
Abstract
Background:
Matrix Gla protein (MGP) is a robust innate suppressor of the detrimental process of vascular calcification in the human body.
Objectives:
The interrelationship between circulating MGP levels and renal and cardiac dysfunction, besides echocardiographic calcification score (ECS) was investigated in a sample of type 2 diabetes (T2D) patients.
Methods:
The study included 130 subjects. They were 95 patients with T2D and 35 age- and sex-matched healthy controls. Patients were further subdivided into 52 T2D patients without DKD (eGFR ⩾ 60 ml/minute/1.73 m²) and 43 T2D persons with DKD (eGFR > 60 ml/minute/1.73 m²). Serum MGP levels, determined by ELISA, renal function tests, lipid profile, and echocardiography were studied in all participants.
Results:
Significantly elevated circulating inactive MGP level was noted in individuals having T2D compared to controls. It correlated negatively with eGFR and left ventricular (LV) diastolic and systolic functions and positively with indices of LV hypertrophy. ECS was significantly increased in both T2D groups compared to controls and in DKD group compared to the diabetic group without DKD. A significant positive correlation was observed between inactive MGP and ECS.
Conclusion:
Serum inactive MGP may contribute to the development of DKD and to the associated process of cardiac valvular calcification. It may be a beneficial diagnostic marker for early prediction of cardiac calcification and preclinical LV systolic and diastolic dysfunction in T2D patients, especially in those complicated with DKD.
Keywords
Introduction
Type 2 diabetes (T2D) is a widespread chronic medical condition with escalating prevalence rates approaching a global pandemic. The most important complications of chronic hyperglycemia in diabetic patients include cardiovascular disease (CVD) and chronic kidney disease (CKD), which constitute the leading causes of morbidity, mortality, and outstanding healthcare expenditure. 1
Diabetic kidney disease (DKD) constitutes a considerable burden, consequently leading to end-stage renal disease (ESRD). Patients with CKD exhibit a pronounced risk for cardiovascular events and CVD is incriminated in more than 50% of all deaths in those patients. Patients in early stages of CKD are expected to experience a fatal CV event more likely than go through hemodialysis (HD) due to ESRD.2,3 Nonetheless, a history of CVD is expected to pose a 29% higher risk for decline in kidney function in CKD patients. Evidently, CVD and CKD are 2 tightly interconnected morbidities. Common pathogenetic mechanisms encompass endothelial dysfunction, arterial calcification, and stiffness, which contribute to CVD, as well as to progression of CKD.4,5
Calcification of the vascular tree and heart valves has evolved as a relevant and independent risk anticipator for CVD. Matrix Gla protein (MGP) is believed to constitute a robust natural inhibitor of the detrimental process of vascular calcification in the human body. MGP was also found to revert the vascular calcification that has already taken place. 6
MGP is a protein that is related to the vitamin K-dependent proteins. It is composed of 84 amino acids. Cells secreting MGP include chondrocytes and vascular smooth muscle cells (VSMC). Besides being expressed in bone cells, MGP was also found to be expressed in other diverse tissues including adipocytes, kidney, lung, heart, cartilage, and VSMCs that are present in the media layer of the arteries. It includes 5 γ-carboxyglutamic acid (Gla) residues that require vitamin K for its activation. 7
T2D was shown to induce atherosclerosis development or further accelerate its progression. T2D was also implicated in the process of vascular and ectopic calcification, ultimately leading to cardiovascular disease. 8 Studies that describe the associations between serum inactive MGP and both kidney and cardiac dysfunction in T2D patients are still lacking. The current research investigated the relation between circulating inactive MGP level and renal and cardiac function as well as echocardiographic calcification score (ECS) in patients having T2D with and without DKD.
Subjects and Methods
The present case control research comprised a total of 130 subjects, divided into 95 patients with T2D and 35 age- and sex-matched healthy controls. T2D patients were further subdivided into 52 T2D patients without DKD (eGFR ⩾ 60 ml/minute/1.73 m²) and 43 T2D persons with DKD (eGFR > 60 ml/minute/1.73 m²). Patients were selected from the outpatient clinics of the department of Endocrinology and Metabolism at Al-Zahraa University Hospital during the period from August 2021 to January 2022. They willingly agreed to participate in the study and verbal and written consents were taken.
Inclusion criteria included patients having T2D with and without DKD based on their eGFR. The control group included apparently healthy non-diabetic subjects age and sex matched with the patients.
Exclusion criteria included an age of <18 or ⩾65 years, patients with type 1 diabetes, non-diabetic kidney diseases, renal transplantation, or dialysis therapy, history or clinical evidence of heart failure, acute ischemic heart diseases, acute cardiovascular events, previous myocardial infarction, cerebrovascular events, valvular heart diseases, deficiency or treatment with vitamin K or its antagonists, anemias, and known hemoglobinopathies and acute medical conditions such as infections and cancers.
Clinical and laboratory evaluation
History reviewing and full clinical examination were applied to all participants. They included anthropometric measurements, blood pressures and vital signs assessment. Clinical evaluation for diabetic complications was performed for peripheral neuropathy using Toronto clinical scoring system (TCSS), 9 and for diabetic retinopathy by a dilated fundus examination.
All subjects had their blood drawn aseptically while fasting for laboratory investigations. Serum total cholesterol, low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), triglycerides (TG), serum urea, creatinine, calcium (Ca), and phosphorus (Ph) were measured by routine enzymatic methods. Serum parathyroid hormone (PTH) was measured by automated immunoassay using cobas e 411 analyzer. Glycated hemoglobin (HbA1c %) was measured colorimetrically from EDTA-treated blood using cation-exchange resin.
Urinary albumin and creatinine levels were measured using spot urine samples. After that, the albumin to creatinine ratio (A/C ratio), which is represented in mg albumin/g creatinine, was calculated. Estimated glomerular filtration rate (eGFR) was also calculated using chronic kidney disease Epidemiology Collaboration group (CKD-EPI) equation. 10
Serum inactive matrix Gla protein (MGP) was measured by enzyme linked immunosorbent assay (ELISA) using kits supplied by Innova Biotech Co, Beijing, China.
Echocardiography
Transthoracic echocardiography was performed at rest using a Vivid E9 XD clear ultrasound system (origin country: Norway) with an attached echoPac workstation version (201). Patients were examined in the standard positions using multi-frequency (1.5-4.6 MHz) matrix probe M5S. Image acquisition was done from all accessible windows and views. The images and cine loops were digitally stored for later offline analysis. Echocardiographic assessment was performed by a single researcher who was blinded to the patient characteristics and the mean of coefficient of variances of echocardiographic measurements was about 19.5%.
LV dimensions and functions were studied using various echocardiographic modes (including M-mode, 2-dimensional (2D) conventional Doppler flow tissue, Doppler Imaging and speckle tracking echo (STE)). Imaging and analysis were done according to recommendations of the American Society of Echocardiography guidelines 2015.
11
The following parameters were obtained: M-mode measures: Assessment of left ventricle wall thickness and cavity dimensions were done including end diastolic interventricular septal wall and posterior wall thickness (IVSd and LVPWd respectively), left end diastolic dimension (LVEDD), left ventricle end systolic dimension (LVESD), from which left ventricular percent fractional shortening (%FS) and left ventricle ejection fraction (LVEF %) were automatically calculated. Left atrial (LA) diameter and aortic root (Ao) diameter, left ventricular volumes at end diastole and end systole were obtained and LV ejection fraction (Biplane LVEF) was calculated.
LV diastolic function was assessed using conventional pulsed Doppler of mitral valve flow and tissue Doppler assessment of mitral annular velocities including peak mitral early diastolic flow velocity (MV-E vel), peak mitral late diastolic flow velocity (MV-A vel), and the ratio between the MV-E vel and MV-A vel (mv-E/A). Mitral annular early diastolic velocity (E′), measured through TDI was used to calculate an estimated value for left ventricular end diastolic pressure with calculation of mitral E/E′ ratio.
Using 2-Dimensional Speckle Tracking Echo (2D-STE), derived left ventricle global longitudinal strain (GLS) was determined as a tool for detection of early subclinical left ventricular systolic dysfunction.
Detection of valvular calcification, namely, Aortic valve calcification (AVC), Mitral annular calcification (MAC), aortic root, and papillary muscle calcification was done. Calculation of ECS was done according to the previously published study of Gaibazzi et al. 12 Each aortic valve leaflet was graded on a scale of 0 (normal) to 3 (severe) according to leaflet thickening and calcific deposits; the highest score for a given cusp was assigned as the overall degree of aortic valve sclerosis. MAC was measured from the leading anterior to the trailing posterior edge and judged on a scale of 0 (normal) to 3 (severe). Papillary muscle and aortic root calcium were assigned a grade 0 or 1 according to absence and presence of calcification. Accordingly, a final score was calculated as the sum of all identified cardiac calcific deposits in the range of 0 (no calcium visible) to 8 (extensive cardiac and aortic root calcific deposits).
Statistical analysis
Data were collected and analyzed using the statistical package for social sciences, version 23.0 (SPSS Inc., Chicago, Illinois, USA). Data were explored for normality using Shapiro-Wilk test. The quantitative data were presented as mean ± standard deviation while qualitative variables were presented as numbers and percentages.
Chi square (χ2) and 1 way analysis of variance followed by Post Hoc Tukey’s test or Kruskal Wallis test followed by Post Hoc Mann-Whitney test were performed for comparing the data. Correlations between serum inactive MGP and other parameters were assessed using Spearman’s rank correlation coefficient. Receiver operating characteristic (ROC) curves were generated for serum levels of inactive MGP as a classifier biomarker of type 2 diabetes and diabetic kidney disease based on eGFR. Finally, multiple linear regression analysis to identify significant predictors of serum inactive MGP concentration was carried out. P < .05 was considered statistically significant.
Results
Table 1 shows demographic, clinical, and laboratory characteristics of the studied groups. Inactive MGP was found to be significantly increased in both diabetic patients’ groups (without and with DKD) compared to controls (P > .001). T2D group with DKD had higher levels but not statistically significant as compared to the T2D group without DKD.
Demographic, clinical, and laboratory characteristics of the study groups.

Abbreviations: A/C ratio, albumin/creatinine ratio; BMI, body mass index; Ca, calcium; DBP, diastolic blood pressure; DKD, diabetic kidney disease; DM, diabetes mellitus; eGFR, estimated glomerular filtration rate; HbA1c, glycated Hemoglobin; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; MGP, matrix Gla protein; Ph, phosphorus; PTH, parathyroid hormone; SBP, systolic blood pressure; T2D, type 2 diabetes; TG, triglycerides; WC, waist circumference.
Data are expressed as Mean ± SD or Number (%).
Chi-square test, 1 way analysis of variance followed by post hoc Tukey’s test or Kruskal Wallis test followed by Post Hoc Mann-Whitney U test were performed.
a: P-value for the comparison between T2D without DKD and T2D with DKD.
b: P-value for the comparison between T2D without DKD and control group.
c: P-value for the comparison between T2D with DKD and control group.
: Significant at P-value <.05. **: Significant at P-value <.001.
Obesity indices (weight, BMI, and WC) were significantly higher among T2D groups compared to controls. Significantly longer diabetes duration and higher diabetic neuropathy scores were notable among the T2D group with DKD compared to those without DKD. Furthermore, DKD group had significantly higher renal function namely, blood urea, serum creatinine, A/C ratio, and significantly lower eGFR compared to both T2D group without DKD and controls (P > .001). A significant increase in glycated hemoglobin and decrease in HDL-C were also observed in both T2D groups compared to controls.
Table 2 displays the echocardiographic findings of the study participants. Significantly increased IVSd was shown in both T2D groups compared to the control group and in the group with DKD compared to the group without DKD. LVPWd and LA diameters and were significantly higher in the DKD group compared to the control group. Also, they were higher in DKD group compared to the group without DKD and in the T2D group without DKD compared to control group but with no statistical significance. These findings denote LV hypertrophy among T2D patients, a finding which was more pronounced in the group with DKD.
Echocardiographic parameters among the studied groups.

Abbreviations: 2-D STE GLS, 2-dimensional speckle tracking echocardiography global longitudinal strain; Ao, aorta; AVC, aortic valve calcification; DKD, diabetic kidney disease; Echo, echocardiography; ECS, echo calcification score.; EF, ejection fraction; FS, fraction shortening; IVSd, interventricular septal diameter; LA, left atrium; LVPWd, left ventricular posterior wall diameter; MAC, mitral annular calcification; T2D, type 2 diabetes.
Data are expressed as Mean ± SD or Number (%).
One Way analysis of variance followed by post hoc Tukey’s test or Kruskal Wallis test followed by Post Hoc Mann-Whitney U test were performed.
a: P-value for the comparison between T2D without DKD and T2D with DKD.
b: P-value for the comparison between T2D without DKD and control group.
c: P-value for the comparison between T2D with DKD and control group.
: Significant at P < .05, **: Significant at P < .001.
Moreover, significantly increased Mitral E/E′ (ratio) was observed in DKD group compared to T2D group without DKD and controls (P = .005 and <.001 respectively). This indicates markedly increased LV flow pressure in patients with DKD, which is the main parameter of LV diastolic dysfunction, denoting severe LV diastolic dysfunction in the DKD patients. Mitral E/E′ (ratio) was also found to be higher in the group without DKD compared to the control group denoting LV mild diastolic dysfunction in non DKD group. GLS was significantly lower in both T2D groups compared to the control group (P < .001) and in the DKD group compared to the group without DKD (P = .022) signifying a degree of subclinical LV systolic dysfunction in both T2D groups.
Cardiac calcification was significantly higher at level of mitral annulus, papillary muscle and aortic root in both patients’ groups in comparison to control group, but there was no significant difference between both patients’ groups. ECS was significantly higher in both T2D groups compared to controls (P < .001) and in DKD group compared to the group without DKD (P = .026).
Correlations between serum inactive MGP and all research variables are displayed in Table 3 and Figures 1 and 2. Serum inactive MGP was positively correlated with age, clinical obesity indicators (weight, BMI, and WC; P < .001), diabetes duration, renal functions (urea, creatinine, A/C ratio), and HbA1c (P < .001), while it was negatively correlated with eGFR (P < .001). Positive correlations were also observed between serum inactive MGP and total cholesterol and TG (P = .048 and .029 respectively).
Correlation between serum inactive MGP and all studied parameters among the study population.

Abbreviations: A/C ratio, albumin/ creatinine ratio; BMI, body mass index; Ca, calcium; DBP, diastolic blood pressure; DM, diabetes mellitus; ECS, Echo calcification score.; eGFR, estimated glomerular filtration rate; HbA1c, glycated Hemoglobin; HDL-C, high-density lipoprotein cholesterol; IVSd, interventricular septal diameter; LA, left atrium; LDL-C, low-density lipoprotein cholesterol; LVPWd, left ventricular posterior wall diameter; MGP, matrix Gla Protein; Ph, phosphorus; PTH, parathyroid hormone; SBP, systolic blood pressure; STE GLS, speckle tracking echocardiography global longitudinal strain; TG, triglycerides; WC, waist circumference.
Spearman’s rank correlation coefficient was performed.
: Significant at P-value <.05, **: Significant at P-value <.001.

Correlation between serum inactive MGP with biochemical characteristics of the study population: (a) serum creatinine, (b) eGFR, (c) A/C ratio, (d) HbA1c, (e) total cholesterol, and (f) Triglycerides.

Correlation between serum inactive MGP with (a) mitral E/E′, (b) GLS, and (c) ECS among the study population.
Serum inactive MGP correlated with indices of LV hypertrophy, namely, IVSd and LVPWd (P < .001 and .047 respectively). As regard the echocardiographic features that signify LV diastolic function; serum inactive MGP was found to correlate positively with mitral E/E′ and negatively with mitral E/A (P = .035 and <.001 respectively). GLS, which is a reliable measure of LV systolic function, correlated negatively with serum inactive MGP. As regard cardiac valve calcification, ECS was positively correlated with serum inactive MGP.
Linear regression analysis performed to determine predictors of serum inactive MGP concentration shows that WC, diabetes neuropathy score, and HbA1c were the most predictor factors affecting serum level of inactive MGP concentration arranged in that order (P = .002, .015, and .029, respectively), as shown in Table 4.
Multiple linear regression analysis to identify predictors of serum inactive MGP concentration.
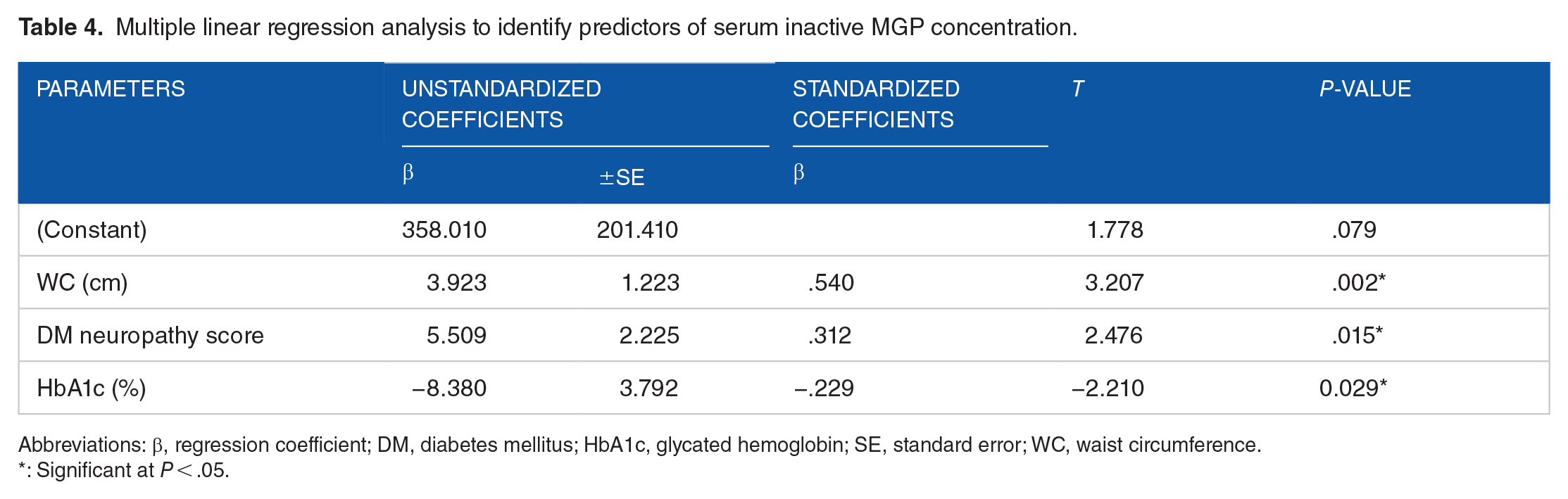
Abbreviations: β, regression coefficient; DM, diabetes mellitus; HbA1c, glycated hemoglobin; SE, standard error; WC, waist circumference.
: Significant at P < .05.
Roc analysis was performed to assess the cutoff value for serum inactive MGP to distinguish T2D patients from controls which was found to be 452.5 pg/ml. The area under the curve was 0.893 with sensitivity 95.8% and specificity 85.7%. Also, a cut-off of value for serum inactive MGP level as a predictor of decline in eGFR was found to be 532.5 pg/ml. The area under the curve was 0.704 with sensitivity 70% and specificity 61% as shown in Figure 3.

Receiver operating characteristic curve for inactive MGP as: (a) a classifier Biomarker for T2DM, the area under the curve was 0.893 with sensitivity 95.8% and specificity 85.7% and (b) a predictor for decline in eGFR, the area under the curve was 0.704 with sensitivity 70% and specificity 61%.
Discussion
Activated MGP is a robust endogenous inhibitor of ectopic and vascular calcification which is the hallmark of vascular disease and imminent cardiovascular complications. The enhanced arterial calcification, frequently noted in patients with CKD, may denote that MGP expression and function may be suboptimal in this population. Subsequently, this may aggravate the long-term ectopic and vascular calcification process. 5 The most important complications of chronic hyperglycemia include CVD and CKD. T2D is usually associated with detrimental cardiovascular adverse events, including vascular calcification, and accelerated atherosclerosis. These pathological sequelae add to the increased morbidities and life threatening cardiac events frequently encountered in patients having diabetes. 8 Studies that describe the associations between serum inactive MGP and both kidney and cardiac dysfunction in T2D patients are still lacking. Therefore, we assessed serum inactive MGP levels in a sample of patients having T2D to explore its relations with renal and cardiac functions.
Serum inactive MGP levels in T2D Patients with and without DKD
In the present study, circulating level of inactive MGP was noted to be significantly higher in both T2D groups when compared to controls (P < .001). These results underscore a possible pathogenic role for MGP in the augmented vascular calcification phenomenon, frequently encountered in individuals with diabetes.
In agreement with our results, Riphagen et al, 13 in a large general population-based cohort study, reported significantly higher serum inactive MGP in T2D patients. Furthermore, Griffin et al, 5 reported significantly higher serum inactive MGP in T2D patients compared to healthy controls. They found that MGP levels were significantly higher in the diabetic group with DKD compared to the diabetic group with normal function.
Vitamin K deficiency is considered the main factor responsible for MGP activation. Our results may thus confirm the theory that T2D and DKD are overt or subclinical vitamin K deficiency states. Accordingly, increasing dietary vitamin K and/or vitamin K supplementation may represent a promising therapeutic approach to prevent or reduce ectopic calcification in CKD.
Serum inactive MGP level and clinical characteristics
In the current work, positive correlation was noted between circulating inactive MGP and age, as well as other clinical characteristics including duration of diabetes, waist circumference (WC), systolic blood pressure (SBP), and diabetes neuropathy score. These findings signify a close relation between MGP and central obesity, and consequently insulin resistance. Significant correlation between inactive MGP and diabetes duration and diabetes neuropathy score suggest that, MGP could be associated with diabetic microvascular complications, which are more prevalent with longer diabetes duration.
In concordance with our results, Malhotra et al, 14 in a prospective longitudinal community-based observational cohort study, explored the association between inactive MGP and vascular calcification and stiffness among participants in the Framingham Heart Study. They reported that older age was associated with higher inactive MGP levels.
Adel et al, 15 assessed serum inactive MGP in a sample of Egyptian diabetic patients with and without diabetic retinopathy. Congruent to our results, they reported positive correlation between serum inactive MGP and diabetes duration. Li et al, 16 in their study on a randomly selected sample of Chinese population, reported that serum inactive MGP level was positively associated with central obesity, which was assessed by visceral fat index using body composition monitor and waist to height ratio.
Malhotra et al, 14 and Griffin et al, 5 observed that serum inactive MGP was associated with body mass index (BMI). Malhotra et al 14 and Riphagen et al 13 found that higher SBP correlated with higher inactive MGP concentrations. In accordance with our results, Jeannin et al 17 found that peripheral neuropathy score was associated with higher MGP in their cross-sectional study on T2D patients with diabetic complications.
Serum inactive MGP level and biochemical characteristics
In the present study, serum inactive MGP was found to be correlated with impaired renal function, namely, elevated serum urea and creatinine, decreased eGFR, and increased A/C ratio. Similar results were reported by several previous researchers who found an association between serum inactive MGP and deterioration of renal function in T2D.2,5,14
Wei et al, 18 in a longitudinal study, assessed the association between eGFR and plasma inactive MGP in a general population. After 8.9 years follow-up, they noted that, serum inactive MGP increased by 23%, while eGFR decreased by 4.05 ml/minute/1.73 m2.
In the current study, inactive MGP correlated positively with parathyroid hormone, while there was no significant correlation with serum calcium and phosphorus. However, different results were reported by Parker et al, 19 who observed direct correlations between inactive MGP and both serum calcium and phosphorus levels.
As regard the glycemic and lipid parameters, in the present study, it was observed that serum inactive MGP correlated positively with HbA1c, total cholesterol, and triglycerides. In concordance with our results Malhotra et al, 14 reported that higher inactive MGP concentrations were associated with hyperlipidemia. Roumeliotis et al, 2 reported positive correlation between serum inactive MGP and TG, but not with total cholesterol. Li et al, 16 reported that serum inactive MGP correlated positively with LDL-C and negatively with HDL-C.
Wei et al, 20 studied the association between inactive matrix Gla protein and retinal arteriolar narrowing in 935 randomly recruited Flemish participants. They found that hyperglycemia was associated with higher inactive MGP concentrations. Antonopoulos et al, 21 also noted a significant positive association between MGP and insulin resistance in their study on T2D patients. On the other side, Griffin et al, 5 found no significant association between serum inactive MGP and HbA1c and the lipid panel.
The association between serum inactive MGP levels and the dysmetabolic parameters observed in the present study, highlights the interrelation between serum inactive MGP levels and the altered metabolic status occurring in diabetes, including glucotoxicity, lipotoxicity, and insulin resistance. These metabolic derangements eventually lead to oxidative stress, inflammation, and mitochondrial dysfunction. All these factors may contribute to the pathogenesis of vascular calcification through induction of vascular smooth muscle cells differentiation into osteoblast.
Serum inactive MGP level and echocardiographic findings
The congruency between increased inactive MGP and increased vascular stiffness was noted and described in several research.22,23 Arterial stiffness is known to be related to higher hypertension prevalence rates, altered remodeling of the myocardial tissues, diastolic dysfunction, and heart failure. 14
In the current study, serum inactive MGP positively correlated with indices of LV hypertrophy. In accordance with our results, Malhotra et al, 14 reported that increased circulating inactive MGP concentrations were associated with increased left atrial diameter and LV relative wall thickness assessed by echocardiography.
Furthermore, in the present study, significant correlation was encountered between serum inactive MGP and parameters of LV systolic and diastolic function. It correlated negatively with Mitral E/A ratio and LV GLS and positively with mitral E/E′ ratio. Thence, we hypothesize that serum MGP may enhance LV systolic and diastolic functions and may play a role in maintaining myocardial integrity and diastolic LV performance. Hence, inactive MGP may be a potential diagnostic marker that can early predict preclinical LV systolic and diastolic dysfunction.
Similar results were reported by Wei et al, 24 who found an association between serum inactive MGP and LV diastolic dysfunction among Flemish and Swiss population cohort studies. Malhotra et al, 14 reported that among their study population, elevated inactive MGP values and worse LV GLS co-existed.
Cardiac valvular calcification in relation to inactive MGP level
MGP is the main inhibitor of ectopic calcification including vascular calcification and cardiac valve calcification through inhibition of bone morphogenetic protein-2 (BMP-2) which stimulates differentiation of the osteoblast. 25 Chronic inflammation has a crucial contribution to the pathogenesis of T2D. Thus, it is emphasized that T2D is a relevant risk factor involved in the pathogenesis of valvular calcification by promoting early mineralization of the cardiac valves. 26 Previous studies reported close relation of valvular calcification especially aortic valve calcification with coronary artery disease, and suggested that ECS could be a significant predictor for coronary artery disease and cardiac events.27,28
In the current study we found that cardiac valvular calcification at the level of mitral valve annulus, papillary muscle, and aortic root were significantly higher in T2D patients compared to control (P ˂ .001). Also, AVC was higher in both T2D patients’ groups compared to controls. However, this did not reach statistical significance. As regard the total ECS it was significantly higher in both patients’ groups compared to control group (P ˂ .001) and in T2D group with DKD compared to group without DKD (P = .026).
Previous researchers reported increased expression of markers of valvular calcification, in aortic valve tissue in T2D patients compared to nondiabetic subjects who underwent aortic valve replacement, thus suggesting higher susceptibility of T2D patients to calcific aortic stenosis.29,30
Tang et al, 31 reported increased cardiac valvular calcification assessed by echocardiography and valvular regurgitation in T2D patients with DKD compared to another diabetic group without DKD. Litovkina et al, 32 also reported increased incidence of cardiac valvular calcification assessed by echocardiography mainly MAC and AVC in DKD patients on chronic hemodialysis.
No previous studies have discussed the association between inactive MGP level and ECS. In the present study serum inactive MGP was found to be correlated positively with ECS. Brandenburg et al, 33 reported that higher serum inactive MGP was associated with AVC assessed by cardiac CT scan. Capoulade et al, 34 reported that plasma levels of the inactive form of this protein were correlated with progression of calcific aortic stenosis assessed by echocardiography. Parker et al, 19 in their study on patients with stable CVD reported that inactive MGP was associated with higher incidence of mitral annular calcification in individuals having diabetes. These Findings support the theory of higher susceptibility of T2D patients especially those with DKD for vascular calcification in general and cardiac valve calcification in particular. Our results suggest that serum inactive MGP could be an early predictor for, besides being an inducer of, cardiac valve calcification among T2D patients and patients with DKD.
Parameters predicting circulating inactive MGP concentration
In the present study, multiple linear regression analysis model showed that WC, diabetes neuropathy score, and HbA1c were the most predictor parameters affecting serum level of inactive MGP concentration arranged in that order (P = .002, .015, and .029, respectively). This signifies the close relationship between inactive MGP and visceral obesity and insulin resistance as represented by WC, as well as with the hyperglycemic load (HbA1c) and the burden of diabetic complications, namely diabetic neuropathy (neuropathy score). However, the current study plan does not allow for delineation of the causal nexus. Future prospective studies are warranted to investigate the direction of this chain of changes.
Similar results were reported by Li et al, 16 who found that inactive MGP was independently associated with central obesity. However, different results were reported by Roumeliotis et al, 2 who concluded that inactive MGP was independently associated with eGFR. Additionally, Wei et al, 24 found that MGP was independently associated with mitral E/E′.
The incongruity between the various studies might be attributed to the diverse study plans and sampling methods.
Study Strengths and Study Limitations
The present study is the first to assess cardiac calcification scores in relation to MGP in T2D with and/or without DKD. Measurement of total serum MGP was reported to provide conflicting results. 19 Measurement of inactive rather than total MGP represents a point of strength to the present study. Additional points of strength include utilization of several indices for measurement of kidney function, besides the selection of our study population who had no clinical evidence of overt CVD. Furthermore, multiple potential confounding variables were also measured, including HbA1c, lipid profile, kidney functions, serum calcium, Ph, and PTH. Limitations of the current study include the relatively small sized study population sample. Furthermore, the power analysis for sample size calculation was not done. The study participants had mild and moderate CKD, thence, our results may not be generalizable to persons with advanced stage CKD. The observational nature of the study design does not determine the cause-effect relationship between the studied variables.
Conclusions
Our findings appeal for the contribution of inactive MGP in the pathogenesis of diabetic kidney disease and ectopic cardiac calcification. The correlation between serum inactive MGP level and LV diastolic and systolic dysfunction highlights the possible role of MGP in maintaining myocardial integrity and diastolic LV performance. Accordingly, we speculate that serum inactive MGP level may be a useful diagnostic marker for early prediction of ectopic cardiac calcification as well as preclinical LV systolic and diastolic dysfunction in T2D patients, especially in those complicated with DKD. Accordingly, it may also be a promising therapeutic modality to counteract ectopic and vascular calcification that are hallmark phenomena in patients with DKD.
Footnotes
Acknowledgements
Thanks are due to the medical and paramedical working team at the Department of Endocrinology and Metabolism at Al-Zahraa University Hospital, Faculty of Medicine (Girls), Al-Azhar University, Cairo, who helped throughout the process of patient identification and sampling. Also, we acknowledge all the efforts exerted by the staff of Biochemistry and Molecular Biology Department, Faculty of Pharmacy (Boys), Al-Azhar University, Cairo, for their assistance throughout the practical work and for facilitating the use of the central lab facilities.