizes the effects of ABI/PSL and ABI/DEX therapies on laboratory data according to the doses of glucocorticoids and abiraterone. Because there appeared no significant differences in the baseline serum potassium concentrations within ABI/PSL and ABI/DEX in terms of differences in doses of abiraterone or glucocorticoids, we combined the data together into the 2 groups irrespective of differences in the doses of abiraterone and glucocorticoids within the groups. There were no significant differences between serum potassium concentrations at baseline and those after commencement of abiraterone therapy in the ABI/PSL group (4.29 ± 0.37 mEq/L versus 4.27 ± 0.43 mEq/L) and in the ABI/DEX group (4.13 ± 0.36 mEq/L versus 4.12 ± 0.38 mEq/L) (Figure 1). Daily dose of dexamethasone (0.5 or 1 mg) had no effect on the change in serum potassium level in the ABI/DEX group (Table 2). In addition, there were no significant differences between the groups in the mean change in serum potassium concentration (−0.02 ± 0.47 mEq/L in the ABI/PSL group versus −0.02 ± 0.45 mEq/L in the ABI/DEX group) (Figure 1). Although 1 patient in the ABI/PSL group and 3 patients in the ABI/DEX group developed grade 1 hypokalemia, they recovered promptly by oral potassium chloride supplementation. Because the data of blood pressure and body weights were incomplete, no statistical analysis was undertaken for these parameters.
The effects of co-administration of either dexamethasone or prednisolone with abiraterone on laboratory data.

Abbreviations: DEX, dexamethasone; PSA, prostate-specific antigen; PSL, prednisolone.
Data are presented as mean ± standard deviation, median (interquartile range), or number (percentage).
Defined as serum potassium concentrations between 3.0 and 3.5 mEq/L according to the criterion of Common Terminology Criteria for Adverse Events version 4.0.
Data obtained from the last observation in the study period for each patient. No posttreatment PSA had not evaluated from 2 patients in abiraterone 1000 mg/d + DEX 0.5 mg/d group and 1 patient in abiraterone 1000 mg/d + PSL 10 mg/d group.

Changes in serum potassium concentration from baseline (pre) to after the commencement (post) of co-administration of abiraterone and prednisolone (ABI/PSL) or dexamethasone (ABI/DEX). Data are expressed as mean ± standard deviation. Open circle denotes co-administration of prednisolone 10 mg/d, gray diamond dexamethasone 0.5 mg/d, and closed circle dexamethasone 1 mg/d.
Serum PSA concentrations during abiraterone therapy were obtained from 51 of 53 patients. The time course for each patient was plotted as percent change in PSA relative to baseline for 3 months after the commencement of abiraterone therapy (Figure 2). In the ABI/PSL group, 12 patients (46%) showed elevation of serum PSA defined as either ≥25% or ≥2 ng/mL increase from baseline, and 7 patients (27%) discontinued abiraterone therapy within 3 months from the initiation of the therapy due to >50% PSA increase compared with baseline. In the ABI/DEX group, 6 patients (24%), comprising 2 (10%) patients receiving dexamethasone 0.5 mg/d and 4 (80%) receiving 1 mg/d, showed clinically significant elevation of PSA, 3 of whom who received dexamethasone 1 mg/d discontinued abiraterone therapy within 3 months due to treatment failure. The difference in percentages of elevation in PSA between ABI/PSL and ABI/DEX groups did not reach a statistically significant level (P = .120). No significant dose dependency was observed for changes in serum potassium and PSA levels between patients receiving abiraterone at either 500 or 1000 mg/d.
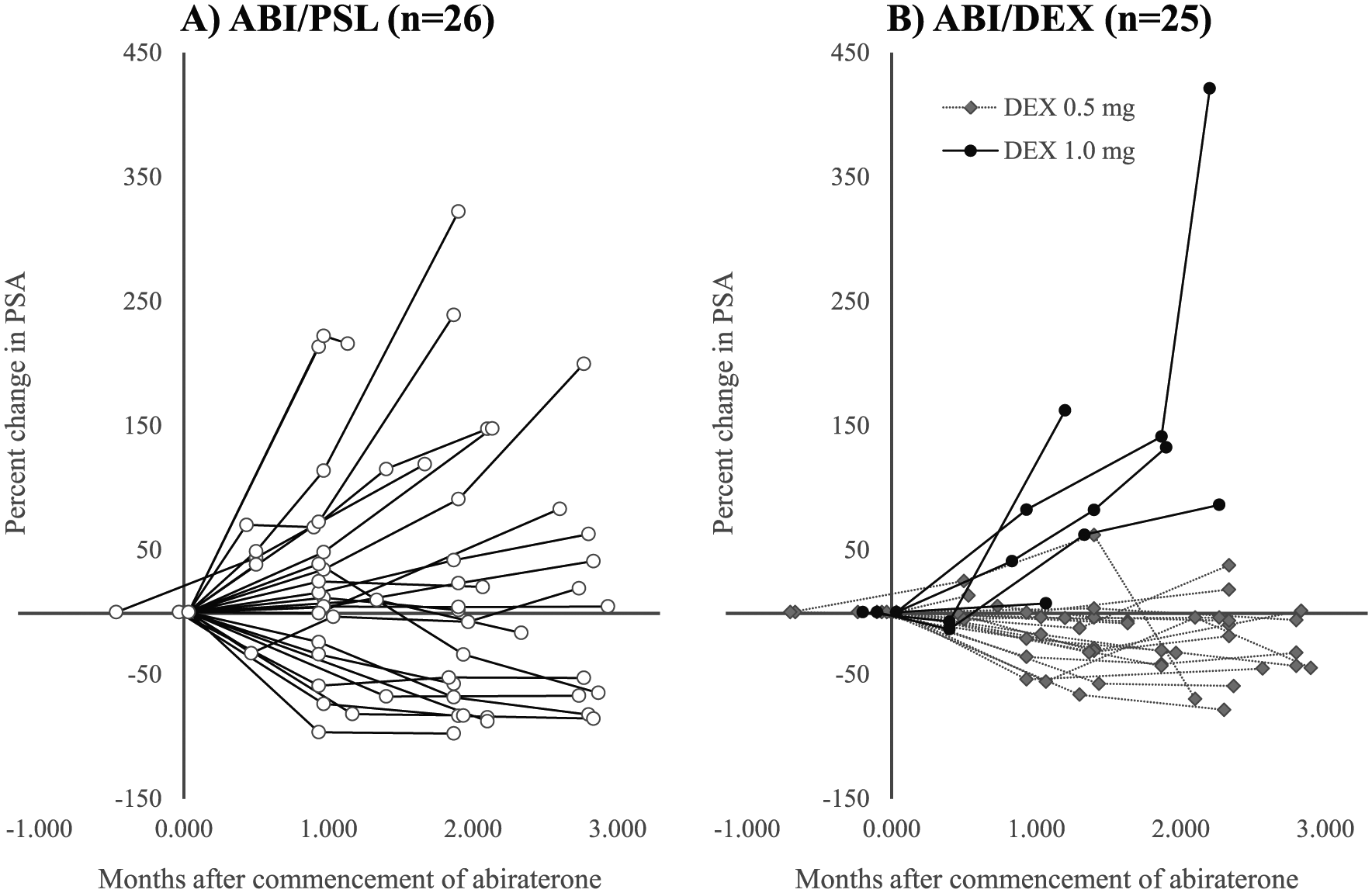
Time courses of serum PSA (percent change from baseline) in patients receiving abiraterone with either dexamethasone (ABI/DEX) or prednisolone (ABI/PSL). Open circle denotes co-administration of prednisolone 10 mg/d, gray diamond dexamethasone 0.5 mg/d, and closed circle dexamethasone 1 mg/d.
Discussion
This study is, to our knowledge, the first to compare time courses of serum potassium and PSA between patients with CRPC receiving abiraterone with prednisolone and those with dexamethasone. The results indicated that the administration of dexamethasone 0.5 or 1 mg/d was largely comparable in efficacy for preventing abiraterone-induced hypokalemia compared with prednisolone 10 mg/d (Figure 1). Our data are consistent with those of Lorente et al 18 who reported observational data on the clinical courses of patients with CRPC receiving abiraterone combined with prednisolone or prednisone initially and then switched to dexamethasone due to tumor progression. They revealed that the prevalence of abiraterone-associated hypokalemia was higher during the preswitch period (28.6%) when abiraterone was given with prednisolone than that during the postswitch period (7.1%) when abiraterone was given with dexamethasone. Our study and that of Lorente et al 18 were retrospective in design, whereas no prospective study comparing the potassium-retaining effects of dexamethasone and prednisolone has been reported to date. Whether dexamethasone, such as prednisolone or prednisone, can be recommended to be used with abiraterone in patients with CRPC for preventing hypokalemia remains to be confirmed in a prospective study. According to the information posted on ClinicalTrials.gov, a randomized phase 2 study evaluating abiraterone with different steroid regimens (prednisone at 5 and 10 mg/d and dexamethasone at 0.5 mg/d) for CRPC is underway (NCT01867710: https://clinicaltrials.gov/ct2/show/NCT01867710) and the results will be available soon.
As a serendipitous observation, we found that co-administration of dexamethasone 0.5 mg/d with abiraterone in patients with CRPC appeared to yield lesser elevations than those of dexamethasone 1 mg/d or prednisolone 10 mg/d regarding the time course of serum PSA levels (statistical comparison was not made) (Figure 2). Our data appear to imply that the antitumor effect of abiraterone may be influenced by the potency of glucocorticoid receptor stimulation elicited by glucocorticoids administered concomitantly. It is generally believed that prednisolone 10 mg/d and dexamethasone 1.5 mg/d have comparable glucocorticoid effects. 19 Arora et al 20 reported that activation of glucocorticoid receptor by prednisolone-induced resistance to enzalutamide, an androgen receptor antagonist. They also revealed that resistance to enzalutamide was reversed by switching prednisolone to dexamethasone at doses associated with less glucocorticoid receptor stimulation. It remains unknown whether the mechanism of resistance to enzalutamide is applicable to abiraterone. Nevertheless, a previous randomized study with a small number of patients with CRPC (n = 82) demonstrated that there was a tendency (P = .08) of greater suppressive effects on the PSA time courses in patients receiving abiraterone with dexamethasone 0.5 mg/d (41%) than in patients receiving abiraterone with prednisolone 10 mg/d (22%). 21 In addition, a retrospective analysis of patients with CRPC (n = 30) undergoing a switch from prednisolone to dexamethasone while on abiraterone due to progression of PSA demonstrated that 39% of the patients showed a 30% or greater decline in serum PSA level after switching compared with the preswitch level. 18 Collectively, previous studies and our data were obtained from small numbers of patients and retrospective in design. In this context, clinical studies should be conducted to explore the best glucocorticoids and the optimal doses to be co-administered with abiraterone to achieve favorable antitumor effect.
This study has some drawbacks that are inherent to retrospective studies. For instance, the patients given dexamethasone 1 mg/d had a longer disease duration (median: 2610 days, interquartile range: 1694-2672 days) than those given dexamethasone 0.5 mg/d (median: 2181 days, interquartile range: 1489-3301 days). As a result, the patients given dexamethasone 1 mg/d may have had more advanced prostate cancer compared with those given dexamethasone 0.5 mg/d. The observed differences in the time course of serum PSA between ABI/PSL and ABI/DEX might have been caused by the difference in sensitivity to abiraterone rather than the difference in dose of dexamethasone. Because dose selection of dexamethasone was made by physicians’ comprehensive judgment, patients given dexamethasone at 1.0 mg/d might have had tumors being more resistant to abiraterone. In addition, our sensitivity analysis of the contribution of abiraterone dose (500 or 1000 mg/d) to changes in serum potassium, and PSA levels failed to raise possibility of dose dependency because of small sample size and uncontrollable confounding factors. Prospective, randomized studies are required to verify the present findings obtained from a retrospective study with a small sample size.
Conclusions
We observed that co-administration of dexamethasone 0.5 or 1 mg/d and co-administration of prednisolone 10 mg/d were equally efficacious in the prevention of abiraterone-induced hypokalemia.
Footnotes
Acknowledgements
The authors are grateful to the peer reviewers and the Editor-in-Chief (William Cho) for their helpful input into the revision of this manuscript.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MT and RO participated in designing the protocol of the present study. MT and RO were responsible for statistical analyses of the data. NK, SK, FS, YS, KS, HE, and AM participated in interpretation of the data and contributed to discussions. MT, RO, and HE worked together in drafting the manuscript. All authors read and approved the final manuscript.
Availability of Data and Material
The data sets generated during and/or analyzed during this study are not publicly available for protection of individual privacy but are available from the corresponding author on reasonable request.