
Abstract
Background:
Adequate knowledge, awareness, and adherence to diabetic self-care practices are vital tools to protect patients from risks of disease complications, developing comorbidity and mortality. Therefore, this study aimed to assess specific domains of diabetic self-care practice and associated factors among patients with type-2diabetes in Hawassa University Comprehensive Specialized Hospital, Sidama regional state.
Materials and methods:
A hospital-based cross-sectional study design was conducted on 217 patients with type 2 diabetes from January 01 to April 30, 2020. A structured questionnaire and the Summary of Diabetes Self-Care Activities (SDSCA) tool were used to collect relevant data through interviewer administration. Statistical analysis was done using SPSS version 23.
Results:
A total of 207 patients with type-2 diabetes were participated in the study with a 95% response rate. Overall 47.8% (95%CI: 41.2-55) of patients adhered to diabetic self-care practice. Concerning the specific domain of self-care practice, 54.6%, 39.1%, 28%, and 65.2% of patients adhered to a healthy diet, physical exercise, self-monitoring blood glucose (SMBG), and diabetic foot care practices, respectively. Besides, all patients received at least 80% of the prescribed doses and frequency of anti-diabetic agents and 60.4% had good glycemic control. Receipt of advice from treating physicians and having no familial history of diabetes were significantly associated with adherence toward eating a healthy diet, diabetic foot care, and SMBG. While male sex was associated with adherence toward healthy diet management. Moreover, having glucometer, age, male sex, diabetes duration ⩾ 5 years, and anti-diabetic treatment modality were associated with adherence toward SMBG.
Conclusion:
This study indicates 52.2%, 72%, and 60.1% of diabetes patients did not adhere to diabetic self-care, SMBG, and physical exercise, respectively. Improving awareness and regular diabetic education is imperative to scale up patients’ adherence toward diabetic self-care practice.
Introduction
According to 2019 International Diabetes Federation (IDF) report prediction, 578 million people (10.2% of the population) will have diabetes by 2030. That number will rise to a staggering 700 million (10.9%) by 2045. 1 In addition, more than 4 million peoples were died among patients with age 20 to 79 years old in 2019 due to diabetes and its complications. 1 Regarding economic burden, the global health expenditure on diabetes was estimated to be USD 727 billion in 2017. 2 Diabetes is 1 of the highly increasing non-communicable diseases in Sub-Saharan Africa. 3 More than 21 million people have DM in Africa and it will increase two-fold by 2035 and of this more than 2.1 million diabetes patients might be expected in Ethiopia. 4 About 50% of all deaths in developing countries comprising Sub-Saharan Africa were attributed to diabetes according to the IDF report. 4 Both qualities of life and life expectancy become lowered due to DM and it predisposes a big economic burden on patients and healthcare systems directly or indirectly.5-7 In Africa, an estimated USD 2.8 billion was spent on healthcare expenditure in 2011 due to diabetes and this might be expected to rise 61% in 2030. 8 In sub-Saharan Africa, diabetes greatly increased the risks of heart attack, stroke, kidney damage, blindness, neural damage leading to amputation, and reduced life expectancy. 9 The meta-analysis that conducted in 2019 indicates the pooled prevalence of adherence toward anti-diabetic medication in Ethiopia was 69.5% (95% CI (61.1, 78.0)), while the rate was 88.2% (95% CI: 80.5, 95.9%) in South Nations and Nationalities Peoples Region (SNNPR), and 78.7% (95% CI: 68.8, 88.5) in Addis Ababa). 10 Adherence to self-care practice among diabetes patients is crucial to limit the complex nature of the disease in a social context. 11 The adherence to self-care practice of type 2 diabetes patients includes performing regular physical activity, recommended healthy diet eating, diabetic foot care, self-monitoring of blood glucose (SMBG)12,13 and medications. 14 Adherence to these self-care behaviors improves glycemic control and reduces the severity of disease complications; 15 conserves blood pressure; 16 and health care costs. 17 Factors that affect self-care practice in DM patients were sex and occupation,18,19 marital status, socioeconomic status, and educational status.18,20
Adherence to the specific domains of diabetic self-care practice of patients might vary from one health care institution to another due to patients, institutions, and health care providers’ related factors. Therefore, this study aimed to assess the magnitude and predictors of adherence to domains of diabetic self-care status among patients with type-2 diabetes.
Methods
Study setting, design, and study population
This institution based cross-sectional study was conducted from January 01 to April 30, 2020. Hawassa University Comprehensive Specialized Hospital (HUCSH) is the largest public referral as well as teaching Hospital which is found in Sidama regional state, Southern Ethiopia. Hawassa city is located 275 km from Addis Ababa, the capital city of Ethiopia. The hospital serves more than 20 million populations of Sidama regional state, Southern Nations Nationalities and Peoples Region (SNNPR), Somalia and Oromia regions. It provides the health services in major departments (Internal medicine, Surgery, Pediatrics, Gynecology and Obstetrics), Ophthalmology, Dermatology, ear neck and throat (ENT), Radiology, psychiatry, Oncology, Laboratory & Pharmacy. The department of internal medicine provides inpatient, emergency, and outpatient services. One of the outpatient services is carried out at a medical referral clinic (MRC) that includes a neurology unit, cardiology unit, gastroenterology unit, endocrinology units, and Hematology units. Diabetes clinic gives services for DM patients like therapeutic management, advice and education on diabetic self-care management. Currently over 500 registered diabetes patients regularly attending the outpatient department (OPD) of diabetic clinic in the hospital and 30 to 40 patients with diabetes visit the hospital every week. Moreover, the hospital provides payment-free healthcare services for only those who provide an official evidence letter about their economic status to be free of pay, while the rest of patients get the healthcare service with a charge of their pocket money. At the beginning of antidiabetic treatment initiation: all dietary, glycemic control, diabetic foot care, physical activity and antidiabetic medication-related counseling can be offered by the treating physicians and clinical nurses in the diabetes clinic and all required advising could be repeated by the treating physician/internist at every visit to upsurge patients’ adherence rate. The study subjects enrolled in this study were patients with type-2 DM and those who have a regular follow up in the diabetic clinic. Furthermore, the study participants were a minimum of 18 years old and receiving at least 1 anti-diabetic agent for greater than or equal to 6 months. However, patients with a psychiatric problem or mentally unstable and critically sick cases were not included in the study.
Sample size and sampling technique
The sample size estimation was based on 41.2% of diabetic self-care practice that was conducted among type-2 DM patients at Arba Minch referral hospital, Southern Ethiopia. 21 The required sample size was calculated by a single population proportion formula at a confidence interval (CI) of 95%.

Where, P= proportion of diabetic self-care practice, Z/2 = critical value at 95% level of confidence (Z = 1.96) d = margin of error (5%), n = the required sample size that was 372. However, sample size correction was done using Cochran’s sample size correction formula [n/(1 + (n/N))] based on the number of population with diabetes who have on active follow up in the clinic (n = 470), and considering a 5% non-response rate. The final sample size was calculated to be 217, and a simple random sampling technique was applied to collect the study data.
Study variables and data collection procedure
Socio-demographic, clinical and other data were collected through face-to-face interviews using a structured questionnaire. The socio-demographic study variables were sex, age, marital status, education, occupation, residence, and religion. Whereas, clinical and other variables were glycemic control status, familial history of DM, anti-diabetic treatment modality, sources of medication, access of medication, medication cost affordability, availability of glucometer with strips at home, comorbidities, physical activities, receipt of advice from treating physicians on healthy diet eating, foot care, physical activity, self-monitoring of blood glucose and utilization status medications as per prescribed dose and frequency. Trained clinical nurses who were working in the diabetic follow-up care clinic did the collection of all relevant information from each study subject after an exhaustive explanation of the purpose of study. The 5 main areas concerning diabetes self-care practices are diet, exercise, medication, foot care and self-monitoring of blood glucose (SMBG), and these variables were assessed by the Summary of Diabetes Self-Care Activities (SDSCA) tool. 22 Self-care practice of type-2 DM patients was evaluated by self-report of 15-items of SDSCA among 5 domains of diabetic self-care indicator items (healthy diet = 5, physical activity = 2, SMBG = 2, foot care = 5 and medication = 1). SDSCA scale tool was used to measure the frequency and adherence toward self-care activity status of each domain among patients with type-2 diabetes in the last 7 days.
Operational definitions
Data management and analysis
The questionnaires were double-checked and entered into Statistical Package for Social Sciences (SPSS), Version 23 for statistical analysis. Descriptive statistics (frequency, means, standard deviation (SD), median, interquartile range, and percentages) were tabulated to describe socio-demographic and other important clinical features of the study subjects. Binary logistic regression analysis was done to determine the association and the possible predictors of adherence to each domain of diabetic self-care practice among diabetes patients. All covariates that indicated a P-value <.2 in bivariate analysis also were considered for further analysis in the multivariable logistic regression to control the effect of confounders. The adjusted odds ratio (AOR) with 95%CI were determined to assess the predictors of adherence toward each domain of diabetic self-care. Moreover, the model fitness was tested using the Hosmer-Lemeshow goodness of fit test and P-value <.05 accepted as statistical significance at 95%CI.
Data quality assurance
The questionnaire was primarily set by English language and then translated to Amharic, language, and then translated back to English by independent language teachers. To assure data quality, a pretest was done on 10% questionnaires in other the study site and all compulsory amendment was done based on pretest feedback. In addition, training was given for data collectors (two BSc nurses) by the principal investigator on data collection approach and ethics. The collected data were reviewed and checked carefully by principal investigator daily at the spot during the collection time for its completeness, accuracy, and clarity.
Results
Socio-demographic characteristics of the study population
From a total of 217 identified patients with type-2 diabetes, 207 were included in the study with a response rate of 95%. One hundred five (50.7%) of the participants were males and 102 (49.3%) were females. The mean (±SD) age of study subjects was 51.7 (±12.2) years. One hundred twenty two (59%) of the participants were aged ⩾50 years. The mean (±SD) age since the occurrence of DM was 44.9(±10.1) years with the range of 25 to 72 years (Table 1).
Socio-demographic characteristics of type-2 diabetes patients.

Clinical and treatment features of the study population
The median (IQR) duration of DM since its diagnosis was 5(2-5) years, with a range of 6 months to 25 years. One hundred twenty five (60.4%) of the participants have good glycemic control status (70-130 mg/dl). One hundred sixteen (56%) of the participants were taking oral hypoglycemic agents, while 76 (36.7%) and 15 (7.2%) were using insulin injection and a combination of insulin and oral medication, respectively. The 35 (16.9%) had a family history of DM, while 48 (23.2%) did not know about a familial history of DM (Table 2).
Clinical and treatment characteristics of type-2 diabetes patients.

Abbreviation: IQR, interquartile range.
Patterns of adherence toward self-care among the study population
The overall 47.8% (95% CI: 41.2-55) of patients adhered to diabetic self-care practice, while 108(52.2%) of the diabetes patients did not adhere to diabetic self-care practice. All patients adhered to antidiabetic medication because they received at least 80% of medications as per prescribed dose and frequency. In total, 54.6% (95%CI: 48.8-61.7) of respondents adhered to recommended healthy diet management, whereas 94 (45.4%) did not adhere to a healthy diet management. Moreover, 39.1% (95%CI: 32.6-45.9), 28% (95%CI: 22.2-33.8), and 65.2% (95%CI: 59-72) of the participants adhered to physical exercise, SMBG, and diabetic foot care, respectively (Figure 1).

Adherence toward diabetic self-care among patients with type-2 diabetes.
Factors associated with adherence toward physical exercise
In bivariate analysis, males the crude odds ratio (COR: 2.3; 95%CI: 1.3-4.0), self-employed (COR: 4.6; 95%CI: 1.4-15.6), secondary education (COR: 4.4; 95% CI: 1.9-10), urban dwellers (COR: 3.6; 95%CI:1.6-8.3), comorbidity (COR: 2.2; 95%CI:1.2-3.9) and receipt of advice from treating physicians about performing a physical exercise (COR: 4.2; 95%CI:1.8-9.6) and taking a combination of insulin and oral medication (COR: 4.5; 95% CI:1.3-15) were associated with adherence toward physical exercise.
While, in multivariable analysis, patients who did not know about their family history of DM and received advice from treating physicians on physical exercise were found to have a statistically significant association with the adherence toward physical activity. DM patients who didn’t know about their family history of DM were 7.2 times more likely to have a good adherence toward physical activity when compared to those who had a family history of DM, the adjusted odds ratio (AOR: 7.2, 95% CI:2.0-26.5). Patients who received advice from their treating physicians on physical exercise were 3.5 times more likely to have a good adherent toward physical exercise when compared to their counterparts (AOR: 3.5, 95% CI: 1.1-11; Table 3).
Predictors of adherence toward physical exercise among patients with type-2 diabetes.

Abbreviations: AOR, adjusted odds ratio; COR, crude odds ratio; CI, confidence interval; DM, diabetes mellitus.
P < .2. *P < .05. **P < .01. ***P < .001.
Factors associated with adherence toward recommended healthy diet management
In bivariate analysis, participants who had no a family history of DM (COR: 3.4; 95% CI:1.6-7.5), self-employed (COR: 3.6; 95% CI: 1.6-8.1), unemployed (COR: 2.2; 95% CI: 1.1-4.3), medication cost affordability (COR: 4.4; 95% CI:1.3-15.3), comorbidity (COR: 0.49; 95% CI:0.27-0.87) and receipt of advice from treating physicians on a healthy diet (COR: 2.0; 95% CI: 2.6-10.2) were associated with the adherence to healthy diet management.
However, in multivariable analysis, male sex (AOR: 3.1; 95% CI: 1.5-6.7), self-employed (AOR: 3.6; 95% CI:1.4-9.2), unemployed (AOR: 4.4; 95%CI: 1.8-11.1), no familial history of DM (AOR: 3.3; 95% CI: 1.4-8.0), presence of comorbidity (AOR: 0.45; 95% CI: 0.22-0.91), and receipt of advice on healthy diet from treating physician (AOR: 3.2; 95%CI: 1.2-8.6) were significantly associated with adherence toward healthy diet management (Table 4).
Factors associated with adherence to recommended healthy diet management among patients with type-2diabetes.

Abbreviations: AOR, adjusted odds ratio; COR, crude odds ratio; CI, confidence interval; DM, diabetes mellitus, SMBG, self-monitoring of blood glucose.
P < .2. *P < .05. **P < .01.***P < .001.
Factors associated with adherence toward diabetic foot care
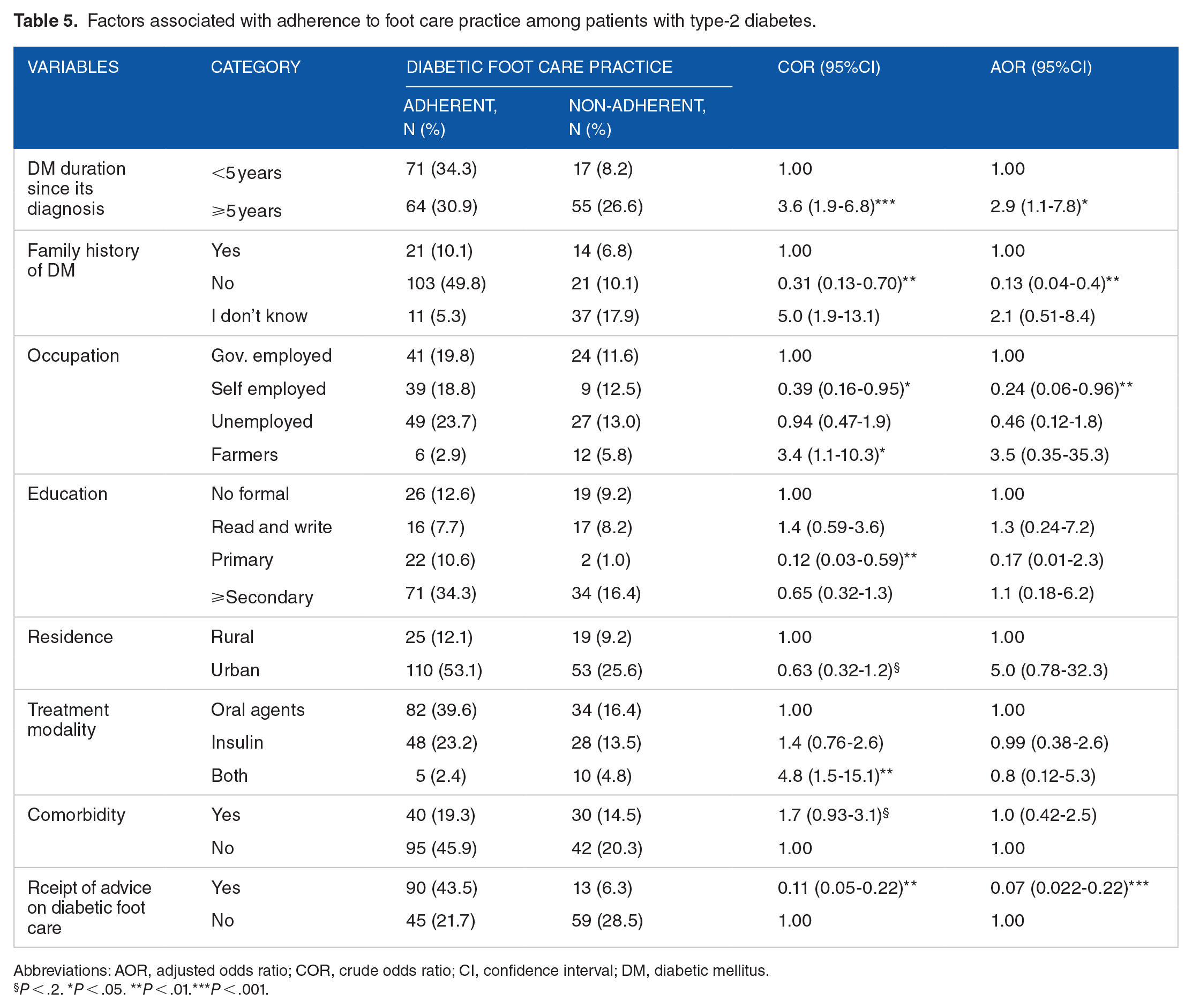
In bivariate analysis, the familial history of diabetes (COR: 0.31; 95% CI: 0.13-0.70), patients who did not know about their familial history of DM (COR: 5.0; 95% CI: 1.9-13.1), DM duration ⩾5 years since its diagnosis (COR: 3.6; 95% CI: 1.9-6.8), being farmers (COR: 1.1; 95% CI: 1.1-10.3), taking a combination of insulin and oral hypoglycemic medication (COR: 4.8; 95% CI: 1.5-15.1), and receipt of advice on foot care from treating physicians (COR: 0.11; 95% CI: 0.03-0.22) were associated with diabetic foot-care. 0.07 (0.022-0.22).
In multivariable analysis, familial history of diabetes, receipt of advice on diabetic foot care, and DM duration ⩾5 years since its diagnosis were found to have a statistically significant association with the adherence to diabetic foot care practice. Patients who did not have a family history of DM (AOR: 0.13; 95% CI: 0.04-0.40), duration of DM ⩾5 years since its diagnosis (AOR: 2.9; 95% CI: 1.1-7.8), and receipt of advice on foot care from treating physician (AOR: 0.07; 95% CI: 0.022-0.22) were significantly associated with adherence toward diabetic foot care (Table 5).
Factors associated with adherence to foot care practice among patients with type-2 diabetes.
Abbreviations: AOR, adjusted odds ratio; COR, crude odds ratio; CI, confidence interval; DM, diabetic mellitus.
P < .2. *P < .05. **P < .01.***P < .001.
Factors associated with adherence toward self-monitoring blood glucose
In multivariable analysis, sex, age, and familial history of DM, duration since the diagnosis of DM, treatment modality, and receipt of advice on self-monitoring blood glucose and having glucometer with strips at home were found to have a statistically significant association with the adherence toward SMBG. The AOR (95%CI) was: 4.1 (1.5-11.3) for the male sex, 0.05 (0.01-0.18) for age ⩾50 years, 3.7 (1.1-11.8) for no familial history of DM, 3.6 (1.2-10.6) for the duration ⩾5 years since the diagnosis of DM, 4.8 (1.2-19.5) for having glucometer with strips, 3.8 (1.3-11.3) for the receipt of advice on SMBG from treating physicians (Table 6).
Factors associated with adherence toward self-monitoring of blood glucose among type-2 diabetes patients.

Abbreviations: AOR, adjusted odds ratio; COR, crude odds ratio; CI, confidence interval; DM, diabetic mellitus, SMBG, self-monitoring of blood glucose.
P < .2. *P < .05. **P < .01. ***P < .001.
Factors associated with glycemic control among patients with type-2 diabetes
In bivariate analysis, being urban dwellers (COR: 2.7; 95% CI: 1.4-5.5) and taking a combination of insulin and oral hypoglycemic medication (COR: 5.9; 95%CI: 1.7-19.7) were associated with glycemic controlling status. In addition, in multivariate analysis, being urban dwellers (AOR: 3.2; 95% CI: 1.4-7.2), medication cost affordability (AOR: 2.4; 95%CI: 1.2-4.6) and receiving a combination of insulin and oral hypoglycemic agents (AOR: 11.2 (2.8-45) were significantly associated with glycemic controlling status (Table 7).
Predictors of glycemic control among type-2 diabetes patients.

Abbreviations: AOR, adjusted odds ratio; COR, crude odds ratio; CI, confidence interval; DM, diabetes mellitus.
P < .2. *P < .05. **P < .01. ***P < .001.
Discussion
Diabetes is 1 of non-communicable diseases that consequence the development of different health complications. Therefore, adherence toward diabetes self-care is vital to limit and manage the risks of developing comorbidity and mortality in diabetes patients. In this study, the authors mainly focused on the assessment of adherence of 5 diabetic self-care domains like SMBG, anti-diabetic medication, physical exercise, diabetic foot care, and recommended healthy diet intake.
In this study, 47.8% (95%CI: 41.2-55) of participants were adhered to overall diabetic self-care. The finding was comparable with the pooled prevalence of adherence toward diabetic self-care among type-2 DM patients in Ethiopia, which was 49% (95%CI: 43-56), 23 and nearly comparable with the study conducted in Mekelle, North Ethiopia, which was 51%. 24 However, inconsistent rate of adherence to diabetic self-care was reported by different studies like 41.2% in Arbaminch, Southern Ethiopia, 21 60.3% in Addis Ababa, Ethiopia, 20 54.5% in West Showa, Ethiopia, 25 38.1% in Harar and Dire Dawa, Eastern Ethiopia, 26 42% in Gauteng, South Africa, 27 28.4% in Bahir Dar, Northwest Ethiopia, 28 and 43.7% in Philippine. 29 This variation might be attributed to the differences in sample size, provision of information concerning the diabetic self-care, and levels of self-care classification between the studies.
In the present study, the adherence toward recommended healthy diet management was 54.6%. The finding was nearly comparable with the study conducted in Dilla, Southern Ethiopia, 49.7%, 30 a meta-analysis report of DM patients in Ethiopia, 50% (95%CI: 42-58) 23 and Philippines, 50%. 29 However, inconsistent finding was reported from different studies like 64.5% in Sudan, 31 62% in Gauteng, South Africa, 27 78% in Davangere, India, 32 47.2% in Harar and Dire Dawa, Eastern Ethiopia, 26 24.1% in Addis Ababa, Ethiopia, 33 and 45.9% in Mangalore and Karnataka, India. 34 The economic status of individuals to access healthy diet, health education on healthy diet utilization, the response of patients with diabetes to adhere and knowledge of DM patients to identify the diet that contains low- and high-carbohydrate contents and low-fat foods might be a plausible factor for the variation.
In this study, male DM patients were 3 times more likely to have good adherence toward healthy diet management than females; and patients who received advice on SMBG from their treating physicians were 6 times more likely to have good adherence toward healthy diet management than their counterparts. This finding in line with the study conducted in Dilla, Southern Ethiopia, 30 in which males were 2 times more likely to have healthy diet adherence than females, and patients who received information were nearly 3 times more likely to have healthy diet management than those who did not receive information concerning the disease. 30
In the present study, the adherence rate toward physical exercise was 39.1% (95%CI: 32.6-45.9). This in line with the study reported from Ambo, West Showa, 35 which was 36.42%. However, inconsistent findings were reported from different studies like 17.6% in Sudan, 31 74% in Mekelle, North Ethiopia, 23 66.9% in Harar and Dire Dawa, Eastern Ethiopia, 26 9% in Gauteng, South Africa, 27 44.5% in Dilla, Southern Ethiopia, 30 and 43.4% in Mangalore and Karnataka, India. 34 In addition, the American Diabetes Association (ADA) recommends physical exercise performance at least 150 minutes/week of moderate aerobic physical activity. 36 The variation may be due to age differences to perform physical exercise, lack of adequate knowledge about the importance of physical activity, lack of access to entertaining and the individual’s motivation to perform physical exercise. Further, a study from Delhi reported that non-adherence to exercise was found usually unrelated to socio-demographic factors and most patients attributed it to clinical pathology especially knee joint pain. 18
In this study, patients who have their glucometer with strips and patients who received advice on physical exercise from their treating physicians were more likely to have good adherence toward physical exercise than their counterparts. Moreover, awareness creation particularly on different types of physical activity performance and selecting a particular exercise is advisable to improve the adherence rate. 37 However; the presence of comorbidities can affect the practice of physical exercise. 38
In the present study, 65.2% (95% CI: 59-72) of the participants were adhered toward diabetic foot care. This finding in line with a study reported from Addis Ababa, Ethiopia, 39 which was 66.6%. However, the proportion was higher than the report of several studies that conducted in Ethiopia like 51.3% in Mekelle, North Ethiopia, 24 39.1% in Harar and Dire Dawa, Eastern Ethiopia, 26 and 58% of meta-analysis report that conducted among DM patients in Ethiopia. 23 The knowledge gap on how to perform foot care, level of advice on diabetic foot care, and socio-economic conditions to purchase suitable footwear may be plausible reasons for the variation of adherence rate between the studies.
In this study, 28% (95% CI: 22.2-33.8) of the participants were adhered toward SMBG. This finding in line with pooled adherence rate toward SMBG of diabetic patients, 23 which was 28% (95%CI: 19-37). However, several studies reported inconsistent rates of adherence toward SMBG for example 20% in Mekelle, North Ethiopia, 24 7.5% in Dire Dawa, 26 55.6% in Philippines, 29 92.18% in South Africa, 27 and 16.5% in Addis Ababa. 33 Moreover, only 15.9% of participants in the present study have glucometer with strips, and the finding was not comparable with the study reported from South Africa 27 that indicated 92% of DM patients have a glucometer to measure and know their blood glucose level. The variability in adherence toward SMBG could be attributed to the economic status of patients to purchase glucometer or to have a check-up in the health institutions between the intervals. Further, patients who have a glucometer with strips were 5 times more likely to have good adherence toward SMBG than their counterparts. In similar, 1 study reported that an association between poor adherence toward SMBG and unavailability of glucometer for DM patients. 24
Moreover, in this study, all patients were adherent to antidiabetic medication, because they received at least 80% of medication as per the prescribed dose and frequency. However, inconsistent rates were reported from different studies: 69.4% in Sudan, 31 83.7% in North Ethiopia, 24 85% in Gondar, Northwest Ethiopia, 40 90% in Eastern Ethiopia, 26 67% in Gauteng, SA 27 76.2% in the Philippines, 29 95.7% in Addis Ababa, 33 76% in Aksum, North Ethiopia, 41 and 45% in Davangere, India. 32 The classification approach of adherence toward antidiabetic medication and the nature of self-reported adherence evaluation condition between the studies might expose the adherence rate evaluation to over or underestimation.
Furthermore, the study conducted in Jimma, Southwest Ethiopia 42 indicated that taking a combination of insulin and oral antidiabetic medication was significantly associated with glycemic control (AOR = 4.59; 95 % CI: 1.05-20.14). Likewise, this study revealed that receiving a combination of antidiabetic agents (insulin + oral hypoglycemic agents) was significantly associated with glycemic control status (AOR = 11.2; 95%CI: 2.8-45.0).
Limitations
First, the study focused on the cross-sectional design and it has limits on the conclusion of causality of adherence patterns. Secondly, most of the adherence evaluations relied on self-reports and activity, this might be susceptible to bias. Third, the study was conducted in a single health institution and patients with type-2 diabetes, so the finding cannot be generalized to all diabetes patients as a whole. Fourth, this study assessed only the antidiabetic medication adherence rate, but not the medications for comorbid diseases like hypertension, cardiac problem, and others.
Conclusion
This study indicates 52.2%, 72%, and 60.1% of patients with diabetes have not adhered to the practice of diabetic self-care, SMBG, and physical exercise, respectively. Therefore, improving awareness and regular education on diabetes is imperative to scale up patients’ adherence toward diabetic self-care practice.
Footnotes
Acknowledgements
We want to acknowledge nurses who were working in the diabetic follow up clinic for their support during data collection. Our gratefulness is also protracted to Sr. Enisha Seyoum for her invaluable support during data collection and patients with type-2 diabetes for their keen participation in the study.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by Hawassa University.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
GD designed the research, performed data collection, data entry, and interpretation. KW was advisor throughout the project. ST supported interpretation and appraisal. ATH analyzed data, did result interpretation, and wrote the manuscript including appraisal. All authors read and approved the final manuscript.
Availability of Data
The dataset of this article is not openly accessible but it can be available on reasonable requests from the corresponding author with authorization of Hawassa University’s comprehensive specialized hospital clinical director office.
Ethical Approval and Infomed Consent
The study was ethically approved by the institutional review board (IRB) of Hawassa University College of Medicine and health sciences (Ref. No: IRB/014/12). Permission of data collection was obtained from the Clinical and Academic Director Office of Hawassa University Comprehensive Specialized Hospital. All the study subjects provided written informed consent to participate in this study before data collection. All studies on humans defined in the present manuscript were conducted with the approval of the accountable ethics committee and as per national law and the Helsinki Declaration of 1975 (in its recent, revised form). The privacy of the study participants’ information was kept confidentially.