
Abstract
Incidental adrenal cysts are quite rare and thus can present a diagnostic conundrum for even experienced clinicians. Here, we present the case of a patient with an incidentally identified 5 cm adrenal mass. Her evaluation was notable for evidence of mild autonomous cortisol secretion and imaging findings concerning for malignancy with possible invasion of the inferior vena cava. Adrenalectomy was performed; pathology ultimately demonstrated an adrenal cortical pseudocyst without evidence of malignancy. All patients with solid, high-density, or large adrenal tumors require further imaging for characterization and biochemical testing for hormone secretion. While simple, low-density adrenal adenomas and cysts do not require further imaging evaluation beyond non-contrast CT, mixed cystic and solid lesions or pseudocystic lesions should be evaluated similarly to solid tumors, with the caveat that pseudocysts cannot always be well-differentiated from benign cysts on imaging. All adrenal incidentalomas should be evaluated with a biochemical work-up to assess hormonal activity. Tumors suspicious for malignancy require surgical excision. Patients with benign, hormonally active tumors should be managed surgically or medically, according to their primary pathology.
Plain language summary
In this case report, we present a patient with an incidentally found cystic lesion in the adrenal gland. These types of lesions are quite rare and can represent benign or cancerous tumors. We opted to resect this tumor because it had features of a cancerous mass, but it was ultimately found to be benign. All patients with adrenal cysts with concerning features need to be assessed for whether the cysts secrete hormones or whether they have features concerning for cancer. If they do, then the cysts should be removed with surgery.
Introduction
Incidentally discovered adrenal masses are increasingly common, with estimated prevalence ranging from 0.98% to 4.2%. 1 Adrenal cysts, which comprise approximately 1% to 2% of adrenal incidentalomas, are rare amongst adrenal lesions. 2 The evaluation for cystic adrenal lesions, as with that for adrenal incidentalomas in general, is based on evaluating the potential for malignancy and functional status of the lesion. 3 Although simple adrenal cysts are benign and non-hormone secreting, pheochromocytomas and malignant neoplasms can present as cystic or partially cystic masses. Here we present the case of a large, incidentally discovered benign adrenal pseudocyst masquerading as adrenocortical carcinoma (ACC).
Case Description
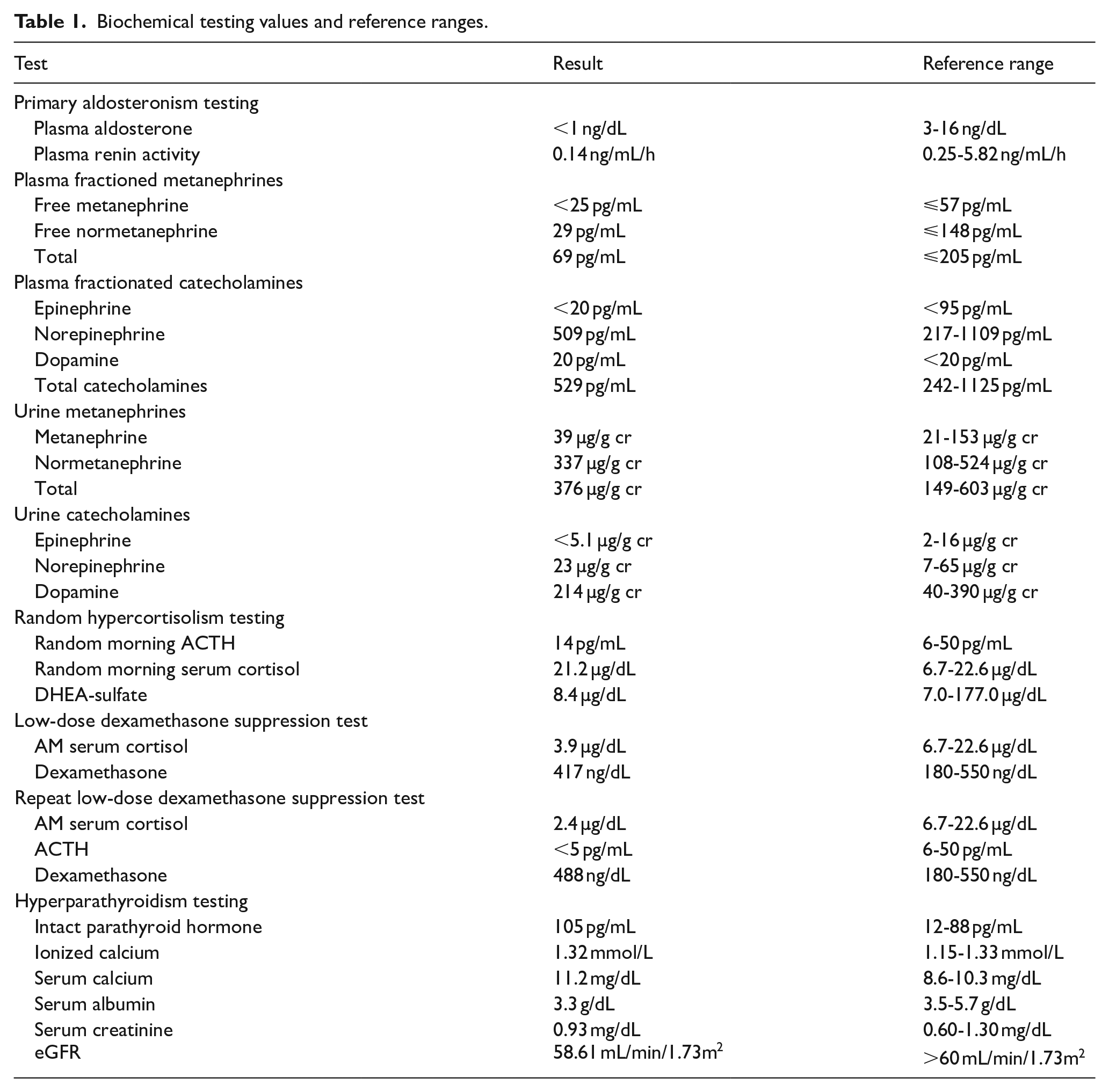
A 76-year-old female with a history of Stage III chronic kidney disease (CKD), right basal ganglia infarct, hypertension, and hypothyroidism presented to a community hospital after a fall at home with significant recent weight loss. She underwent an extensive evaluation for neurologic, cardiovascular, infectious, and metabolic etiologies, all of which were ultimately unrevealing. During this evaluation, she underwent a computed tomography (CT) scan with intravenous contrast of the chest, abdomen and pelvis. She was incidentally found to have a 4.7 cm heterogeneous appearing right adrenal mass with concern for invasion of the inferior vena cava (Figure 1A and B). This mixed cystic and solid mass had a density of approximately 30 Hounsfield units (HU) within the cystic component and 55 HU in the solid component; no washout phase was obtained. Given the mixed solid and cystic components with HU > 10, this mass was interpreted to likely represent an adrenocortical carcinoma or pheochromocytoma; metastatic disease was deemed less likely given the absence of an obvious primary elsewhere on imaging. Follow-up magnetic resonance imaging (MRI) characterized the lesion as an indeterminate 5.2 cm enhancing, bilobed right adrenal mass with intrinsic T1 shortening within the mass, perhaps representative of intratumoral hemorrhage, and enhancement within its superior and posterior aspects. Her biochemical evaluation was notable for suppressed plasma aldosterone and renin activity levels, normal plasma fractionated metanephrines and catecholamines, mildly elevated plasma dopamine, and normal random urine metanephrines/catecholamines and urine dopamine levels (Table 1). A morning adrenocorticotropic hormone (ACTH) was low-normal with high-normal serum cortisol. During her hospitalization, she was also incidentally noted to have labs consistent with primary hyperparathyroidism. After hospital discharge, she underwent endocrinology evaluation including an overnight low-dose 1 mg dexamethasone suppression test (DST) which failed to fully suppress cortisol secretion, suggestive of mild autonomous cortisol secretion (MACS).4 -7

Computed tomography (CT) images showing a heterogenous right adrenal mass (circled in red) with concern for invasion of the inferior vena cava in (A) axial and (B) coronal views. Hematoxylin and eosin immunohistochemistry of the resected right adrenal mass (C and D) demonstrated a cystic mass containing blood, fibrin products and hemosiderin-laden macrophages (blue arrow) encapsulated by a thickened band of collagenous tissue (green arrow) and surrounded by normal adrenal tissue (white star).
Biochemical testing values and reference ranges.
The patient ultimately presented to endocrine surgery clinic at our quaternary academic center a few months after her initial presentation. A repeat low-dose DST was performed, confirming the diagnosis of MACS.
Given the constellation of imaging and biochemical findings, the primary diagnostic consideration was an adrenocortical carcinoma. Laparoscopic transabdominal approach was planned, with high likelihood of conversion to open surgery depending on clinical findings. The procedure was performed under hydrocortisone coverage with administration of 100 mg of IV hydrocortisone on induction and then 50 mg of IV hydrocortisone every 6 hours for 24 hours post-operatively, starting in the recovery area. The procedure was started laparoscopically via transabdominal approach. On mobilization and exposure of the adrenal gland, the adrenal mass was found to be firm and fixed, suspicious for malignancy. The procedure was converted to open through a midline incision to facilitate complete oncologic resection. Completion of the adrenalectomy was uncomplicated and there was no evidence of tumor invasion into the inferior vena cava as had been suspected on preoperative imaging. The patient had an uneventful immediate postoperative course and was discharged on post-operative day 7 on a glucocorticoid taper. The final surgical pathology showed a 6.1 × 4.8 × 4.2-centimeter adrenal cortical pseudocyst without evidence of malignancy (Figure 1C and D). Six weeks after surgery the patient was doing well and had tapered off glucocorticoids.
Discussion
In this case report, we discuss a patient with an incidentally identified large adrenal cyst with imaging characteristics concerning for adrenocortical carcinoma. After resection, this mass was actually found to represent a benign adrenal pseudocyst. While incidental adrenal masses are quite common, cystic lesions are rare and thus represent a diagnostic and therapeutic conundrum for most physicians. Of all adrenal masses, only 1% to 2% are adrenal cysts; while simple cysts are uniformly benign, other cystic masses may represent cystic pheochromocytomas (0.27% of all adrenal masses) or other cystic adrenal malignancies including primary adrenocortical carcinomas and secondary malignancies metastatic to the adrenal gland (0.09%). 2 Thus, a thorough evaluation of malignant potential using imaging features and screening for hormonal excess may be required to exclude pheochromocytoma and malignancies.
In this patient, the final pathology was concordant with an adrenal pseudocyst; adrenal pseudocysts are cystic lesions within the adrenal gland with a fibrous wall rather than an endothelial lining thought to occur secondary to trauma, infection, or bleeding.8 -10 They can also occur in adrenal tumors with cystic degeneration, making it not possible to categorically rule all cystic lesions as benign or hormonally inactive.10,11 This patient also had suggestion of MACS on biochemical testing without any obvious factors affecting absorption or metabolism of dexamethasone as to perhaps lead to a false positive test. Further testing will be necessary to assess resolution of this condition after surgery.
Most adrenal cysts are asymptomatic at presentation, having been discovered incidentally. However, certain aspects of a patient’s history and physical can clue a clinician into the potential etiology. In the setting of cystic pheochromocytoma, symptoms of catecholamine excess such as palpitations, headaches, diaphoresis, and paroxysmal or sustained hypertension may be present. Clinicians should also pay attention to physical exam findings and aspects of the patient’s family history, given the strong heritability and frequent association with genetic syndromes of these tumors. On imaging, cystic pheochromocytomas may have a thick, solid rim with higher CT attenuation, the volume of which may be associated with the level of catecholamine secretion. 12 Adrenocortical carcinomas may also present with symptoms of hormone excess. An estimated 40% to 60% of ACCs are functionally active tumors, most commonly secreting cortisol. 13 However, hormone secretion is not specific to pheochromocytoma and ACC, as benign adrenal pseudocysts can exhibit hormone excess as well, as seen in this case.
In patients with active malignancy, a high index of suspicion for metastasis should be maintained. Compared to simple adrenal cysts, cystic ACCs and metastases are more heterogeneous on imaging and contain a larger solid component. 2 A parasitic adrenal cyst is also on the differential diagnosis but is rare. These cysts are almost exclusively hydatid cysts and should only be considered in patients with characteristic risk factors such as exposure to endemic areas and suspicious imaging findings such as “cysts-within-a-cyst” and peripheral calcification. 2
Ultimately, historical findings, examination, and initial imaging alone may be inadequate to rule out pheochromocytoma or malignancy in a cystic adrenal lesion. In cases of diagnostic uncertainty or suspicious initial imaging findings, suspected adrenal cysts identified on CT may require further evaluation with MRI and biochemical testing (Figure 2). 7 For solid adrenal tumors, additional imaging and testing to rule out autonomous cortisol, aldosterone, androgen, and catecholamine secretion should be considered in accordance with current guidelines, clinical and physical exam characteristics, and initial imaging findings.3,7
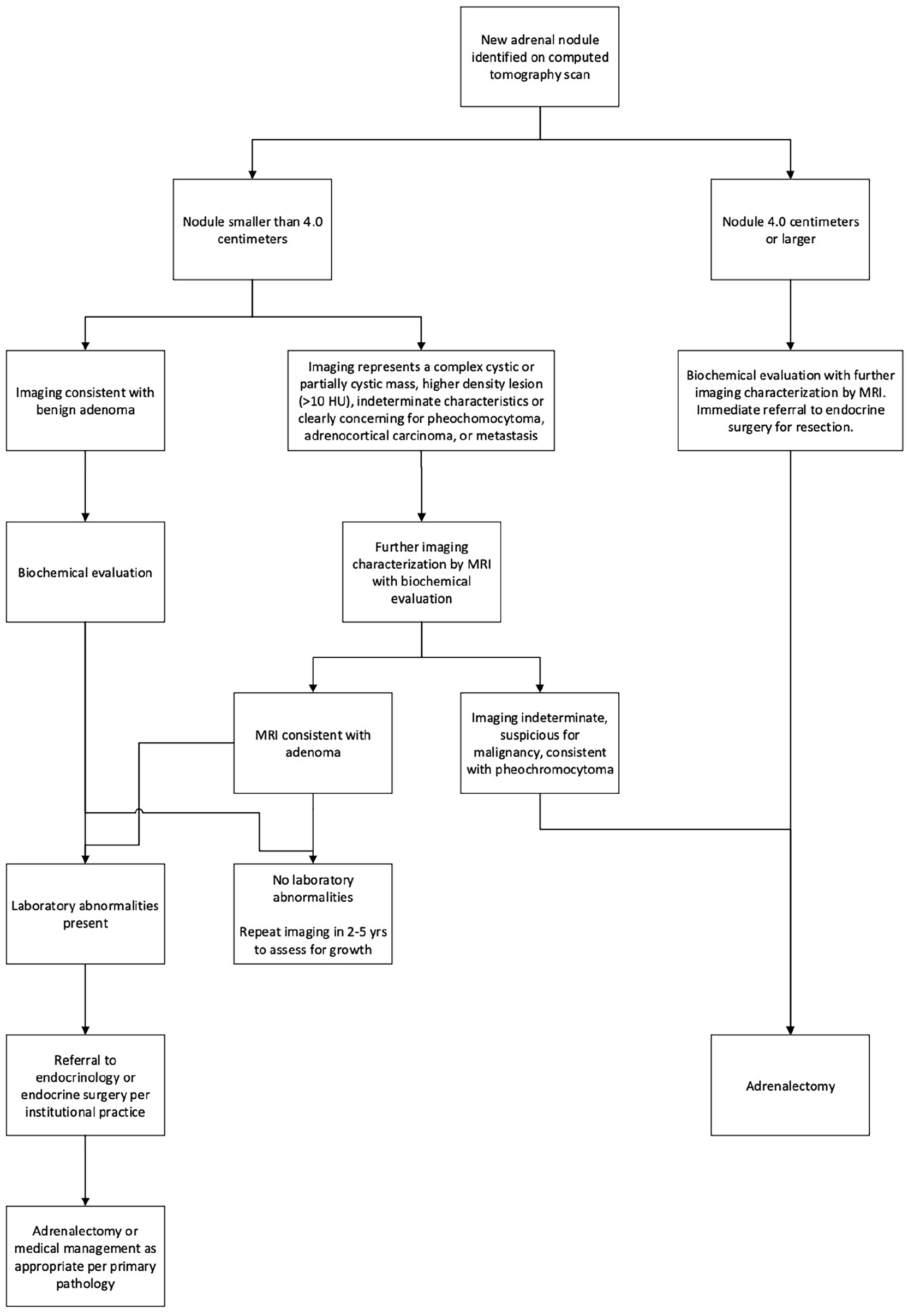
Suggested evaluation pathway for a newly identified adrenal incidentaloma based on our institutional practice, which was developed based on clinical practice guidelines, expert opinion, and health system considerations. Adrenal pseudocysts and solid nodules with cystic components should be treated as suspicious for malignancy and receive additional imaging and biochemical evaluation.
Generally, patients with concern for malignancy on imaging or evidence of hormone excess may benefit from adrenalectomy. Benign, non-functional adrenal cysts, in contrast, can be managed with observation. Initially asymptomatic cysts may grow over time leading to symptoms of mass effect, however. 2 For example, a review by Dogra et al of 92 benign adrenal cysts found a median size of 4.8 cm (range 0.4-20 cm) and a median growth rate of 0.2 cm/year. 14 When benign cysts display rapid growth or become symptomatic, surgical resection can be beneficial for symptom relief.
Conclusions
Adrenal cysts are a rare finding with significant diagnostic ambiguity, as illustrated by this case in which we present a patient with a large, heterogenous adrenal mass and mild autonomous cortisol secretion. Despite initial concern for ACC, the patient was ultimately found to have a benign pseudocyst. Interestingly, in our case this lesion was highly concerning for an adrenocortical carcinoma and was not read as cystic on either CT or MRI. All solid, partially cystic or cystic adrenal masses require imaging characterization and biochemical evaluation to assess for hormonal activity. All tumors with malignant potential or hormonal activity should generally be resected when feasible. While there is no consensus on the treatment of asymptomatic simple adrenal cysts, they are generally managed conservatively as they have little to no malignant potential. For asymptomatic benign cysts with rapid growth or compressive symptoms, surgical intervention can be considered for symptom relief.
Footnotes
Ethical Considerations
This case report did not require IRB approval.
Consent to Participate
We personally obtained informed consent from the subject of this case report with written consent documented within the electronic health record.
Consent for Publication
As stated above, the subject of this case report has consented to publication of all anonymized patient images and data.
Author Contributions
Andrew C. Hu: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Resources; Validation; Visualization; Writing—original draft; Writing—review & editing. Jesse E. Passman: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Supervision; Validation; Visualization; Writing—original draft; Writing—review & editing. Heather Wachtel: Conceptualization; Data curation; Formal analysis; Funding acquisition; Investigation; Methodology; Project administration; Resources; Supervision; Validation; Writing—original draft; Writing—review & editing.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: HW received support from the National Institutes of Health, National Cancer Institute Grant #K08 CA270385.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
As the data in the manuscript pertain to a specific patient, additional data is not available to be shared with outside parties.