
Abstract
Background:
Dyslipidemia is a condition where lipid metabolism is altered, and its mechanism is closely related to non-alcoholic fatty liver disease. The alteration of lipid metabolism during non-alcoholic fatty liver disease results in disrupted uptake, oxidation, and export. Assessing dyslipidemia among non-alcoholic fatty liver disease using these lipid panel is affordable, widely available, and compatible with existing laboratory infrastructure which enables for identifying individuals at increased risk of its complications, guiding therapeutic interventions, and supporting metabolic risk management.
Objective:
The study aimed to assess Dyslipidemia and its associated factors among non-alcoholic fatty liver disease-diagnosed type 2 diabetes mellitus patients in Adama Hospital Medical College, 2024.
Methods:
An institution-based cross-sectional study design was used, and the study units were selected using a systematic random sampling technique. Sociodemographic, Behavioral, and Clinical data were collected using a structured questionnaire. Anthropometric measurements were taken by experienced nurses. Fasting venous blood was collected to test the lipid profiles and fasting blood glucose of study participants using Siemens Healthineers dimension EXL 200 chemistry analyzer. Data were assessed using STATA version 17 for correlation analysis among lipid parameters and the predictors, and P < .05 was considered statistically significant. Binary logistic regression was performed to show the statistically significant association among dyslipidemia and associated factors, and P < .05 was also considered statistically significant.
Results:
The overall proportion of dyslipidemia was found to be 199 (85.04%). High TG 128 (54.7%) and low HDL-C 121 (51.71%) accounts for the major abnormal lipid parameters. BMI, blood pressure, and non-alcoholic fatty liver disease showed a weak positive statistical correlation with increased LDL-C, TG, and TC and a weak negative statistical correlation with HDL-C. The odds of lack of regular exercise and non-alcoholic fatty liver disease were higher for developing dyslipidemia.
Conclusions:
The overall prevalence of dyslipidemia was found to be high among non-alcoholic fatty liver disease-diagnosed type 2 diabetes mellitus patients. Hypertriglyceridemia was found to be highly prevalent, followed by low HDL-C, and high LDL-C.
Introduction
Non-alcoholic fatty liver disease (NAFLD) is defined as the presence of ⩾5% hepatic steatosis without a competing liver disease such as viral hepatitis, autoimmune hepatitis, hemochromatosis, Wilson’s disease, or alcoholic liver disease, and without the use of steatosis-inducing medications. 1 NAFLD is found in approximately two-thirds of obese individuals and half of patients with type 2 diabetes (T2DM). The presence of the metabolic syndrome is associated with non-alcoholic steatohepatitis and advanced fibrosis among NAFLD patients. 2
The global prevalence of NAFLD increased from 25.8% in 1990 to 2006 to 38% in 2016 to 2019. 3 Worldwide 589 million people live with T2DM which is 11.1% of the world population. It is estimated that it will reach at 853 million in 2050 with large increasing in Africa. 4 It is well recognized that T2DM and NAFLD commonly coexist and work synergistically to raise the risk of adverse clinical outcomes, both hepatic and extra-hepatic. 5 A recent studies in Ethiopia showed high prevalence of NAFLD among T2DM patients with including disruption of lipid profile.6,7 Adipose tissue lipolysis is facilitated by T2DM and insulin resistance. This results in the release of free fatty acids, which are then deposited in the liver and cause steatosis. In addition to liver-related mortality, T2DM is a major risk factor for developing progressive non-alcoholic steatohepatitis, cirrhosis, and fibrosis. 8 Different studies showed the coexistence of NAFLD and T2DM. Studies conducted in Ethiopia around different regions showed the prevalence of NAFLD among T2DM patients as 73% 9 and 48.3%. 6
Dyslipidemias are alterations to the plasma lipid profile that are often associated with clinical conditions. They are classically characterized by abnormal serum levels of cholesterol, triglycerides, or both, involving abnormal levels of related lipoprotein species. 10 Primary or family dyslipidemias are genetically determined, while secondary dyslipidemias are more frequently caused by other illnesses such diabetes mellitus, obesity, non-alcoholic fatty liver disease, or an unhealthy lifestyle. 11
Dyslipidemia is caused by impaired hepatic lipid metabolism pathways in NAFLD. The altered lipid metabolism in NAFLD leads to elevated hepatic triglycerides (TG). De novo lipogenesis is increased by elevated plasma insulin and glucose levels, respectively. As a result, mitochondrial activity and fatty acid oxidation are decreased. 12 Increased hepatic TG content leads to higher TG secretion and, as a consequence, increased plasma TG levels. The liver absorbs less low density lipoprotein (LDL) when intracellular cholesterol levels are elevated. 13 The combination of these alterations promotes the development of foam cells and, eventually, atherosclerosis by raising large very low-density lipoprotein (VLDL1) and small dense LDL. 14
The global burden of dyslipidemias has accounted 28.8% with hypertriglyceridemia followed by hypercholesterolemia (low HDL-C and high LDL-C). 15 Major risk factors for cardiovascular disease include dyslipidemias, especially increased plasma LDL-cholesterol levels. However, other types of dyslipidemias, such hypertriglyceridemia, are linked to serious illnesses in other organ systems, such as acute pancreatitis and NAFLD.16,17 Hypercholesterolemia is the most common form of dyslipidemia. In 1990, raised plasma LDL-cholesterol levels were the 15th most important risk factor for death; by 2007, that number had risen to 11th, and by 2019, it had risen to 8th. The higher incidence of VLDL remnants, VLDL, LDL, and combination dyslipoprotinemia is independently linked to NAFLD rather than advanced hepatic fibrosis. 18
Increases in plasma lipid levels and the incidence of dyslipidemias in low-income nations have been primarily caused by rapid economic expansion, dietary changes, and the adoption of unhealthy lifestyles. It is important to control the dyslipidemia linked to NAFLD because of the substantial cardiovascular risk. 19 Therefore, optimizing the lifestyle through a rational diet and exercise intervention is undoubtedly the basis and important link of NAFLD treatment. The combination of drugs, which can effectively regulate glucose and lipid metabolism and reduce liver inflammation and fibrosis, might be more beneficial for the treatment of NAFLD. 20 The assessment of dyslipidemia among NAFLD diagnosed patients is very important in reducing the clinical impact of the disease complications such as cardiovascular disease which is the leading cause of mortality in NAFLD patients, predicting the disease severity and progression, and monitoring treatment response and treatment individualization. It is also crucial in enabling the early detection and prevention strategies, guideline development and resource allocation, and epidemiological surveillance. In Ethiopia there is lack of a comprehensive study on assessing dyslipidemia among NAFLD diagnosed T2DM patients. Therefore, the study aimed to assess dyslipidemia and its associated factors among NAFLD diagnosed T2DM patients.
Methods and Materials
Study Design, Period, Area, and Setting
An institutional-based cross-sectional study design was conducted to assess dyslipidemia and its associated factors among NAFLD diagnosed T2DM patients at Adama Hospital Medical College, South Eastern Ethiopia, from May to August, 2024. Adama Hospital Medical College is located in Adama city, which is found in Oromia region, East Shewa Zone, 99 km away from the capital Addis Ababa.
Study Population
The study included T2DM patients who had diagnosed positive for NAFLD, visited the DM clinic during the study period, and who fulfilled the eligibility criteria.
Eligibility Criteria
Inclusion Criteria
All adult patients with T2DM who had a follow-up, diagnosed positive for NAFLD, and visited the DM clinic of Adama Hospital Medical College during the study period.
Exclusion Criteria
People using lipid lowering drugs currently, who had a known history of chronic liver disease other than NAFLD, renal diseases, and pregnant or lactating women were also excluded.
Sample Size Determination and Sampling Technique
Since there was lack of study conducted in Ethiopia on the assessment of dyslipidemia and its associated factors among NAFLD diagnosed T2DM patients a single population proportion formula with a 95% confidence level and a 5% marginal error used with the assumption of 50% proportion to obtain the maximum possible size. The sample size became 385, and after adding for a 10% nonresponse rate, it reached to 424. However, a finite population correction formula is required as the total number of population was 520 which was less than 10,000, and the last sample size was 234. The study participants were chosen using a systematic random sampling technique. The calculated for the systematic random sampling was 2. Therefore, study participants were interviewed at every second interval, and the first study participant was chosen by the lottery method.
Study Variables
Outcome Variable
Dyslipidemia.
Independent Variables
Sociodemographic characteristics such as age, sex, marital status, and occupational status. Anthropometric measurements such as BMI and clinical factors such as NAFLD status, duration of DM and blood pressure and behavioral characteristics such as exercise habits.
Operational Definition
Dyslipidemia was characterized by a single or combined lipid abnormalities in the lipid profile. Each lipid profile parameters taken as abnormal when LDL-C > 100 mg/dl, HDL-C < 40 mg/dl, TG > 150 mg/dl, and TC > 200 mg/dl. 21
Data Collection Process and Laboratory Methods
All T2DM patients with the age of ⩾18 years and who were diagnosed for NAFLD using ultrasonography were recruited after the purpose of the study had been explained to them and they provided written informed consent. Experienced nurses conducted face-to-face interviews with study participants using a structured questionnaire. Clinical data were also collected by experienced nurses from the chronic case unit OPD by looking at their charts and measuring BP. BP was measured using Mercury sphygmomanometer from left upper arm and positioned at the heart level. BP results were classified as higher when systolic ⩾ 140 mm/Hg and diastolic ⩾ 90 mm/Hg. 22
The research participants’ height and weight were measured using a stadiometer. Shoes and hats were removed from the participant before the height assessment. The height was calculated to be within 0.1 cm. Participants were instructed to take off any extra layers of clothing, shoes, jewelry, and anything in their pockets before standing with their weight equally spread between both feet, their arms at their sides, palms facing in the direction of their thighs, and their heads up and facing forward. Finally, weights were measured to the nearest 0.1 kg. BMI was then determined by dividing weight in kilograms (kg) by height in meters squared (m2). The classification of BMI was based on WHO categorization as underweight < 18.5 kg/m2, normal weight 18.5 to 24.9 kg/m2, and ⩾25 kg/m2 overweight. 23
After an over-night fast of 8 to 12 hours, an experienced medical laboratory technologist collected 5 ml venous blood from patients with T2DM who visited chronic care unit of the hospital. The collected blood was poured into a serum separator test tube (SST), then left for 30 minutes while it clotted. The blood was centrifuged at 3500 rpm for 5 minutes, and the serum was used for lipid profiles and fasting blood sugar tests. A skilled laboratory technologist examined the FBS, and lipid profile using Siemens Healthineers Dimension model EXL 200 clinical chemistry analyzer catalog number of 23-313-015 with advanced LOCI technology. It uses integrated photometric, immunoassay, and QuikLYTE IMT methods without manual reagent preparation. The analyzer uses enzymatic colorimetric (photometric) methods with specific, ready to use flex reagent cartridges. The intensity of the colored compound resulted from a series of enzymatic reactions is directly proportional to the concentration of lipid parameter at specific wave lengths. To exclude hepatitis B virus, hepatitis C virus, and pregnant women, a rapid chromatographic immunoassay strip test was used.
Data Quality Assurance
The questionnaire was first prepared in English and then translated into local languages (Amharic and Affan Oromo), it was translated back into English to check its consistency. Data collectors were trained, and regular supervision was carried out to ensure the quality of the data. The data were checked for completeness and sample labeling, adequacy, proper container, hemolysis, and proper volume. Anthropometric measurements were taken twice, and the average of the 2 was used. Finally, at each stage of laboratory analysis (pre-analytical, analytical, and post-analytical), the manufacturer’s instructions, standard operating procedures, and quality assurance were followed. Calibration was performed initially at the startup of using the machine and quality controls were performed every morning before any sample run using manufacturer prepared quality control reagents. All types of reagents and test kits used were checked for their expiration dates. The findings were carefully documented, transcribed, and evaluated.
Data Analysis and Interpretation
Data were cleaned, edited, entered, and analyzed by using STATA version 17. Variables were described using frequency tables and descriptive summaries. Pearson correlation analysis was performed among lipid parameters and predictor variables to measure the strength and direction of the relationship of the variables and P ⩽ .05 were taken as statistically significant. Binary logistic regression was performed to show the association of variables with dyslipidemia. Variables in bivariate analysis with P < .25 were taken as candidates for multivariate analysis. Multiple logistic regression analysis was used to identify associated risk factors for the prevalence of dyslipidemia. P-value was set at <.05 for statistical significance.
Results
Sociodemographic Clinical and Behavioral Characteristics of Study Participants
A total of 234 NAFLD diagnosed T2DM patients were participated and 120 (51.28%) of them were female and more than half 135 (57.69%) were below the average age (47.9). About 210 (89.74%) of them were married, 77 (32.9%) of them were government employee, and 102 (43.59%) of them were completed college or university. majority of the study participants were overweight 110 (47.02%) and less than half of the participants exercise regularly. The NAFLD status of the T2DM patients were 109 (46.58%) mild, 97 (41.45%) moderate, and 28 (1.97%) severe (Table 1).
Sociodemographic, Clinical, and Behavioral Characteristics of NAFLD Diagnosed T2DM Patients in Adama Hospital Medical College (n = 234).

Dyslipidemia Among Study Participants
The mean ± standard deviation (SD) of the LDL-C, HDL-C, TG, TC, were 93.2 ± 38.93, 41.38 ± 22.78, 173.51 ± 100.3, 155.78 ± 47.34 respectively. In this study the general proportion of dyslipidemia was 199 (85.04%; Figure 1).

The prevalence of dyslipidemia among different NAFLD status in Adama Hospital Medical College (n = 234).
When the single components of dyslipidemia were analyzed, higher LDL-C was found in 101 (43.16%), lower level of HDL-C was found in 121 (51.71%), higher TG was found in 128 (54.7%), and higher TC found in 41 (17.52%) of study participants (Table 2).
Distribution and Prevalence of Components of Dyslipidemia Among NAFLD Diagnosed T2DM Patients in Adama Hospital Medical College (n = 234).

Correlation Analysis of Lipid Profile with Predictors of Study Participants
The statistically positive correlation was found between serum LDL-C with BMI, and NAFLD. A statistically weak negative correlation was found between HDL-C with BP, and BMI. TG with BMI, and NAFLD; TC with age, BMI, and NAFLD showed a statistically weak positive correlation (Table 3).
Correlation Analysis of Lipid Profile with Predictors Among NAFLD Diagnosed T2DM Patients in Adama Hospital Medical College (n = 234).

Statistically significant P ⩽ .05 in Pearson correlation analysis.
The assessment of sociodemographic, clinical, and behavioral factors using binary logistic regression showed that NAFLD diagnosed T2DM patients who had not exercise regularly have higher odds of having dyslipidemia as compared to individuals who exercised regularly and with severe status of NAFLD as the reference category, dyslipidemia was associated with the mild and moderate status of NAFLD, with the highest odd observed for moderate NAFLD status (Table 4).
Binary and Multivariable Logistic Regression Analysis of Dyslipidemia Among NAFLD Diagnosed T2DM Patients in Adama Hospital Medical College (n = 234).
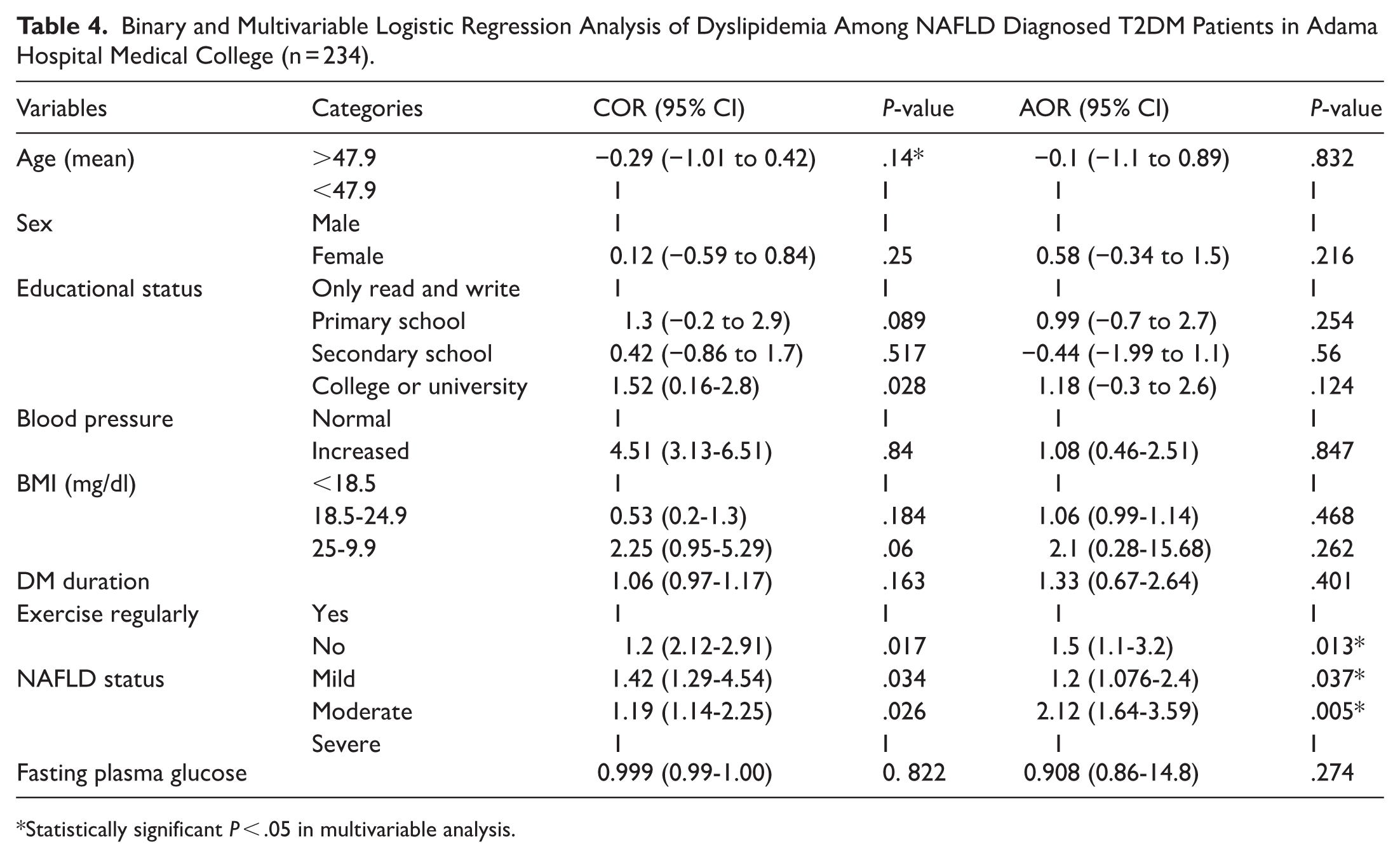
Statistically significant P < .05 in multivariable analysis.
Discussion
Metabolic disturbances involving insulin resistance and hepatic fat accumulation interconnected T2DM, NAFLD, and dyslipidemia pathways. Insulin resistance may cause failing to suppress hormone sensitive lipase and results adipose tissue lipolysis which increases the delivery of free fatty acids to the liver. Those free fatty acids re-esterified in liver and increased the TG accumulation and promotes over production of VLDL. This lead to NAFL and later NASH. The continuous disruption of lipids result abnormal lipid metabolism dyslipidemia. 24 Increasing prevalence of T2DM along with NAFLD worldwide increases the lipid abnormalities which are the main causes for the cardiovascular disease. LDL-C is the major to be associated with the cardiovascular disease and Hypocholesteremia is the most prevalent. 11 Extensive exchange between VLDL and LDL particles further supported by lipolysis of triglyceride-rich particles results in the increased formation of dense small LDL particles. 25 These pathophysiological links between altered systemic lipid-lipoprotein profile and liver fat content have been confirmed in clinical studies. This study aimed to assess dyslipidemia and its associated factors among NAFLD diagnosed T2DM patients. The proportion of dyslipidemia was found 199 (85.04%) and the components of lipid profile abnormality were 101 (43.16%) high LDL-C, 121 (51.71%) low HDL-C, 128 (54.7%) high TG, and 41 (17.52%) high TC. This result was higher from studies conducted china, 26 Pakistan. 27 The discrepancy of the studies may be due to the difference in diagnostic criteria, methods used to diagnose NAFLD which is other than ultrasonography techniques and additional liver function tests, the inclusion of type 1 DM patients, the genetic factors affecting lipid metabolism across populations, sociocultural differences among study areas that may result variety in food intake and other life styles. The increasing of sedentary life style which includes less physical activity and increased use of processed food may be the reason for the increased prevalence.
Higher LDL-C, TC, and TG were statistically weakly positively correlated with BMI and NAFLD and lower HDL-C was statistically weakly negatively correlated with BMI and blood pressure level. This result was in line with studies conducted in and Ethiopia.28,29 The increasing of BMI is directly related with insulin resistance that have a strong pathophysiological linkage in exacerbating NAFLD and T2DM. These may be due to the multiple effect of obesity, hyperglycemia, and NAFLD in the metabolism of lipid. The protective effect of HDL-C prevents oxidation of LDL-C that reduces oxidative stress in vessels preserving normal vascular tone.
NAFLD diagnosed T2DM patients who did not exercises regularly have higher odds of developing dyslipidemia as compared to those who exercise regularly. The finding of this study was similar with studies conducted in China 30 and Italy. 31 The major abundant cause for increasing NAFLD as well as T2DM is sedentary life style which is directly related with decreased or no exercise. This may later pave the way for the complications of NAFLD and T2DM including dyslipidemia and other metabolic syndromes.
Dyslipidemia was more strongly associated with the mild and moderate status of NAFLD with using the severe status of NAFLD as a reference. This result was similar with study conducted in Pakistan. 27 This may be due to that the liver plays a central role in lipoprotein metabolism as it participates in the production and/or clearance of all classes of lipoprotein particles. In addition to its role in the metabolism of lipoprotein particles, the liver is also a major site of metabolism for their substituent triglycerides and especially cholesterol. There is consequently an intricate link between hepatic metabolic dysfunction in NAFLD and altered lipoprotein metabolism and composition.
Strength and Limitation of the Study
The study assess dyslipidemia among NAFLD diagnosed T2DM patients which can provide relevant insights in to the burden and pattern of dyslipidemia targeting on high-risk population. It yields evidence where data on NAFLD-related dyslipidemia are scarce. Despite the questionnaire was developed based on relevant literature and expert input, it was not formally validated. Additionally the narrow systematic random sampling approach may have resulted selection bias, thereby limiting the external validity of the study.
Conclusions and Recommendations
The proportion of dyslipidemia among NAFLD diagnosed T2DM patients in Adama Hospital Medical College was 85.04%. NAFLD status and lack of physical exercise habit was significantly associated with higher odds of developing dyslipidemia. BMI, blood pressure, and NAFLD were significantly correlated with increased LDL-C, TG, and TC and lower HDL-C. To avoid further complications, it is recommended that routine screening of dyslipidemia and also NAFLD among T2DM patients is very impactful. Policy makers and stake holders should pay significant consideration regarding the increasing of non-communicable diseases including dyslipidemia, NAFLD, and also T2DM.
Footnotes
Acknowledgements
The authors would like to acknowledge the study participants for their voluntary participation in the study and then gratitude extends to Adama Hospital Medical College officials and staffs for their support and creating favorable working condition.
Ethical Considerations
The study was conducted after obtaining ethical clearance from Institutional ethical review board of College of Health Science, Debre Tabor University (Reference Number: 0145/2024). A permission letter was also obtained from Adama Hospital Medical College. Study participants were given an information sheet to understand the study objectives and scopes, and any questions were welcomed. Data collection were done after a signed written consent was obtained. Additionally, they were made aware that they can even stop participating in the study in between of the data collection and the data obtained from them would be kept confidential and used only for research. Any abnormal laboratory findings found during the study period were communicated to the physician for appropriate diagnosis and care. Moreover, all methods were performed in accordance with the relevant guidelines and regulations.
Consent for Publication
Not applicable.
Author Contributions
Mahider Shimelis Feyisa: Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Resources; Software; Supervision; Validation; Visualization; Writing - original draft; Writing - review & editing. Bruktawit Eshetu: Conceptualization; Data curation; Formal analysis; Software; Writing - original draft. Rahel Birhanu Arage: Formal analysis; Methodology; Software; Writing - review & editing. Besfat Berihun Erega: Conceptualization; Data curation; Formal analysis; Validation; Writing - review & editing. Ayenew Berhan: Formal analysis; Methodology; Software; Validation; Writing - review & editing. Teklehaimanot Kiros: Data curation; Formal analysis; Methodology; Supervision; Validation; Writing - review & editing. Getaneh Mola: Conceptualization; Investigation; Methodology; Validation; Writing - original draft; Writing - review & editing. Ermias Bekele Enyew: Data curation; Formal analysis; Investigation; Methodology; Software; Supervision; Validation; Writing - original draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Upon the corresponding author’s request, all the necessary information is made available.