
Abstract
Background:
The most prevalent heart symptom of hyperthyroidism is atrial fibrillation. Other than sinus tachycardia, which occurs with hyperthyroidism, atrial fibrillation is the most prevalent cardiac arrhythmia. Hyperthyroidism results in excess mortality from increased incidence of circulatory diseases and dysrhythmias. The aims of the study was prevalence and associated factors of atrial fibrillation among hyperthyroidism adult patients attending the University of Gondar Referral Hospital, Northwest Ethiopia
Objective:
This study aimed to determine the prevalence and associated factors of atrial fibrillation among adult hyperthyroid patients attending the University Of Gondar Referral Hospital, Ethiopia.
Methods:
Using a consecutive sampling technique, 228 patients with hyperthyroidism participated in an institution-based cross-sectional study. A standardized questionnaire that had been pretested was used to gather the data that was designed to include socio-demographic data, clinical presentation, biochemical profile, and electrocardiography findings through chart review and interviews. The data were manually curated
Result:
Atrial fibrillation was present in 32 (14%) patients, with a 95% CI of 9.6 to 19.2. The identified predictor variables were age >61 years (Adjusted Odd Ratio = 4.2, 95% CI = 1.5-11.7), female sex (Adjusted Odd Ratio = 4.0, 95% CI = 1.4-12.0), and high serum FT4 >23.9 pmol/l (Adjusted Odd Ratio = 8.0, 95% CI = 2.1-30.0).
Conclusion:
The prevalence of atrial fibrillation among hyperthyroidism patients was 14%. Being female, being older, and having high serum FT4 levels were significantly associated with AF in hyperthyroid patients.
Plain Language Summary
The aim of this study determines the prevalence and associated factors of atrial fibrillation among adult hyperthyroid patients attending the University Of Gondar Referral Hospital, Ethiopia. Hyperthyroidism results in excess mortality from increased incidence of circulatory diseases and dysrhythmias such as AF. Atrial fibrillation (AF) is the most common cardiac condition associated with hyperthyroidism. The information that obtained from this research is intended to help health care decision makers, patients and clinicians, among others make well informed decisions by developing clear guideline and thereby improve the quality of health care services toward the overall treatment plans of AF in hyperthyroidism patients. A consecutive sampling technique was used to conduct a cross-sectional study on 228 hyperthyroidism patients. The prevalence of atrial fibrillation among hyperthyroidism patients was 14%. Being female, being older, and having high serum FT4 levels were significantly associated with AF in hyperthyroid patients. This study demonstrates a substantial relationship between atrial fibrillation in hyperthyroidism and age, gender, and high serum FT4. The physiology behind this interaction will improve our knowledge of hyperthyroidism’s impact on cardiovascular health. It would be clinically relevant to conduct additional research on the prognostic implications of atrial fibrillation in hyperthyroidism.
Introduction
Background
Elevated serum thyroid hormone levels, or hyperthyroidism, are caused by increased thyroid gland synthesis and secretion. 1 Thyroid hormones are synthesized in the thyroid gland via multiple steps and are controlled by the thyroid, pituitary, and hypothalamus axis. Thyroid stimulating hormone (TSH) is stimulated by the hypothalamus’ production of thyrotropin releasing hormone (TRH) synthesis by the anterior pituitary gland, which in turn stimulates the production of thyroid hormones. Eighty percent are thyroxine (T4), and the remaining 20% are triiodothyronine (T3). Most T3s are from the peripheral conversion of T4. These hormones are also important for in utero development and metabolic homeostasis in adults. Hyperthyroidism can be overt or subclinical. Overt hyperthyroidism is characterized by high T3 and T4 and low or undetectable TSH. Subclinical hyperthyroidism, on the other hand, is distinguished by low or undetectable TSH but generally ranges from T3 to T4. Hyperthyroidism is caused by Grave’s disease, toxic multinodular goiter, toxic adenoma, TSH-secreting pituitary adenoma, functioning thyroid cancer, Struma ovary, etc.2,3
Thyroid hormones affect every organ system; especially, the heart reacts to even the smallest variations in the quantity of blood thyroid hormone. Atrioventricular fibrillation, nonspecific ST-T alterations, ventricular hypertrophy, and dilated cardiomyopathy are a few cardiac problems associated with thyrotoxicosis. Aside from sinus tachycardia, atrial fibrillation is the most prevalent cardiac arrhythmia that people with hyperthyroidism experience. Atrial fibrillation is a cardiac arrhythmia characterized by seemingly disorganized, rapid, and irregular atrial electrical activation, resulting in the loss of organized atrial mechanical contraction. 4
Increased heart rate, systolic hypertension, increased ventricular contractility, and cardiac hypertrophy are the results of thyroid hormones’ upregulation of sarcoplasmic calcium ATPase, myosin heavy chain alpha, voltage-gated K+ channels, Na+ channels, and beta1 adrenergic receptors. 5 Patients with hyperthyroidism experience dysrhythmias, particularly atrial fibrillation, due to changes in the electrophysiological characteristics of the atria. 6 Thyroid hormones also decrease peripheral vascular resistance and increase tissue oxygen demand, which increases cardiac workload. 7
The most frequent heart disorder linked to hyperthyroidism is atrial fibrillation (AF), which is thought to affect 28% of those who have overt hyperthyroidism. 8
An increased incidence of atrial fibrillation has been linked to subclinical hyperthyroidism in the past, however these studies were all conducted in relatively small cohorts or with pooled data from multiple small cohorts. 9
Patients’ quality of life is greatly impacted by AF, which doubles the chance of death in hyperthyroidism patients compared to those without AF. Growing older, being a man, having high blood pressure, having diabetes, having a myocardial infarction, and having congestive heart failure are the main risk factors for AF.10,11
In underdeveloped nations like Ethiopia, there is a noticeable lack of data despite the abundance of information in high-income environments. Inadequate laboratory testing and subpar patient care practices are major causes of undiagnosed cases. Furthermore, the absence of viable therapeutic options leads to a rise in problems..
Early diagnosis and the immediate initiation of appropriate treatment are needed to decrease cardiovascular and cerebrovascular events. The aim of the finding was to determine the magnitude and associated factors of atrial fibrillation among hyperthyroidism patients at the University of Gondar Compressive Specialist Hospital.
Methods
Study area and period
The research was carried out between July 2023 and January 2024. The Gondar Comprehensive Specialized Hospital is situated 750 km (km) northwest of Addis Ababa, the capital of Ethiopia, in the Central Gondar administrative zone. The 2018 population forecast put the number of people living in Gondor town at 351 350 (178 447 men and 172 903 women).
An institution-based cross-sectional study was conducted at UOGCSH. All patients who were diagnosed with hyperthyroidism, attended UOGCSH and fulfilled the inclusion criteria for July 2023–January 2024 were included in the study population. All patients above 18 years of age with newly diagnosed hyperthyroidism or who had follow-up, hyperthyroid patients with a documented AF diagnosis by a clinician, and patients with uncontrolled hyperthyroidism for the past 3 months were incorporated into the research. Individuals who have permanent pacemaker implants or incomplete medical records were excluded.
Sample size determination
For sample size determination, a single population formula was used, considering the overall prevalence of atrial fibrillation in one study at Ayder Comprehensive Specialized Hospital, Tigrai, Northern Ethiopia, which was 28.9%. 8


Where
n = minimum sample size for a statistically significant survey
z = normal deviant at apportion of 95% confidence and, which is 1.96
d = marginal error taken as 5%
p = expected proportion of the population with of thyro-cardiac disease in Hyperthyroidism in similar study is 28.9%
q = 1 − p
With this formula sample size was 322.
Sample size for the second objective

So after the comparison of both objectives particularly the first objective has large sample size.
Correction of sample size was required, giving the population size was <10 000 and corrected with following formula

n = Final sample size
n0 = Initial sample size
N = Source population size
Based on the above procedure the sample size was 207 and 10% non-respondent rate was add giving final sample size of 228.
Sampling technique
Study participants were selected using a consecutive sampling technique. All patients with hyperthyroidism who fulfilled the eligibility requirements and had either had a recent diagnosis or had a follow-up examination at the University of Gondor Comprehensive Hospital throughout the research period were included.
Study variables
The study outcome variables were atrial fibrillation (AF) and socio-demographic characteristics (age, sex, occupation, income, educational status, and residence). Traditional risk factors (hypertension, DM, smoking, alcohol consumption, dyslipidemia, obesity, etc.) were also included. Pattern of clinical presentation, treatment (B-blockers, anticoagulants, and antithyroid agents, etc.) Laboratory and imaging characteristics (TFT, ECG, and echocardiography) were the independent variables.
Operational/standard definitions
Normal sinus rhythm
A normal P-wave, PR-interval, QRS complex, T-waves, and P-waves were observed before to each QRS complex, indicating a regular heart rate between 50 and 100 beats per minute. 13
ECG alterations
Any changes in the ECG beyond the normal sinus rhythm based on Minnesota coding criteria. 14
Euthyroid: refers to normal level of TSH (0.45-4.5 mIU/L), FT3 (2.3-6.3 pmol/l), FT4 (10.3-19.4 pmol/l). 1
Subclinical Hyperthyroidism: low serum TSH (<0.45 mIU/L), but normal level of FT3 and FT4.1,9,15,16
Overt Hyperthyroidism: If serum TSH is low (<0.45 mIU/l) and FT4 >19.4 pmol/l or FT3 >6.3 pmol/l or both.1 -3
Thyro-cardiac disease: form of HF characterized by myocardial damage secondary to excess thyroid hormone leading to electrical or structural cardiac abnormalities. 17
Highlands: In Ethiopia, regions that are higher than a 1000 m above sea level are referred to as highlands. 18
Lowlands: In Ethiopia, regions that are lower than 1000 m above sea level are referred to as lowlands. 18
Cerebrovascular events: clinical signs or history of the acute onset of a neurologic deficit of presumed vascular origin.
Nodular goiter: there is a single nodule making the extra amount of thyroid hormone and In a toxic multi-nodular goiter there is more than 1 nodule—and usually several—producing an extra amount of thyroid hormone. 3
Data collection tool and technique
The data were collected by trained BSc nurses and physicians at the UOGH follow-up clinic. The data collectors explained the study’s objectives to the participants and obtained informed written consent before data collection began. The data were collected through face-to-face interviews using pretested, semi-structured questionnaires for assessing the prevalence of AF and associated factors among hyperthyroidism patients. Socio-demographic factor, behavioral factor, and Comorbidity data were gathered, and patient medical documents were examined for information about medical disorders.
Serum levels of thyroid hormones (TSH, FT3, and FT4) were measured by an immune assay analyzer (BECKMAN COLTER) at the UOG laboratory and the Magnumi 800 at private clinics in Gondar town.
Using a typical 12-lead ECG equipment, supine resting ECGs were evaluated(Schiller AT-2 Plus, Nihon Kohlen, Tresmed Cardipia 400H) and calibrated at 1 mV for 10 mm (0.1 mV/mm) at a speed of 25 mm/s.
The recommended electrocardiography protocol was developed using the Minnesota standard manual as a guide. Internists manually assessed the ECG findings after analyzing them for recording faults. 14
The individuals with altered ECGs were directed to a cardiac clinic for additional evaluation and therapy. The client’s height (m) and weight (kg) were used to calculate their body mass index (BMI) (kg/m2).
Height was assessed for each subject, and weight was determined using a certified weighing scale (VMED, TAIWAN).
Patients without shoes should stand with their backs to the wall, their heels together, and their eyes directed ahead.
Data quality control
The goal of the study, the items on the checklist, the process for gathering data, and other ethical concerns were all covered in the 2 days of training that the data collectors received. Five percent of the entire sample size was used for the pretest of the data, and the necessary adjustments were made in response to the input received. The lead investigator constantly and regularly verified the acquired data’s completeness during the data collection period.
Data processing and statistical analysis
The data were coded, reviewed, and entered into Epi Info 7.2.6 and then exported to SPSS version 26 for analysis after the template was created. The results were described using descriptive statistics like frequency, percentage, mean, and standard deviation. The relationship between each independent variable and the dependent variable was examined using binary logistic regression analysis, and variables with P-values less than .25 were found. The identified variables were entered into a multivariable logistic regression model to identify the independent factors associated with AF. A 95% confidence interval (CI) and an associated factor with a P-value less than .05 were considered to indicate statistical significance. Model fitness was checked with the Hosmer-Show fitness test, and multi-collinearity was also checked.
Results
Socio-demographic characteristics of the participants
One hundred ninety-seven (86.4%) of the 228 hyperthyroidism patients (who had a 100% response rate) were female, 121 (53.1%) were between the ages of 41 and 60, 154 (67.5%) were married, and 181 (79.4%) lived in the highlands. The respondents’ average age ranged from 22 to 82 years old, 44.52 ± 13.39 years with a mean and a standard deviation respectively. Concerning the respondents’ level of education. 153 (67.1%) could not read or write (Table 1).
Socio-demographic characteristics of atrial fibrillation among hyperthyroidism patients attending UOGCSH from July 2023 to January 2024 (n = 228).

Abbreviation: ETB, Ethiopian Birr.
Behavioral characteristics and body habitus
Most of the respondents, 223 (97.8%), were nonsmokers, and 210 (92.1%) were non-alcohol users.
In this study, the majority (73%) of respondents had a normal BMI (Table 2).
Behavioral characteristics of atrial fibrillation among hyperthyroidism patients attending UOGCSH from July 2023 to January 2024 (n = 228).

Abbreviation: BMI, body mass index.
Pattern of hyperthyroidism of the respondents
Of the 228 hyperthyroidism patients, approximately 191 (83%) had overt hyperthyroidism. The most frequent cause of hyperthyroidism 198 (86.8%) was toxic multinodular goiter, which was followed by toxic nodular goiter 24 (10.5%) (Figure 1).

Causes of hyperthyroidism among patients attending UOGCSH from July 2023 to January 2024 (N = 228).
Clinical profiles of hyperthyroidism patients
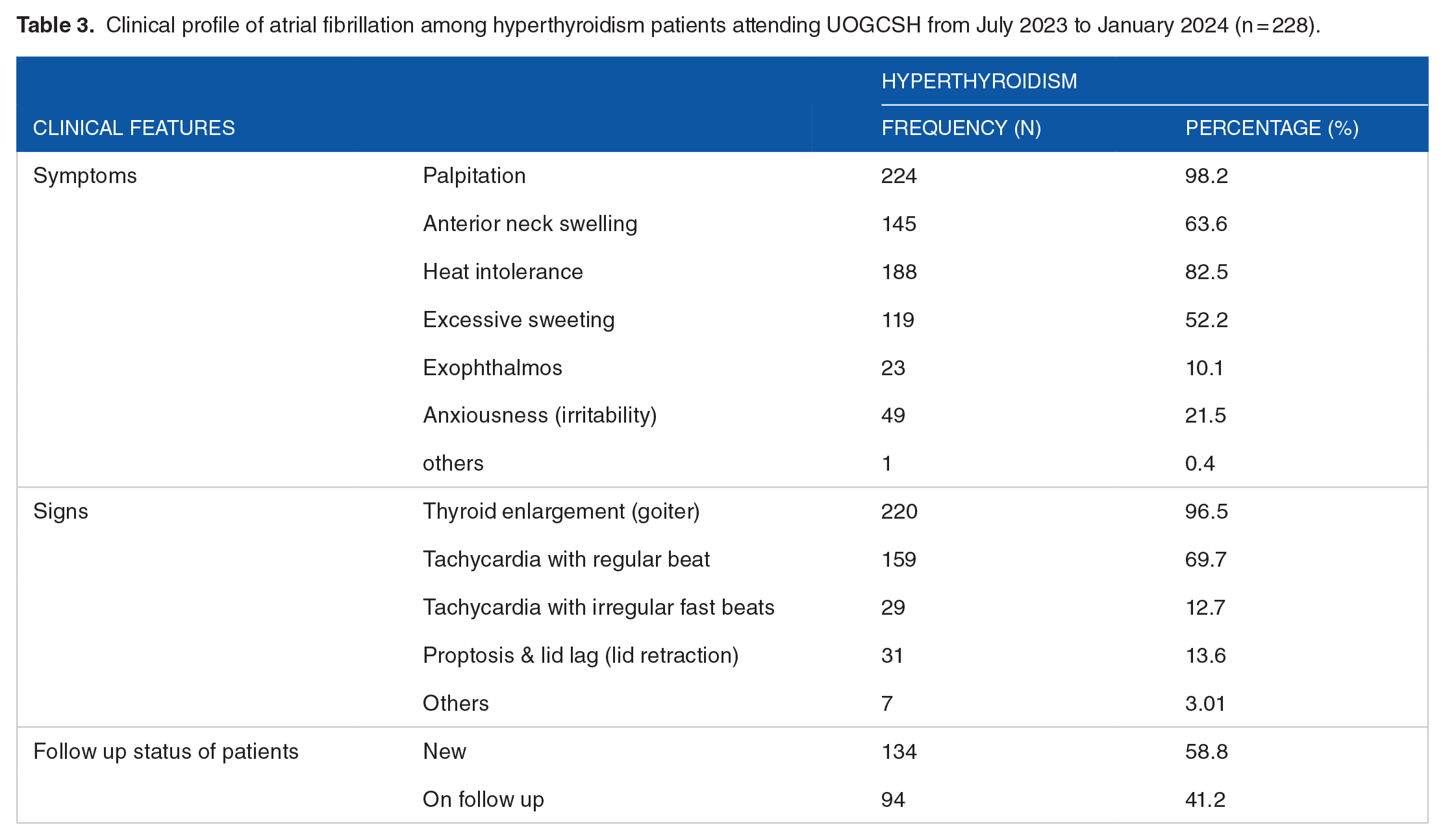
Clinical data from the medical records of the studied subjects revealed that palpitation was the most common symptom in patients with hyperthyroidism, as it was documented in 224 (98.2%) of the patients with hyperthyroidism. The next most common symptoms of hyperthyroidism were heat intolerance (188, 82.5%), anterior neck swelling (145, 63.6%), irritability (49, 21.5%) and excessive sweating (119, 52.2%) and exophthalmos (10.1%). On the other hand, regarding the clinical signs of the patients, thyroid enlargement was the most frequently documented sign (96.5%), followed by sinus tachycardia (69.7%). One patient might have more than one type of symptom or sign. The mean duration of symptom onset was 9.58 ± 8.79 months. In this study, 134 (58.8%) patients were newly diagnosed with hyperthyroidism, and 94 (41.2%) patients were followed up with hyperthyroidism.
In terms of treatment, PTU was administered as an anti-thyroid medication to every patient who underwent follow-up, and 96% of them additionally took beta-blockers.
In this study, among the total 32(14%) AF patients, 22 (68.8%) had previous AF, and 10 (31.3%) had new diagnoses patents with AF (Table 3).
Clinical profile of atrial fibrillation among hyperthyroidism patients attending UOGCSH from July 2023 to January 2024 (n = 228).
Comorbidities and CVA among hyperthyroid AF patients
In this study, comorbidities such as hypertension and diabetes mellitus accounted for 82 (36%) and 25 (11%) patients, respectively. Cerebrovascular accidents account for 2 (0.9%) of the total AF patients and 6 (6.3%) of the total hyperthyroidism patients.
Biochemical profiles of thyroid disorder patients
With respect to the hormonal profiles of the studied patients, the results of thyroid function tests at the time of data collection were reviewed. Accordingly, most (97.4%) of the hyperthyroidism patients had low TSH levels, and only 6 (2.6%) had slightly low TSH levels. Similarly, among all the hyperthyroidism patients, 158 (69.3%) had high T4 levels, 33 (14.5%) had low T4 levels, 24 (10.5%) had normal T4 levels, and only 13 (5.7%) had low free T4 levels. Moreover, the majority of hyperthyroidism patients had no serum-free T3 determination (76.3%) (Table 4).
Biochemical profile of hyperthyroidism patients attending UOGCSH from July 2023 to January 2024 (N = 228).

Prevalence of AF among hyperthyroidism patients
Among the total hyperthyroidism patients of 228 ECG results the internists analyzed and interpreted 32 (14%) had atrial fibrillation patients with (95% CI 9.6-19.2); consequently, 26 (11.4%) had overt hyperthyroidism, and 6 (2.6%) had subclinical hyperthyroidism. Among all the AF patients, a higher prevalence of 22 (68.5%) was observed among the female participants and was related to the age of the patients with AF (See Figure 2).

Comparison of AF detection among age group (228).
Regarding AF resulting from different causes of hyperthyroidism, approximately 27 (11.84%) patients with toxic multi-nodular goiters had AF, followed by 4 (1.8%) with toxic nodular goiter.
In terms of the magnitude of AF in relation to various causes of hyperthyroidism, approximately 27 (11.84%) patients with toxic multi-nodular goiter and 4 (1.8%) patients with toxic nodular goiter experienced AF.
ECG alterations among hyperthyroidism patients
According to the Minnesota coding standards, sinus tachycardia 131 (57.4%) was the most often seen ECG change in this investigation. followed by normal sinus rhythm and atrial fibrillation 64 (28.1%), and atrial fibrillation 32 (14%). Likewise, left ventricular hypertrophy (LVH) 32 (14%), right ventricular hypertrophy (12.3%), and left bundle branch block 10 (4.4%) were the most frequent ECG alterations observed. It is possible for a single patient to have many ECG abnormalities.
Echo findings
Approximately 22.4% of patients underwent echocardiography; of the abnormalities found, degenerative valvular heart disease accounted for 13.6%, pulmonary hypertension and LV systolic dysfunction (EF < 40%) accounted for 4.4%, ischemic heart disease accounted for 1.8%, and mild diastolic dysfunction accounted for 0.9% (Table 5).
Patterns of ECG alterations and ECHO findings among hyperthyroidism patients attending UOGCSH from July 2023 to January 2024 (n = 228).

Abbreviations: A fib, arterial fibrillation; AV block, atrioventricular; DVHD, degenerative valvar heart disease; IHD, ischemic heart disease; LBBB, lift bundle branch block; LVH, lift ventricular hypertrophy; RBBB, right bundle branch block; RVH, right ventricular hypertrophy.
Factors associated with atrial fibrillation
Accordingly, variables such as age, sex, serum FT4, location of residence, HTN, and monthly income were considered for inclusion in the bivariate logistic regression analysis model.
Finally, to control for confounding factors, multivariable analysis was used after checking the Hosmer–Lemeshow goodness of fit test (0.22). Age, sex, and serum FT4 were significantly associated with atrial fibrillation with P ⩽ 0.05.
Therefore, after adjusting for other variables, the study showed that the odds of AF were 4.2 times greater in the >61 years age group than in the <40 years age group (AOR = 4.2, 95% CI = 1.5-11.7), and the odds of AF were almost 3.6 times greater in the between 40 and 60 years age group than in the <40 years age group (AOR = 3.6, 95% CI = 1.2-11.5).
Another significant variable was sex, and the odds of AF were four times greater in females than in males (AOR = 4.0, 95% CI 1.4-12.0).
The odds of atrial fibrillation were 8 times greater in those with very high serum FT4 levels (>23.9 pmol/l) than in those with low serum FT4 levels (<10.3 pmol/l) (AOR = 8.0, 95% CI 2.1-30.0) (Table 6).
Bivariate and multivariable logistic regression analyses of factors associated with AF among hyperthyroidism patients attending UOGCSH from July 2023 to January 2024 (n = 228).

Statistically significant at the P-value ⩽ .05, 1 = Reference.
Discussion
As far as we are aware, this study is the first to evaluate the frequency of factors linked to AF among hyperthyroidism patients in a population. In this study, AF was confirmed in 32 (14%) patients with a 95% CI (9.6-19.2) using 12-lead ECG. This finding was consistent with the findings of studies performed in Austria and India, which reported atrial fibrillation in 13.8% of Auer et al. 9 and 15%, 19 respectively. However, this magnitude is slightly lower than that reported in other studies (24%, 20 25%, 17 and 28.9%, 21 respectively). This might be explained by 2 reasons: one is that occasional screening can miss cases of paroxysmal AF, as shown in the stroke stop study, where AF diagnosis increased 0.5% from initial electrocardiographic screening to 3.0% (95% CI, 2.7-3.5) during 2 weeks of twice-daily electrocardiographic recording. 22
Second, there were differences in the methodology used; we included patients who were followed up and who might have spontaneously reverted AF to SR after the initiation of therapy, and there were no documented baseline electrocardiographic studies. However, the other studies included only treatment-naïve patients. Nevertheless, these percentages are higher than those reported in studies performed in England, Denmark, and China, which were 7.3%, 23 8.3%, 12 and 11%, 24 respectively. Geographical disparities may be the cause of these variations; goiter prevalence ranges from 35% to 70% in Ethiopia, which has the highest rate of iodine shortage, 8 which makes people more likely to experience thyroid issues, which increase the risk of heart problems and changes in lifestyle.
The current finding revealed that the most common cause of hyperthyroidism was TMNG (86.8%), followed by TNG (24; 10.4%) and GD (1.3%), which is consistent with the findings of 2 studies.8,21 Patients with TMNG have greater AF than patients with toxic nodules or Graves’ disease, which is consistent with the findings of a study performed in Turkey. 25
The present study revealed different signs and symptoms among patients with hyperthyroidism in our hospital. Among these, heat intolerance, irregular pulse, palpitation, cold intolerance, and tachycardia are most common. This finding was also in agreement with other studies that reported the presence of these signs and symptoms among patients with endocrine disorders.8,20,23,24
The type of hyperthyroidism was classified as subclinical hyperthyroidism or overt hyperthyroidism based on the results of the TFTs and clinical decisions. The prevalence of subclinical hyperthyroidism was 16.2% in the current study, which is consistent with the magnitude of subclinical hyperthyroidism reported in a study by Jimma Medical Center (17.6%). 26 The observed magnitude of hyperthyroidism was more than 4 times (83%) greater than that in a study performed at Brazzaville Teaching Hospital, which reported a prevalence of 20.8%. 27 The observed difference may be due to geographical location. However, the magnitude of AF in this study was 26 (11.4%) in patients with overt hyperthyroidism and 6 (2.6%) in patients with subclinical hyperthyroidism; this result is consistent with that of a study performed in Austria (13.8%) 9 involving patients with overt hyperthyroidism, even if it contradicts that of patients with subclinical hyperthyroidism (12.7%). The reason could be methodology and geographical differences.
The investigator identified age, sex, and higher serum FT4 as independent predictors of risk factors associated with AF. Hyperthyroidism patients in the >61 years age group had a 4.2 times greater chance of experiencing atrial fibrillation than did those aged less than 40 years (AOR = 4.2, 95% CI = 1.5-11.7), and age range between 41 and 60 years had a 3.6 times higher risk of developing atrial fibrillation than did those aged less than 40 years (AOR = 3.6, 95% CI = 1.2-11.5).
This result in line with Framingham and other epidemiological studies.28,29 It may be the aging process’s structural, metabolic, and electrical alterations may be the source of the elderly subjects’ altered cardiac thoracic increased range of motion as well as an imbalance in sympathetic and parasympathetic activity. Generally speaking, the heart’s usual physiological characteristics change, leading to increased excitability, irritation, and delayed conduction.
Another variable found to be predictive of ECG alterations in the current investigation was sex, Compared to male patients, female patients had over 4 times higher risks of atrial fibrillation (AOR = 4.0; 95% CI: 1.4-12.0). According to a study performed in Denmark, the risk of AF hyperthyroidism in men is up to 2 times greater than that in women. 12 The investigator needs to challenge this assumption. Compared with men, Estrogen may play a major role in the susceptibility to ventricular arrhythmias by changing cardiac ion channels and transporters, which in turn alters cardiac contractility and repolarization. Women also appear to have longer QTc intervals and faster resting heart rates, which appear to evolve after puberty.30,31
The other predictor variable for atrial fibrillation was serum FT4. The odds of AF were 8 times greater in patients with serum FT4 levels > 23.9 pmol/l than in those with FT4 levels < 10.3 pmol/l (AOR = 8.0; 95% CI 2.1-30.0). This finding in line with study performed in Birmingham, England, and Austria.9,23
Other cardiovascular risk factors, such as hypertension and diabetes, were not significantly associated, even though they were positively correlated. The reason could be that most of our patient population was not from an endocrine follow-up clinic.
According to this study, of the AF patients who were followed up, approximately 22 (68.8%) had AF, and 10 (31.3%) had new patents. This result contradicts that of a study performed in China, which revealed that 54% of AF patients experienced spontaneous or pharmacological sinus conversion. The explanations could be that in patients with hyperthyroidism, atrial fibrillation (AF) persists unless euthyroidism is attained and that AF recurrence is also likely to occur (50).
PTU was the only thionamide that was utilized to treat thyrotoxicosis in terms of the kind of medication that they took. This result is comparable to one from a research that was conducted in Mekele, Ethiopia, and in which nearly every patient had PTU. 8 This result conflicts with an American Thyroid Association (ATA) survey that found methimazole to be the most often used medication (83.5%) and PTU to be used infrequently (2.7%). 1 Because of methimazole’s high rate of free T4 normalization and low incidence of side effects, its use has shifted throughout the developed world.
Strengths and limitations of the study
This is the first study to assess the magnitude and factors associated with atrial fibrillation in Gondar and Ethiopia. With limited resources, the study addressed this objective. The study was a facility-based cross-sectional study conducted only at UOGSCH. Because the socio-demographic makeup of the research population can vary and there may be differences in the availability of laboratory facilities and health care coverage, the findings may not accurately reflect the situation in other parts of Ethiopia.
In high-risk individuals, a single point of AF screening may miss paroxysmal AF, and once the patient reaches a euthyroid condition, it’s possible that they won’t be checked on to see if the AF has resolved.
Due to financial constraints, biochemical tests, including serum electrolytes and lipid profiles, as well as an echocardiogram, were not carried out.
Conclusion recommendation
This study revealed that the prevalence of atrial fibrillation among hyperthyroidism patients was 14%, which was second only to sinus tachycardia. Being female, being older, and having a higher serum FT4 level were significantly associated with atrial fibrillation in patients with hyperthyroidism. This study demonstrated a substantial relationship between AF in hyperthyroidism patients and age, sex, and high serum FT4 levels.
Our understanding of the impact of hyperthyroidism on cardiovascular morbidity and mortality will increase with more research on the physiology underpinning this relationship.
It would be clinically relevant to conduct additional research on the prognostic implications of AF in hyperthyroidism patients.
Footnotes
Acknowledgements
We would like to thank the University of Gondar College of Medicine and Health Science Internal Medicine Department for giving me the chance to conduct this research. My sincere gratitude would also go to all my families and friends who were willing to give constructive comments and support in any kind.