
Abstract
Atrial fibrillation is a frequently detected cardiac arrhythmia in the etiology of ischemic stroke. The incidence of atrial fibrillation and the risk of it causing ischemic stroke increase significantly with age; it is rare in young people. It is known that the risk of developing atrial fibrillation is high when there is a background of hyperthyroidism. COVID-19 is thought to cause thromboembolic events, cardiac pathologies, and endocrine disorders. A 54-year-old presented with right-sided hemiplegia and motor aphasia of 1.5 h duration. On evaluation, he tested positive for SARS-CoV-2 imaging was suggestive of acute pons ischemia and found to have hyperthyroidism and atrial fibrillation. It is clear that atrial fibrillation, which is highly unlikely to cause ischemic stroke in young adults, may develop due to hyperthyroidism. COVID-19 has been suggested as a cause of atrial fibrillation and hyperthyroidism. It is also thought to be involved in the etiology of stroke by causing hypercoagulation or triggering vasoconstriction through the renin–angiotensin system.
Introduction
Atrial fibrillation (AF) is an important risk factor for stroke. AF leads to a five-fold increase in the risk of stroke and AF is responsible for approximately 25% of strokes in older adults. The prevalence of AF increases dramatically with age; AF is present in 0.5% of the population under the age of 40 years, and in over 10% of those in their eighth decade of life. In the European Society of Cardiology (ESC) guidelines, the “CHA2DS2VASc Score” is recommended for predicting the risk of developing embolism due to AF. In this classification, in the absence of other risk factors, the risk of stroke due to AF in patients under 65 is considered low enough not to be included in the scoring. 1
AF is a common cardiac manifestation of hyperthyroidism. In hyperthyroidism, the risk of developing AF increases with the presence of the following factors: male gender, older age, ischemic heart disease, congestive heart failure, and valvular heart disease. 2
COVID-19 has been associated with neurological symptoms and complications, including stroke. Furthermore, theories have been developed that associate hypercoagulation with COVID-19, a “sepsis-induced coagulopathy” that may predispose the patient to ischemia. 3 In addition to stroke cases developing during COVID-19 treatment, it has been observed that the number of cases diagnosed with COVID-19 after presenting with stroke clinic is increasing. 4 The case series in which COVID-19 coexists with stroke in patients under the age of 50 years (considered as young stroke) is also remarkable. 5
Case report
A 45-year-old male patient was evaluated in the emergency room with a complaint of right-sided weakness, which was noticed when he awoke 1.5 h before. He was last seen as healthy 3.5 h before. There was no history of systemic disease. He was normotensive (110/70 mm Hg), normoglycemic (95 mg/dL), had tachycardia (137 per minute), and body mass index was 22.49 kg/m2. He was conscious, and his cooperation was limited due to motor aphasia. In his eyes, there was a forced right deviation in the primary position and left lateral gaze paralysis. Right hemiplegia and right extensor plantar reflex were present. AF was detected using electrocardiography (ECG). Diffusion magnetic resonance imaging (MRI) showed an acute infarction in the left half of the pons (Figure 1(a) and (b)). Brain computed tomography (CT) and laboratory test results were normal (Table 1). Intravenous thrombolytic therapy (alteplase) was initiated. There was no change in the patient’s neurological examination findings. Low molecular weight heparin (LMWH) was administered, and hemorrhage was not detected during the 24th hour control CT. In the examinations, low thyroid-stimulating hormone (TSH <0.01 mU/L), high free T4 (77.7 ng/L), and free T3 (24.7 ng/L) levels were detected. Antibodies against thyroid peroxidase (anti-TPO; 102 U/mL) were detected, and the anti-thyroglobulin antibody level was within normal limits. With the diagnosis of hyperthyroidism, methimazole and propranolol were added to the treatment regimen. The patient developed diarrhea on the second day of hospitalization and a day later fever, and respiratory distress was occurred. He was referred to the pandemic hospital after his chest CT (Figure 2) was found to be compatible with COVID-19, and the polymerase chain reaction (PCR) test result was positive for SARS-CoV-2. The patient was treated with high flow oxygen, antiviral agent (favipiravir), and convalescent plasma. On the fifth day, he had respiratory failure requiring tracheal intubation and mechanical ventilation. He passed away on the ninth day of clinical findings as a result of multiorgan failure.
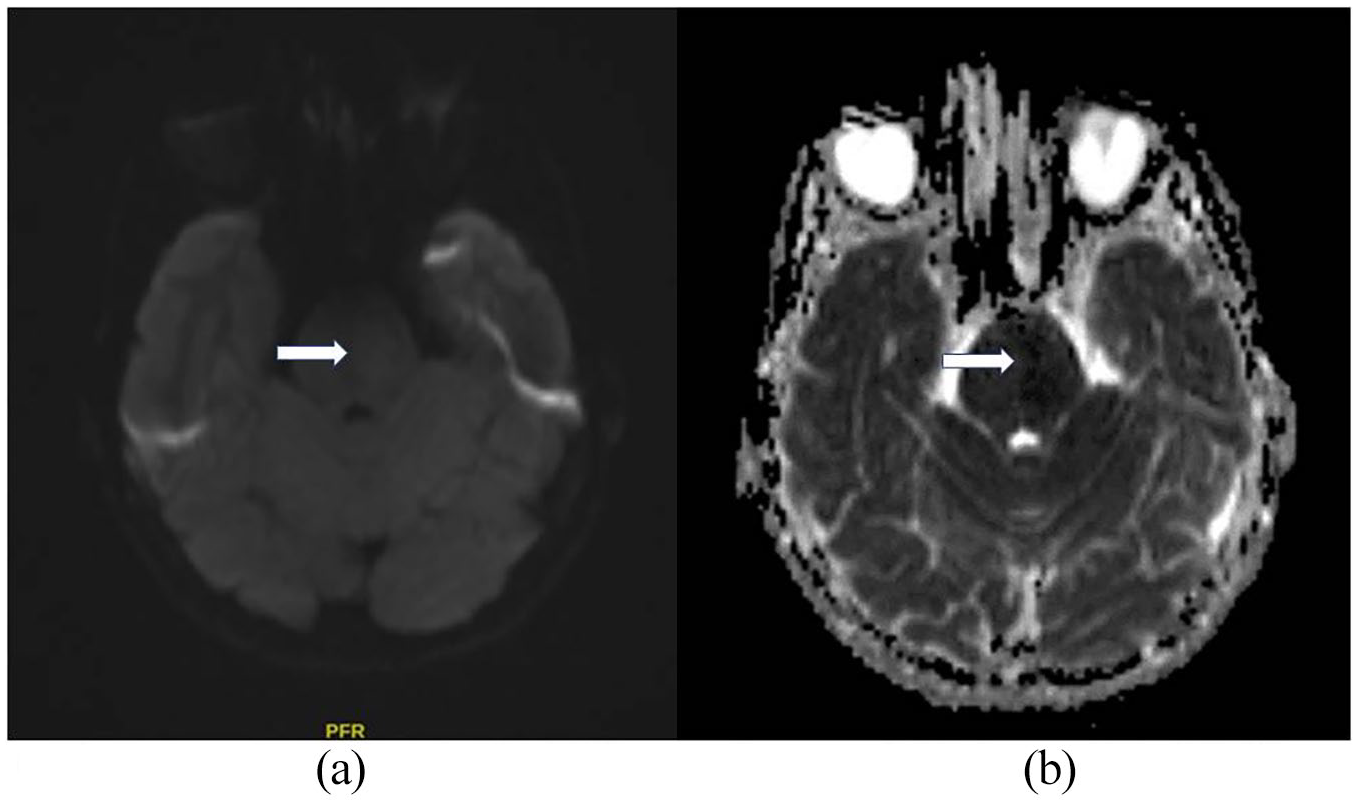
(a) Diffusion magnetic resonance imaging (MRI). (b) Apparent diffusion coefficient (ADC).
Laboratory results.
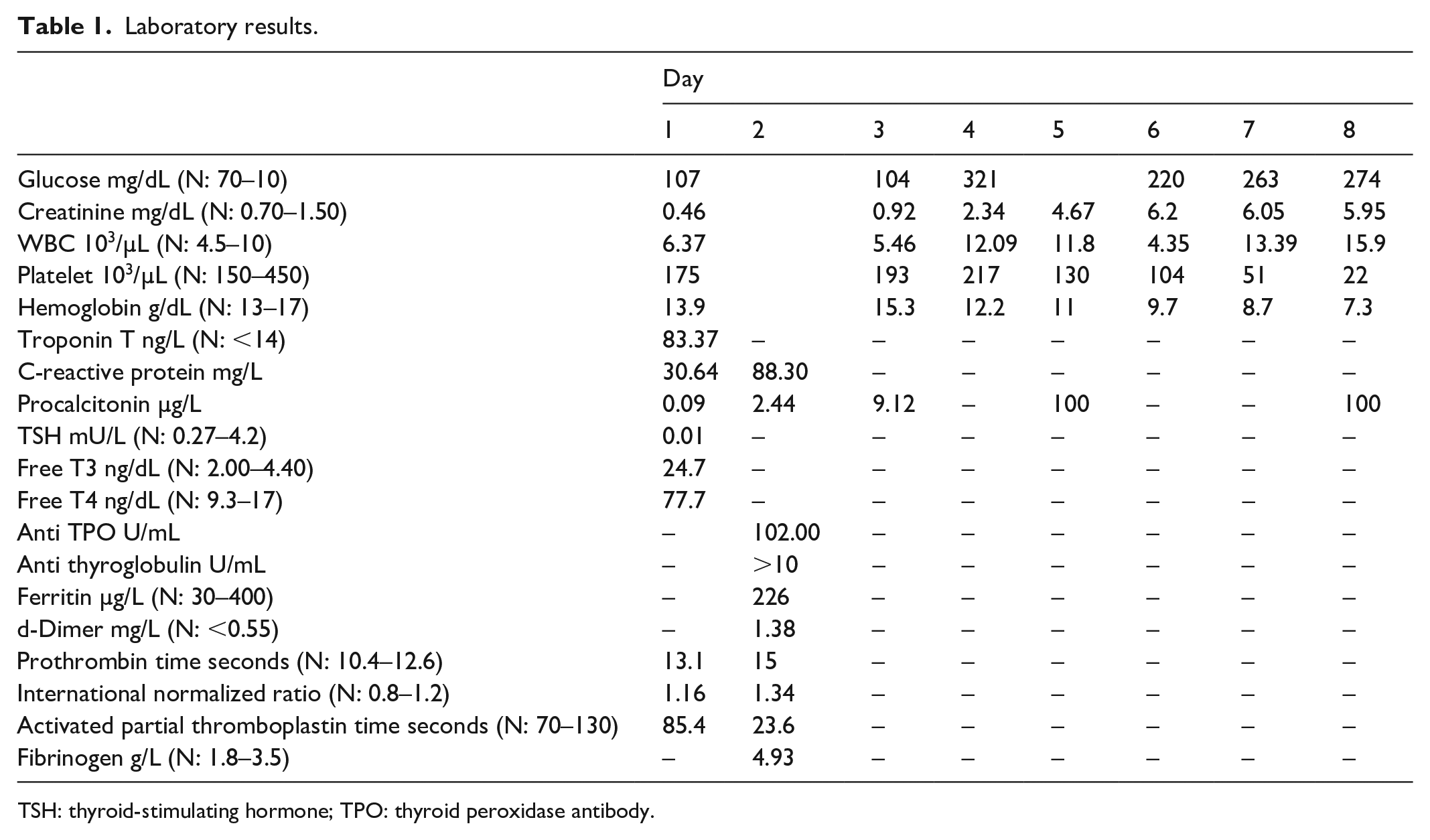
TSH: thyroid-stimulating hormone; TPO: thyroid peroxidase antibody.

Thorax CT.
Discussion
AF is one of the best-known risk factors for ischemic stroke. Like the prevalence of AF in the community, the risk of developing stroke in the presence of AF increases exponentially with age. Very rarely is AF a cause of ischemic stroke in young people. 1
The risk of developing AF on the basis of hyperthyroidism also increases with age. A study that evaluated patients diagnosed with hyperthyroidism over a 20-year period found that 3362 of 40,628 patients were diagnosed with AF or flutter; AF was detected in less than 1% of patients under the age of 40 years, and in 10%–20% of patients over 60 years old. 2
COVID-19 is thought to be responsible for cardiac pathologies, such as acute coronary syndromes, myocarditis, cardiomyopathies, cardiogenic shock, fatal arrhythmias, and sudden cardiac death. The presence of AF has been associated with COVID-19 in two COVID-19 patients, aged 46 6 and 17 7 years old.
In a study in which patients with COVID-19 were evaluated using thyroid function tests, it was found that 20% of the patients had thyrotoxicosis, and that the occurrence was inversely proportional to increasing age. The findings were interpreted as COVID-19 patients having a higher risk of thyrotoxicosis than the general population. 8
COVID-19 presents with a variety of neurological symptoms and has been associated with many neurological complications, including stroke, although its pathogenesis is unclear. Various hypotheses have been put forward regarding pathogenesis. Hypercoagulation observed in COVID-19 may be the cause of stroke associated with infection. High D-dimer levels and high fibrinogen levels, which are parameters that reveal the severity of COVID-19, indicate “sepsis-induced coagulopathy” (SIC). The systemic inflammatory response induced by infection results in endothelial dysfunction and microthrombosis, leading to organ damage. Another hypothesis emphasizes the high affinity of the SARS-CoV-2 virus to angiotensin-converting enzyme 2 (ACE2), which is found in endothelial brain and smooth muscle cells. ACE2 is an essential part of the renin–angiotensin system (RAS), and its activity opposes that of angiotensin converting enzyme 1 (ACE1) and angiotensin II. Angiotensin II has proinflammatory and vasoconstrictive effects, increasing organ damage. Binding of ACE2 by SARS-CoV-2 can alter the balance in favor of the “harmful” ACE1/angiotensin II axis and increase tissue damage, including stroke. 9
COVID-19 is also thought to have various neurological effects during its prodromal period. For example, persistent headache has been reported as a prodromal symptom of COVID-19. 10 It is thought that our patient also developed acute stroke during the prodromal period of COVID-19.
Conclusion
Both COVID-19 and AF are thought to play roles in the development of stroke. It is not clear which one played the major role in the development of stroke in this patient. However, it has been concluded that the patient developed AF on the basis of hyperthyroidism, and that the intervening COVID-19 infection triggered the development of AF-related stroke. More data are needed to interpret the association of COVID-19 with hyperthyroidism, AF, and stroke.
Footnotes
Author contributions
All the authors contributed to the study design, data collection and analysis, and writing of the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient and his wife for their anonymized information to be published in this article.