
Abstract
Introduction:
Only 3 types of coronavirus cause aggressive respiratory disease in humans (MERS-Cov, SARS-Cov-1, and SARS-Cov-2). It has been reported higher infection rates and severe manifestations (ICU admission, need for mechanical ventilation, and death) in patients with comorbidities such as diabetes mellitus (DM). For this reason, this study aimed to determine the prevalence of diabetes comorbidity and its associated unfavorable health outcomes in patients with acute respiratory syndromes for coronavirus disease according to virus types.
Methods:
Systematic review of literature in Pubmed/Medline, Scopus, Web of Science, Cochrane, and Scielo until April of 2020. We included cohort and cross-sectional studies with no restriction by language or geographical zone. The selection and extraction were undertaken by 2 reviewers, independently. The study quality was evaluated with Loney’s instrument and data were synthesized by random effects model meta-analysis. The heterogeneity was quantified using an I2 statistic. Funnel plot, Egger, and Begg tests were used to evaluate publication biases, and subgroups and sensitivity analyses were performed. Finally, we used the GRADE approach to assess the evidence certainty (PROSPERO: CRD42020178049).
Results:
We conducted the pooled analysis of 28 studies (n = 5960). The prevalence analysis according to virus type were 451.9 diabetes cases per 1000 infected patients (95% CI: 356.74-548.78; I2 = 89.71%) in MERS-Cov; 90.38 per 1000 (95% CI: 67.17-118.38) in SARS-Cov-1; and 100.42 per 1000 (95% CI: 77.85, 125.26 I2 = 67.94%) in SARS-Cov-2. The mortality rate were 36%, 6%, 10% and for MERS-Cov, SARS-Cov-1, and SARS-Cov-2, respectively. Due to the high risk of bias (75% of studies had very low quality), high heterogeneity (I2 higher than 60%), and publication bias (for MERS-Cov studies), we down rate the certainty to very low.
Conclusion:
The prevalence of DM in patients with acute respiratory syndrome due to coronaviruses is high, predominantly with MERS-Cov infection. The unfavorable health outcomes are frequent in this subset of patients. Well-powered and population-based studies are needed, including detailed DM clinical profile (such as glycemic control, DM complications, and treatment regimens), comorbidities, and SARS-Cov-2 evolution to reevaluate the worldwide prevalence of this comorbidity and to typify clinical phenotypes with differential risk within the subpopulation of DM patients.
Keywords
Introduction
Coronavirus is a family of viruses that cause respiratory diseases, and 7 of its types can affect humans. 1 Aggressive acute respiratory syndromes are produced by 3 of them. The Severe Acute Respiratory Syndrome Coronavirus type 1 (SARS-Cov-1) originated an outbreak in 2002-2003 in Guangdong, a province in China 2 with a mortality rate of 10%; 3 Middle East Respiratory Syndrome Coronavirus (MERS-Cov) caused other outbreak in Saudi Arabia in 2012, and its lethality reached 34.3%; 4 and Severe Acute Respiratory Syndrome Coronavirus type 2 (SARS-Cov-2) reported its firsts pneumonia cases in the province of Wuhan in China at the end of 2019. Due to its spread and severity, the World Health Organization (WHO) declared it a pandemic on March 11th, 2020. 5
One of the most frequent reported comorbidities of infected adult patients with coronaviruses is diabetes mellitus (DM). 6 Several mechanisms are postulated to explain this association: (1) increased cell affinity and efficient virus entrance by overexpression of angiotensin-converting enzyme 2 (ACE2) receptor7-9 in the case of SARS-Cov-1 and SARS-Cov-2, and dypeptil peptidase 4 protein (DPP4) for MERS-Cov; (2) decreased viral clearance10,11; (3) decreased quantity and function of T-cells 12 ; (4) susceptibility to hyperinflammation by an increase of pro-inflammatory cytokines 13 ; (5) increased cytokines profile without an appropriate stimulus 14 ; and (6) the high comorbidity with cardiovascular diseases such as hypertension which is treated with ACE inhibitors, thus overexpressing the ACE2 receptors in these patients.15,16
DM is associated with poor outcomes in patients with coronavirus infection. In patients with DM, the infection of MERS-Cov is associated with admission to intensive care unit (ICU) (P < .05), 17 need of mechanical ventilation (MV) (P < .05), 18 and a high risk of death (OR: 1.8, 95% CI: 1.5-2.1). 19 In SARS-Cov-2 is similar, among DM patients, 17% 20 were hospitalized in UCI, 20.3% needed MV, 21 and from 10.6% to 47.2% died.21,22 DM is highly prevalent, around the world there are approximately 415 million people 23 with DM, and in the context of the current SARS-Cov-2 pandemic they become a extremely high-risk group to adverse outcomes during an eventual infection. However, the prevalence of DM and coronavirus comorbidity has not been fully explored and compare by virus type, nor has the frequency of poor outcomes in this high-risk population subgroup. Therefore, we aimed to determine the pooled prevalence of DM and its associated unfavorable health outcomes in patients with acute respiratory syndromes for coronavirus disease according to virus type.
Materials and Methods
Protocol and registration
Our study was performed according to the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), 24 the checklist appears in Supplemental Material 1. The study protocol was registered at PROSPERO, number CRD42020178049.
Literature search and study selection
A systematic search was carried out in the following databases: PubMed/Medline, Scopus, Web of Science, Cochrane (via OvidSP), and Scielo until April 2020. Additionally, systematic reviews were explored to identify potential eligible articles for our analysis.
The search strategy included Medical Subject Title (MeSH) terms for “Diabetes Mellitus” and related words for “COVID-19” or “Severe acute respiratory syndrome coronavirus 2” (complete details of the search strategy appear in Supplementary Material 2). Cohorts and cross-sectional studies were included, and no restriction was made with respect to language and geographical area. Any other type of publication was excluded (letter, note, conference paper, short survey, editorial and erratum, review articles, case studies, case-control studies, vaccination and clinical trials, or family-based studies).
The inclusion criteria were: (1) available data of more than 10 patients; (2) adult patients; (3) number of participants with confirmed diagnosis of DM type I or II; and (4) confirmed diagnosis of coronavirus infection. Duplicate documents were removed with Endnote X9 Software. Subsequently, titles and abstracts were selected to identify potentially relevant articles according to the inclusion criteria. Lastly, potential articles were evaluated in full text to assess their eligibility. Two authors carried out the selection process independently (CGO & CIE) and third author (IPT) resolved discrepancies by discussion and consensus. The complete list of articles excluded at this stage of the full text is available in Supplemental Material 3.
Data extraction and quality evaluation
Two authors (CGO and PZL) independently extracted the following data from each included article using a standardized form in Microsoft Excel. Author, year of publication, country, study design, number of participants, characteristics of the population, type of virus, clinical outcome, gender, and prevalence estimates were extracted. A third author (MYA) checked that the data quality before analysis. When studies with the same population were identified, only the most recent or complete publication was included.
We assessed the quality of the prevalence studies according to the questionnaire developed by Loney et al. 25 The study’s quality was based on 8 criteria grouped into 3 dimensions: validity, results, and applicability. We assigned one point if the following criteria is present in the study: (1) random sample or the whole population; (2) unbiased sampling frame (ie, census data); (3) adequate sample size (>50 subjects); (4) standard and objective criteria for DM definition were used; (5) outcomes were measured in an unbiased fashion; (6) adequate response rate (70%) and non-responders were described; (7) confidence intervals and subgroup analysis were reported; and (8) study subjects were described in detail. The total score was calculated for each study (score range 0-8). Quality score of 0 to 2 was considered very low, score of 3 to 4 as low, score of 5 to 6 as moderate, and score of 7 to 8 as high quality.
Statistical analyses
Our primary outcome was the prevalence of patient with coronavirus infection and DM comorbidity as the proportion from the total reported patients with coronavirus diseases. We also calculated and reported the median prevalence and interquartile ranges (IQR). Our secondary outcomes were the frequency of poor health outcome as the proportion of ICU admission, mechanical ventilation, and deaths. All the analyses were performed separately by virus type.
The data were synthesized by meta-analysis analytical techniques. Heterogeneity was quantify using an I2 statistic. Because of the proportions were often expected to be near to 0 or 1, we used Freeman-Tukey Double Arcsine transformation to stabilize the variances before to implement a random effects meta-analysis implementing the DerSimonian-Laird method (due to the a priori expected high between-study heterogeneity).26,27 The pooled estimates were expressed as prevalence per 1000 infected patients with the corresponding 95% confidence intervals using the exact method. 28 We conducted subgroups analysis according gender and country. We also conducted a post-hoc sensitivity analysis according risk of bias categories, sample size, study design, data collection, number of centers, sampling type, and excluding 1 study at the time to test single-study influence.
Additionally, we conducted univariate meta-regression to test the influence of study level moderators on the prevalence of DM and coronavirus comorbidity. 29 We based our analysis on the Thompson and Higgins recommendations, 30 we hypothesized that sample size, study design, diagnostic criteria, and study quality will have an effect on the prevalence estimate. Each moderator was tested on a minimum of 8 included studies in the meta-analysis. 30 To select the best model, we assessed the residual percentage of variation due to heterogeneity and the proportion of between-study variance explained in addition to the significant criterion of P < .05 per each moderator. Furthermore, funnel plots, and Egger’s and Begg’s tests were used to evaluate publication bias. All statistical analyses were performed using STATA 15.
Evidence certainty assessment
As recommended by Cochrane, 31 we assessed the certainty of the evidence (pooled estimates) from our included studies in the quantitative synthesis. The grading of recommendation, assessment, development, and evaluation (GRADE) instrument 32 was used. This critical appraisal was based on considerations such as study design, inconsistency, indirectness, imprecision, and publication bias as stated in the GRADE handbook. 33 We adapted the assessment to prevalence estimates. The certainty of the evidence was characterized as high, moderate, low, or very low. 32 The results were reported as a summary of findings table (SoF), performed in the GRADE online tool (http://gradepro.org).
Results
Studies characteristics
A total of 84 documents were identified during the initial search and 11 duplicates were removed. In the review by title and abstract, there were 44 potentially eligible documents. To the above, 11 articles found in the citations of the systematic reviews identified were added. In the full-text evaluation, 27 documents were excluded either by design or population characteristics, and finally 28 were included in the study (Figure 1).
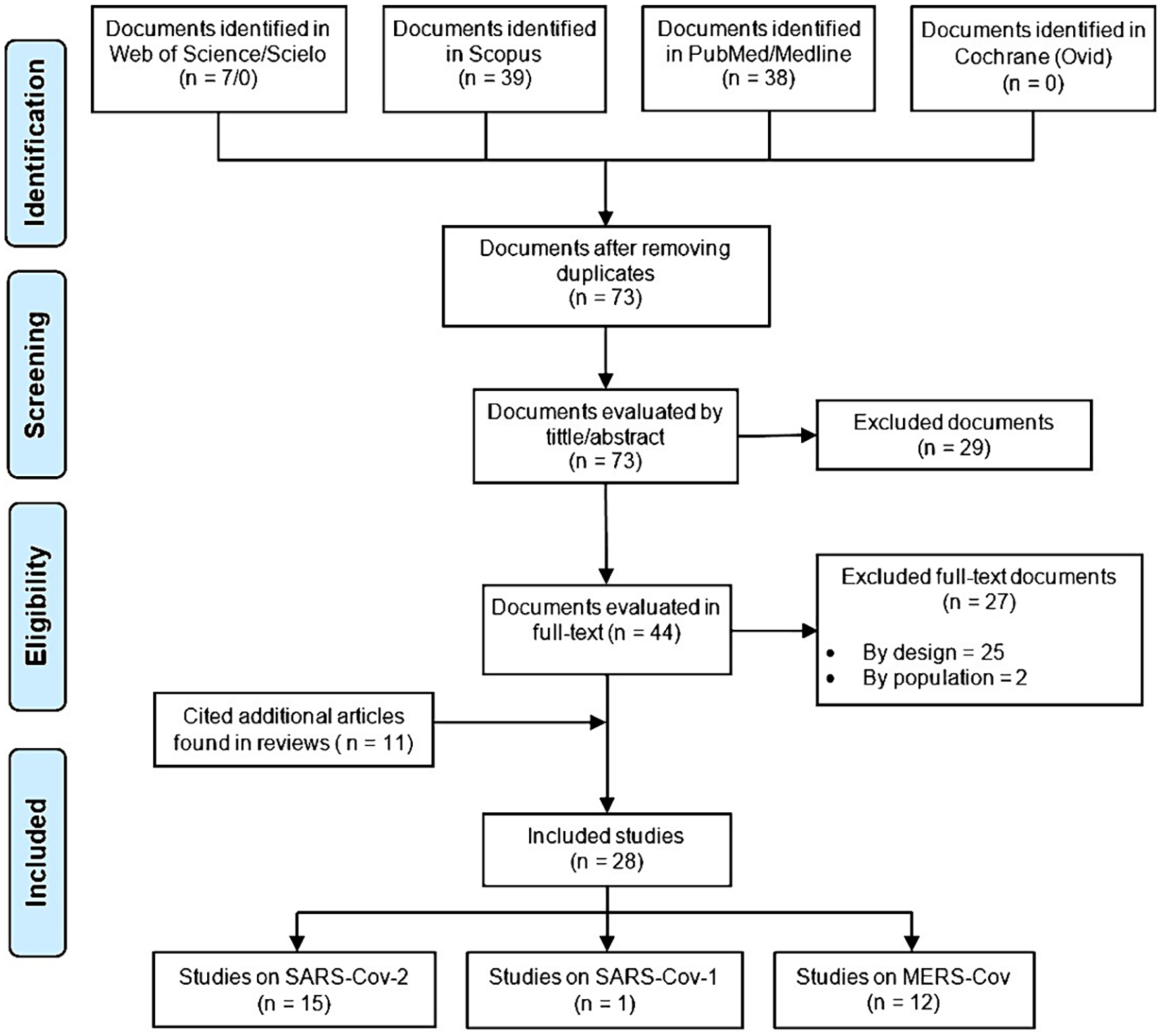
Flow chart of study selection.
The publication years of the included studies ranged from 2006 to 2020. Most of the studies were from China (14), eleven studies from Arabia; Italy, Singapore, and South Korea had 1 study, respectively. Fourteen studies were multicentric, 24 were cohort studies, and 4 studies were cross-sectional. Regarding, the type of virus, 12 studies included MERS-Cov cases, 1 study included SARS-Cov-1 patients, 15 studies included SARS-Cov-2 cases. Also, the most common diagnostic criteria for coronavirus infection were molecular test (24 studies), followed by clinical criteria (2 studies). Descriptive information on each included article is provided in Table 1.
Descriptive information on each article included in the systematic review.

MERS-Cov, Middle East Respiratory Syndrome Coronavirus Disease; SARS-Cov-1, Syndrome Acute Respiratory Syndrome Coronavirus Disease type 1; SARS-Cov-2, Syndrome Acute Respiratory Syndrome Coronavirus Disease type 2; ICU, Intensive Care Unit; MV, mechanical ventilation; NR, not reported; F, female; M, male.
The 28 studies reported data on the prevalence of DM, MERS-Cov studies reported 507 diabetic patients from 1682 participants, the SARS-Cov-1 study included 47 diabetic patients from 520 total participants, and SARS-Cov-2 studies reported 387 diabetic patients from 3758 participants.
Study quality
The range of quality score 25 for the included studies was from 1 to 5, the sixth domain (adequate response rate) was non evaluable in all the studies; whereas the fourth and fifth domain (standard and unbiased measurement) obtained the more negative responses. Most of the studies were of very low quality (75%). From the MERS-Cov studies, 9/12 documents had very low quality (score of 0-2), the SARS-Cov-1 study had a low quality (score of 3-4), and from the SARS-Cov-2 studies, 12/15 documents had very low quality (score of 0-2).
Pooled prevalence estimates
We performed the pooled analysis of the 28 studies (n = 5960). Due to data availability the pooled estimates were performed for MERS-Cov and SARS-Cov-2 studies. The median prevalence proportions and their IQR were 49.3% (29.5-61.4) and 10.8% (5.9-16.6) for MERS-Cov and SARS-Cov-2, respectively. The prevalence analysis according to virus type were 451.9 diabetes cases per 1000 infected patients with MERS-Cov (95% CI: 356.74-548.78, I2 = 89.71%, n = 1682, 12 studies); 90.38 per 1000 patients with SARS-Cov-1 (95% CI: 67.17-118.38, n = 520); and 100.42 per 1000 infected patients with SARS-Cov-2 (95% CI: 77.85-125.26, I2 = 67.94%, n = 3758, 15 studies) (Figure 2).

Meta-analysis of the prevalence of diabetes mellitus in patients with acute respiratory syndromes by coronavirus type. (a) Meta-analysis from MERS-Cov studies. (b) Meta-analysis from SARS-Cov-2 studies.
Unfavorable health outcomes estimates
Unfavorable health outcomes were assessed only in patients with DM. The mortality rate in patients with MERS-Cov (6 studies) was 356.53 per 1000 (95% CI: 294.45-420.98, I2 = 0%), in SARS-Cov-1 (1 study) was 55.77 per 1000 (95% CI: 37.66-79.11), and in SARS-Cov-2 (2 studies) was 96.33 per 1000 (95% CI: 61.36-137.66, I2 = 0%). Mechanical ventilation was reported in just 1 study both MERS-Cov and SARS-Cov-2 and ICU admission was reported in 2 studies in MERS-Cov and just 1 in SARS-Cov-2. The completed estimates are described in the Table 2.
Prevalence of comorbidities and unfavorable outcomes in patients with diabetes mellitus and acute respiratory syndromes for coronavirus disease.

n, number of studies; CI, confidence interval, I2, heterogeneity test; ICU, intensive care unit; MERS-Cov, Middle East Respiratory Syndrome Coronavirus; SARS-Cov-1, Severe Acute Respiratory Syndrome Coronavirus type 1; SARS-Cov-2, Severe Acute Respiratory Syndrome Coronavirus type 2.
Prevalence of each adverse outcome per 1000.
Subgroup Analysis
In the MERS-Cov studies, the prevalence in women was 330.91 per 1000 infected patients (95% CI: 307.98-354.23, I2 = 0%) while in men was 666.73 per 1000 (95% CI: 627.43-704.95, I2 = 35.39%). Eleven studies are from Arabia Saudi, the prevalence was 475.76 per 1000 (95% CI: 364.06-588.63, I2 = 90.62%) and 1 study from Korea with a prevalence of 279.57 per 1000 (95% CI: 216.38-349.93). In the SARS-Cov-2 studies, the DM prevalence in women were 420.07 per 1000 infected patients (95% CI: 329.76-513.06, I2 = 95.71%) while in men was 579.93 per 1000 (95% CI: 486.94-670.24, I2 = 95.71%). According to the country, the DM prevalence in China was 101.79 per 1000 infected patients (95% CI: 73.42-133.81, I2 = 70.01%), in Singapore was 55.56 per 1000 (95% CI: 1.41-272.94), and in Italy was 113.14 per 1000 (95% CI: 97.98-129.73) (Table 3).
Diabetes mellitus prevalence according to subgroup analysis in patients with MERS-Cov and SARS-Cov infections.

n, number of studies; CI, confidence interval; I2, heterogeneity test; MERS-Cov, Middle East Respiratory Syndrome Coronavirus; SARS-Cov-2, Severe Acute Respiratory Syndrome Coronavirus type 2.
Diabetes prevalence per 1000.
Sensitivity analysis
For both MERS-Cov and SARS-Cov-2 evidence bodies, the pooled estimates were not significantly different even if the study with the largest estimation was removed from the analysis and also when we excluded 1 study at a time.
In the sensitivity analysis of MERS-Cov studies, we found that the DM prevalence was double in very low quality studies (539.38 per 1000, 95% CI: 452.59-626.24, I2 = 53.47%) compared to the low (279.57 per 1000, 95% CI: 216.38-349.93) and moderate quality (246.30 per 1000, 95% CI: 222.27-271.14). The DM prevalence was higher when the studies had a small sample (543.94 per 1000, 95% CI: 441.40-644.76, I2 = 59.09%). All studies had longitudinal design and 11/12 were historical cohorts. The prevalence was higher in retrospective studies (475.76 per 1000, 95% CI: 364.06-588.63, I2 = 90.62%).
In the SARS-Cov-2 studies, 12/15 had very low quality with a DM prevalence of 111.34 per 1000 (95% CI: 81.62-144.63, I2 = 66.57%), in studies with a large sample quantity (50 or more subjects) the prevalence was higher (131.50 per 1000, 95% CI: 69.54-206.63, I2 = 0%) than in small sample studies. The DM prevalence was similar according to study design (longitudinal: 100.14 per 1000 and cross-sectional: 104.59) and by the number of centers that participate in the study (single-center: 107.30 per 1000 and multi-center: 93.72 per 1000). The rest of analysis are described in the Table 4.
Diabetes mellitus prevalence according to the sensitivity analysis of MERS-Cov and SARS-Cov studies included in the systematic review.

n: number of studies, *diabetes prevalence per 1000.
CI: confidence interval, I2: heterogeneity test.
MERS-Cov: Middle East Respiratory Syndrome Coronavirus.
SARS-Cov-2: Severe Acute Respiratory Syndrome Coronavirus type 2.
Meta-regression
The univariate meta-regression analyses showed that the prevalence of DM and MERS-Cov comorbidity was higher across studies with relatively small sample sizes (b = 0.28, 95% CI: 0.13-0.43), single-center studies (b = 0.29, 95% CI: 0.12-0.46), hospital-based studies (b = 0.22, 95% CI: 0.03-0.41), and studies with convenience sampling method (b = 0.22, 95% CI: 0.03-0.41). Moreover, we found the quality score influence indirectly the pooled prevalence estimate, meaning for one point increases in the quality score, the estimated prevalence decrease by 8% (b = −0.08, 95% CI: −0.12 to −0.03) (Figure 3). The covariate with stronger influence on prevalence was the quality score, the model explained the 100% of the between-study variance and the residual heterogeneity was 0%. We did not implement multivariate model due to the small number of included studies. For the SARS-Cov-2 meta-analysis, none of the variables influenced the pooled prevalence.

Bubble plot with fitted meta-regression line. The prevalence of DM in patients infected with MERS-Cov (horizontal axis) is presented against the quality score points of the included studies. For each point increase in the quality score the prevalence decreases 8%. The model reported an adjusted R-squared of 100% and a residual I2 of 0%.
Publication bias
In MERS-Cov studies, the funnel plot (Figure 4) shows asymmetry of the estimates suggesting publication bias, although the significance tests have dissociated result (Egger’s test P < .01, Begg’s test P = .13). In case of SARS-Cov-2 studies, the funnel plot shows no publication bias and tests have no significative result (Egger’s test P = .88, Begg’s test P = .88). The SARS-Cov-1 analysis was not possible because only we had 1 study.

Funnel plot for systematic review on the prevalence of diabetes mellitus by virus type. The effect size (horizontal axis) is presented against the standard error of effect size (ES). (a) Funnel plot of MERS-Cov studies. (b) Funnel plot of SARS-Cov studies.
Evidence certainty
Overall, the certainty of the evidence of the pooled prevalence estimates assessed by the GRADE approach was very low (Table 5). No population-based studies were included in either meta-analysis, thus, we started the certainty rating from low certainty. Due to the high risk of bias (75% of included studies were categorized as very low quality), high heterogeneity (I2 higher than 60% in both meta-analyses), and publication bias (for MERS-Cov studies), we down rate the certainty to very low, suggesting that the current evidence is very uncertain about the prevalence of DM and coronavirus comorbidity for the threes included virus types.
Summary of findings.

CI, Confidence interval; MERS-Cov, Middle East Respiratory Syndrome Coronavirus; SARS-Cov-1, Severe Acute Respiratory Syndrome Coronavirus type 1; SARS-Cov-2, Severe Acute Respiratory Syndrome Coronavirus type 2.
The certainty rating started from low since no population-based study were found.
High risk of bias (very low quality by Loney’s scale) was detected in most of the included studies (75%), due to the inadequate response rate, case definition, and outcome measurement.
High inconsistency was detected in both meta-analyses. The calculated I2 was >60%.
Publication bias was detected in MERS-Cov meta-analysis (asymmetrical funnel plot and significant Egger’s test).
Discussion
The estimated prevalence of DM in patients with acute respiratory syndrome due to coronaviruses is high, roughly 10% to 45%, although from evidence with very low certainty. The estimate varies based on the virus type, with higher prevalence in infected patients by MERS-Cov (451.9 cases per 1000), followed by SARS-Cov-2 (100.42 per 1000), and SARS-Cov-1 (90.38 per 1000). Moreover, the proportion of these patients with reported unfavorable health outcomes is high, predominantly ICU admission, mechanical ventilation use, and deaths. These estimates were higher for MERS-Cov and SARS-Cov-2.
DM are associated with an increased risk of respiratory infections (bacterial or viral) and unfavorable health outcomes after infections, this has been reported for influenza, 59 pneumococcal, 60 and tuberculosis 61 infections. In the context of coronaviruses, this trend is repeated and the infection proportion in diabetic patients is greater than in general population. However, we found that within the coronavirus types, the proportion is different. The prevalence of DM comorbidity was up to 4 times higher in patients infected with MERS-Cov than SARS-Cov-1 or SARS-Cov-2.
We have raised several hypotheses in this regard, one of them is based on the binding protein that each coronavirus uses to enter the cell. In the case of SARS-Cov-1 and SARS-Cov-2, this protein is ACE-2, 62 which is higher in diabetic patients. For MERS-Cov the binding protein is dipeptidyl peptidase 4 (DPP4), 63 which is increased in DM patients as well, but there also other conditions that by themselves increase their expression like all manifestation of metabolic syndrome (obesity, fatty liver disease, and high waist circumference). 64 Thus, the synergy of these clinical conditions that usually coexist in the patients with type 2 DM would increase the amount of DPP4 available therefore, it will facilitate the virus binding, making the patient with diabetes more prone to becoming infected by MERS-Cov. Unlike ACE-2 protein, increased DDP4 protein values are associated with impaired immune response 65 to eliminate MERS-Cov, 66 this would explain the higher mortality reported.
An alternative explanation is the different regional prevalence of DM. Diabetes prevalence is higher in Arabia (18.2%-31.6%) 67 than China (4%). 68 In our study we found 91.67% of MERS-Cov studies were from Arabia (11/12 studies), whereas 100% and 86.67% were from China in SARS-Cov-1 (1 study) and SARS-Cov-2 (13/15 studies), respectively. This notable difference in the prevalence of DM in general population could influence the proportion of patients infected with coronavirus due to patient availability.
In subgroup analysis we found in MERS-Cov studies, the DM prevalence is double in men than women and this is related to the fact, that male have higher risk for develop DM in Arabia where most of the studies come from (11/12 studies, n = 1496). The explanation for this fact could be a sub diagnosis of DM due to gender inequalities that do not allow equal access to health. 69 Furthermore, Saudi women reported greater adherence to diet and exercise than men. 70 In SARS-Cov-2 studies, the influence of male gender in DM prevalence is present, yet smaller. There are 2 countries (Italy and China) that contribute almost the entirety of the studied sample, that could explain these differences. Italy, with aging population, 71 the higher prevalence of DM is in men 72 explained by the predisposition to greater central fat deposit in men than in women after 65 years. 73 In China, population with a high education level, 74 there is a direct relationship between obesity and DM with the academic degree in men, and inversely in women. 75
Since the heterogeneity was high in both meta-analyses, we performed a sensitivity analysis and meta-regression models to assess further causes of inconsistency in the estimated effects. We identify in both analysis that the quality of the studies was the most important cause of heterogeneity (studies with better quality reported small prevalence). Most of the studies were of very low quality with a score of 0-2 (MERS-Cov: 9/12 and SARS-Cov-2: 12/15). These results are expected because our units of analysis were observational studies based on hospital reports during outbreaks. There is no random selection of cases, nor was the entire population included, and it was not possible to blind the assessors. Regarding the ideal sample size, Loney et al 25 considers a size greater than 300 patients adequate, given the context of our study (18/28 studies had a sample of less than 100), we considered a lower threshold (50 participants) so some low-quality studies (score 3-4) could be overestimated. In addition, for the MERS-Cov meta-analysis, we identified the sample size (less than 50, or equal or greater than 50) and the number of centers included in the study (single center vs multicenter studies) were important factors of heterogeneity, the pooled estimate is higher in single-center studies with small sample size. In SARS-Cov-2 meta-analysis, we could not identify the main source of heterogeneity, probably explained by the homogenous design and geographical location of the included studies. These findings highlight the need of high-quality, well-powered, and population-based studies to elucidate the relationship between DM and coronavirus infection. Moreover, the lack of clinical data of the reported DM cases such as glycemic control status, glycosylated hemoglobin values, current treatment, and DM associated comorbidities, prevent a better characterization of the within and between-studies heterogeneity.
Diabetic patients infected with coronavirus have higher rate of unfavorable health outcomes (ICU admission, need for mechanical ventilation, and death) than the general population. We found a pooled mortality rate from 6% to 36%, higher for MERS-Cov infection. For SARS-Cov-2 infection, we found a rate of 10% approximately, this represent the double of current reported values of 5% mortality in overall worldwide population (calculated with data till Jun 27th, 2020) 76 SARS-Cov-1 and SARS-Cov-2 bind only to glycosylated ACE-2 receptors, 77 therefore, the worse the glycemic control, the greater the number of glycosylated receptors and the worse the prognosis. 78 Furthermore, if we added the well-known maladaptive immune response associated with DM, the health outcomes are much more adverse. These findings are aligned with a recent meta-analysis reporting twice odds (RR 2.12, 95% CI: 1.44-3.11, I2 = 72%) for death and disease severity in DM population with SARS-Cov-2 infection. 79 Likewise, the scarce clinical characterization of the DM cases infected with coronaviruses hinder the possibility to typify clinical phenotypes with higher or less risk within the subpopulation of DM patients, that could have a great impact in public health policies. We recommend in future studies a complete clinical-pharmacological profile of DM patients infected with coronaviruses, specially SARS-Cov-2 including glycemic control status, comorbidities, treatment regimens and the presence of long-term complications related to DM.
It is important to mention, we included less studies and we found a lower prevalence of DM for hospitalized patients with SARS-Cov-2 compared with other reviews 80 because the presented proportions are based on report of DM as a diagnosis prior to coronavirus infection. We did not count the studies that reported only hyperglycemia without making the distinction between DM and hyperglycemia from other causes. In SARS-Cov-1 and SARS-Cov-2 infections, the hyperglycemia could be explained by the virus bond to ACE-2 receptors expressed on islet cells of the pancreas, which can cause their inflammation resulting in insulin-dependent hyperglycemia. 77 This event could be a confounder in the prevalence calculation in previous studies 6 thus, we followed a strict DM definition criterion to calculate estimates with more precision.
The main limitation of this systematic review is the small number of countries included, which prevents comparisons between regions. However, data from this latest pandemic has not been fully determined due to the recent nature of its presentation. In our review, countries such as France, Spain or the United States were not represented. In other regions, such as South America or the Caribbean, there are issues regarding DM diagnosis, which in many cases is reported as stress-induced hyperglycemia, that could bias the prevalence estimation.
Conclusion and Recommendations
The prevalence of DM in patients with acute respiratory syndrome due coronavirus infection is high (451.9 cases per 1000 infected patients for MERS-Cov, 90.38 per 1000 for SARS-Cov-1 and 100.42 per 1000 for SARS-Cov-2), and the unfavorable health outcomes are frequent in this subset of patients. In the context of the pandemic that we are going through, we recommend that researchers in each country continue to publish well-powered and population-based observational studies including detailed DM clinical characteristics (such as glycemic control, DM complications, and treatment regimens), comorbidities, and evolution of SARS-Cov-2 to reevaluate the worldwide prevalence of this comorbidity and to typify clinical phenotypes with higher or less risk within the subpopulation of DM patients.
Supplemental Material
Supplementary_materials – Supplemental material for Prevalence of Diabetes Mellitus and Its Associated Unfavorable Outcomes in Patients With Acute Respiratory Syndromes Due to Coronaviruses Infection: A Systematic Review and Meta-Analysis
Supplemental material, Supplementary_materials for Prevalence of Diabetes Mellitus and Its Associated Unfavorable Outcomes in Patients With Acute Respiratory Syndromes Due to Coronaviruses Infection: A Systematic Review and Meta-Analysis by Isabel Pinedo-Torres, Magaly Flores-Fernández, Marlon Yovera-Aldana, Claudia Gutierrez-Ortiz, Paolo Zegarra-Lizana, Claudio Intimayta-Escalante, Cristian Moran-Mariños, Carlos Alva-Diaz and Kevin Pacheco-Barrios in Clinical Medicine Insights: Endocrinology and Diabetes
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Self-financed.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ Contributions
IPT, MFF, and MYA conceptualized the idea; CMM design the search strategy; CGO, CIE, and PZL review the citations and extracted the data; IPT, CAD, MYA, and KPB made the statistical analysis; IPT, MFF, MYA, CAD, CMR, CGO, PLZ, CIE, and KPB wrote the first draft; and all authors interpreted the results, and reviewed and approved the final manuscript.
Contribution to the Field Statement
Three of the 7 coronaviruses (MERS-Cov, SARS-Cov-1, SARS-Cov-2) can cause respiratory infections in humans, much more severe and even sometimes fatal than the other coronaviruses. These viruses have caused major outbreaks of deadly pneumonia in the 21st century. According to WHO data, there are 415 million people with diabetes mellitus. People with this disease have chronic low-grade inflammation, leading to immune dysfunction, microvascular and macrovascular complications; therefore, they may have an increased risk of coronavirus infection and its complications.
The present study reports the prevalence of diabetes mellitus in patients with acute respiratory syndrome for coronavirus and its associated unfavorable outcomes. In addition, we hypothesis the possible causes for the different prevalence of diabetes among the virus types based on pathophysiological explanations. Moreover, we explored the between-study heterogeneity with subgroup, sensitivity, and meta-regression analyses. Finally, we suggested recommendations for future studies addressing this question.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.