
Abstract
Neuroendocrine neoplasms (NENs) are derived from neuroendocrine cell system and can have benign or malignant characteristics. They are rare tumors, but have been increasing in incidence over the past 40 years. Patients with NENs may develop symptoms due to primary tumor invasion, metastasis, or from secretion of hormonally active tumor substances. Multiple imaging modalities are used for diagnosis and staging, including specialty scans such as 111In pentetreotide (Octreoscan) and 68Gallium-DOTATATE, along with endoscopy, endoscopic ultrasound, and biochemical marker testing. Treatment involves both surgical approach, for both primary and metastatic lesions, as well as medical management for symptom management and disease progression. This article will review the current clinical knowledge regarding the diagnosis, treatment, and prognosis of these fascinating neoplasms and the associated hormonal syndromes.
Background
Neuroendocrine neoplasms (NENs) are derived from the neuroendocrine cell system and can have benign or malignant characteristics. Neuroendocrine neoplasms are divided into 2 groups: neuroendocrine tumors (NETs) and neuroendocrine carcinomas (NECs). Neuroendocrine tumors are defined as well-differentiated, low-proliferating NENs, whereas NECs are defined as poorly differentiated, high-proliferating NENs. Gastrointestinal (GI) NETs were previously referred to as “carcinoids,” which was first used by German pathologist Oberdorfer in 1907 as “karzinoide.” 1 However, this term has fallen out of favor as pathologists often applied it to tumors with neuroendocrine features, whereas clinicians used it to describe tumors producing carcinoid syndrome. 2
Biology
Neuroendocrine cells are thought to be either from epithelial or neuroectodermal origin. Gastrointestinal NETs are mainly of epithelial origin. 3 They are histologically characterized by positive silver stain and expression of certain proteins, such as synaptophysin, neuron-specific enolase, and chromogranin A (CgA). Many neuroendocrine cells contain membrane-bound neurosecretory granules within which are hormones and biogenic amines such as serotonin, corticotrophin, histamine, dopamine, substance P, neurotensin, prostaglandins, and kallikrein. 4 The release of these substances into systemic circulation may cause a variety of secretory syndromes, which may present as flushing, diarrhea, wheezing, rash, or even multiorgan failure.
Epidemiology
Neuroendocrine neoplasms are rare tumors, with an incidence in the United States of 6.98 per 10 000 persons in 2012, which is an increase of 6.4-fold from 1973. The prevalence was 0.048%, increasing from 0.006% in 1993. 5 The increase of incidence and prevalence could be due to earlier detection with the increased utilization of endoscopy. A study based on the Surveillance, Epidemiology, and End Results (SEER) database showed that the age-adjusted annual incidence of NETs (per 100 000 to 2000 US standard population) arising from the rectum, jejunum/ileum, stomach, colon, duodenum, cecum, and appendix was 0.86, 0.67, 0.30, 0.20, 0.19, 0.16, and 0.15, respectively. 6
Around 20% of NETs are associated with inherited genetic syndromes. Gastrointestinal NETs are associated with multiple endocrine neoplasia type 1 (MEN1) and neurofibromatosis type 1 (NF1). The identification of a germline mutation enables genetic counseling and may be prognostic of treatment response. 7 Those with MEN1 have a higher incidence of NETs and failure to treat leads to decreased life expectancy (typically seen with pancreatic NETs and thymic carcinoids).8,9 As with non-heritable NENs, treatment depends on tumor characteristics. Most tumors <2 cm can be safely observed and followed in those with MEN1, but those that are rapidly growing or greater in size have a higher malignancy rate.10-12
Most (65%-95%) of the gastroenteropancreatic NENs show hepatic metastasis (excluding appendiceal, gastric, and rectal NETs, about 85%-90% of which are local). 13 Some patients may have metastases in both the liver and the bone. One single-institutional study showed that the spine (68%) is the most common site of bone metastases followed by pelvis (24%) and ribs (12%). The median survival was 73.3 months for patients with liver and bone metastases from GI NET. 14
Analysis of NEN survival rates from the SEER database found that the median overall survival (OS) for all NEN patients was 9.3 years in the United States. Well-differentiated tumors were found to have higher OS than moderately differentiated tumors (16.2 vs 8.3 years). The poorly differentiated, undifferentiated, and anaplastic tumors only had an OS of 10 months. 5 Rectal NETs have the best prognosis followed by tumors in the small intestine, stomach, and colon. 15 The median OS decreases with age, with patients more than 70 years old having a poorer OS (28.0 vs 233 months). Older patients often had distant (34%) or grade 3 disease (40.8%). 16 For patients presenting with metastatic NETs, 5-year survival rate is poor (19%-38%) comparing with localized NET (78%-93%). 17
Classification
Neuroendocrine tumors have previously been categorized according to embryonic origins: foregut (lung, stomach, duodenum, upper jejunum, and pancreas), midgut (lower jejunum, ileum, appendix, and cecum), and hindgut (colon and rectum) NETs. 18 The World Health Organization (WHO) separates NENs by grade to reflect tumor biology (Table 1). In 2017, the WHO updated its gastroenteropancreatic NET classification and grading system to better predict disease from tumor characteristics, including separation of poorly differentiated NENs (previously classified as G3) into 2 categories according to pathologic appearance and relabeled mixed adenoneuroendocrine carcinoma (MANEC) as mixed endocrine non-endocrine neoplasms (MINEN/MENEN). Mixed adenoneuroendocrine carcinoma was broadened to MINEN/MENEN recognizing the fact that mixed neoplasms may contain components other than adenocarcinoma. When any component other than endocrine neoplasm surpasses 30%, then it falls into the MENEN category. Most mixed tumors rise from the appendix. 19 They have the tendency to show aggressive behavior and generally have a poor prognosis. 20 The median OS for those of appendiceal origin was 6.5 vs 13.8 years for appendiceal goblet cell carcinoid (P < .0001). 21
2017 WHO Classification of GI Neuroendocrine Tumors.

Source: Adapted from WHO Classification of Tumors of Endocrine Organs, Fourth edition (2017).
Abbreviations: HPF, high-power field; MINEN/MENEN, mixed endocrine non-endocrine neoplasms; NEC, neuroendocrine carcinoma; NEN, neuroendocrine neoplasm; NET, neuroendocrine tumor; WHO, World Health Organization.
An additional classification exists for gastric NENs based on histomorphologic characteristics and pathogenesis. Gastric NETs are divided into 3 types: (1) type I are the most common subtype and associated with autoimmune atrophic gastritis; (2) type II are associated with gastrinoma/MEN-1; and (3) type III are sporadic with normal levels of gastrin, normal gastric pH, and exhibit a more aggressive behavior pattern. Type III gastric NETs tend to present with a larger size and deeper level of invasion than types I and II. Type IV gastric NET is rare, poorly differentiated and tends to be the most aggressive subtype. 22
Presentation
Patients with NETs may develop symptoms due to primary tumor invasion, metastasis, or from secretion of hormonally active tumor substances.
Site-specific symptoms
Symptoms caused by primary tumor are site specific. Gastric NETs arise from proliferating enterochromaffin-like (ECL) cells of the fundus. Patients with type I gastric NETs have anti-parietal cell or anti-intrinsic factor antibodies and present with compensatory hypergastrinemia in response to hypo/achlorhydria. Type II gastric NETs present with hypergastrinemia and excessive gastric acid secretion, which are caused by autonomous gastrin secretion via a gastrinoma. Both type I and II gastric NETs may have symptoms like gastric ulcers, bleeding gastric polyps, or gastric carcinoma. Type III and IV gastric NETs are more aggressive, presenting with features similar to gastric adenocarcinoma.
Small intestinal NETs originate most commonly from the distal ileum, presenting with paroxysmal abdominal pain and intermittent bowel obstruction. 23 Neuroendocrine tumors in the duodenum may also cause upper GI bleeding, jaundice, and/or duodenal obstruction with nausea/vomiting. 24 Neuroendocrine tumors of the colon are commonly diagnosed during evaluation for abdominal pain, anorexia, or weight loss. Typical symptoms of rectal NETs are change of bowel habit and bleeding and may masquerade as hemorrhoids.25,26
Carcinoid syndrome
Carcinoid syndrome is one of the many secretory syndromes that can occur with hormonally active tumors. It occurs in approximately 30% to 40% of patients with well-differentiated GI NETs who present with a constellation of symptoms including episodic facial flushing, diarrhea, or bronchospasm. 27 Late complications include fibrosis (carcinoid valvular disease and mesentery fibrosis) and nutritional deficiency (tryptophan and niacin). For intestinal NETs, carcinoid symptoms typically arise in the setting of liver metastases when tumor secretions are not completely metabolized by the liver and are able to enter the systemic circulation in an active form.
The pathogenesis of fibrotic complications is unclear. It was proposed that vasoactive substances such as serotonin stimulate fibroblasts and fibrogenesis.27-29 Carcinoid heart disease mostly affects the right heart, especially tricuspid valve. Patients are mostly asymptomatic in early phase and present with symptoms of right heart failure (peripheral edema, ascites, abdominal discomfort, and early satiety). 30 Fibrosis of small bowel mesentery and the peritoneum is thought to be a desmoplastic reaction to mesenteric lymph node metastasis.28,29 Peritoneal metastasis can produce local fibrosis with the consequence of mesenteric ischemia 31 and retroperitoneal fibrosis, presenting with abdominal mass and ureteral obstruction.
Normally, 99% of tryptophan is used for the synthesis of nicotinic acid and catabolically degraded into either serotonin or beta-nicotinamide adenine dinucleotide (NAD), which is an active form of niacin. Neuroendocrine tumors associated with carcinoid syndromes can use up to 60% of bioavailable tryptophan, which results in tryptophan and/or niacin deficiencies. Tryptophan deficiency is associated with neuropsychological dysfunction. Niacin deficiency leads to pellagra (dermatitis, diarrhea, and dementia). 27
Carcinoid crisis
Carcinoid crisis is a life-threatening complication characterized by the abrupt onset of hemodynamic instability which can occur with procedural intervention, treatment initiation in those with high tumor burden or high tumor hormonal activity, or spontaneously with poorly controlled carcinoid syndrome.32,33 Periprocedural carcinoid crisis is hypothesized to be related to increased hormone secretion due to tumor manipulation or anesthesia. However, a recent prospective study showed that hypotensive carcinoid crisis occurs without a measurable massive release of serotonin, histamine, kallikrein, or bradykinin, which may indicate that some other unmeasurable substance(s) may be responsible for hypotensive shock. Furthermore, the analysis of cardiac indices, pulmonary arterial pressure, and central venous pressures amid a crisis event found no evidence of cardiopulmonary cause of shock. Rather, it is mostly suggestive of distributive shock due to observed intracardiac hypovolemia and decreased systemic vascular resistance. 34 Octreotide, a somatostatin analog (SSA), has been used in both prophylactic and therapeutic capacities for carcinoid crisis. Patients are treated with long-acting octreotide prior to procedural intervention. Should the patient develop hypotension during the procedure suggestive of carcinoid crisis, they are often treated with additional octreotide boluses. However, studies looking at the utility of octreotide found that preprocedural prophylactic dosing and intraprocedural bolus (independent of dose) are insufficient for preventing intraoperative complications. 35 Continuous octreotide infusion was also tested in conjunction with prophylactic preprocedural long-acting octreotide and preprocedural octreotide bolus and was also found to be similarly insufficient in preventing intraprocedural carcinoid crisis. 36 However, prompt vasopressor use was found to shorten the duration of hypotension leading to a statistically significant decrease in major postoperative complications. 36 Currently, periprocedural octreotide is recommended because carcinoid crisis is suspected to occur secondary to massive hormone release, even if the active substance is not specifically identified, but it should be paired with fluid resuscitation and vasopressors for resuscitation during carcinoid crisis to decrease postoperative complications.34-38
Diagnosis
Imaging
Multiple imaging modalities are used for NETs, including computed tomography (CT), magnetic resonance imaging (MRI), ultrasound (US), endoscopy, and functional imaging. They are indicated for different purposes including localization, staging, assessing response to treatment, and prognostication.
Multiphasic contrast-enhanced CT is often the first modality performed and offers the highest spatial resolution (⩽1 mm). 39 Neuroendocrine tumor liver metastases show an enhancement in the portal venous inflow phase within non-enhanced hepatic parenchyma. 40 Mesenteric metastasis often shows mesenteric contraction and signs of small bowel obstruction on CT.
Compared with CT, MRI has better soft tissue discrimination and better visualization for metastases in the liver, bone, and the central nervous system (CNS).39,41 Neuroendocrine tumor liver metastases have a low signal intensity on T1-weighted sequences and a high signal intensity on T2-weighted sequences compared with the hepatic parenchyma. Early washout of contrast and ring enhancement in gadolinium-enhanced hepatic arterial phase are the distinguishing features from hepatic hemangioma.
Traditional transabdominal US has a relatively low sensitivity for NETs. With the introduction of contrast-enhanced ultrasound (CEUS), using microbubble contrast agents, liver metastases as small as 2 to 3 mm may be detected. Subcentimeter liver metastases appear as low echogenic rounded lesions, whereas larger (>1 cm) metastases are highly echogenic with a low echogenic halo and/or low echogenic central necrosis. 40 Primary NETs of the small intestine are difficult to be detected by US even with contrast. Two thirds of small intestinal NETs first present with mesenteric changes as mesenteric thickening on US. Such findings should prompt for further assessment of the small intestine with axial imaging. 42
Six human subtypes of somatostatin receptors (SSTRs) have been identified (1, 2A, 2B, 3, 4, and 5). Well-differentiated GI NETs generally have overexpression of SSTRs, especially subtype 2A.39,43,44 Positron emission tomography (PET) and single-photon emission computed tomography (SPECT) are commonly performed with CT or MRI in the diagnosis of NETs to increase sensitivity and localization. In the past, 111In pentetreotide (Octreoscan) was the mainstay functional imaging for GI NET staging. The 111In pentetreotide scan is a set of whole-body planar images, the first obtained 4 hours after intravenous injection of 111In pentetreotide (5mCi) and the second obtained 24 hours post-injection. 39 The overall positive predictive value (PPV) and negative predictive value (NPV) of Octreoscan were determined by types of NETs. For GI NETs, these scans have an associated 84.6% PPV and a 50% NPV. 45 However, PET/CT imaging with novel radiolabeled SSAs has recently replaced the Octreoscan as the new gold standard. 46 One of these molecules, 68Gallium-DOTATATE, has been shown to have a better detection rate compared with CT of primary tumor (89% vs 25%) and carcinomatosis (88% vs 75%), a higher detection rate than conventional 111In pentetreotide SPECT/CT (95.1% vs 45.3%, P < .001), 47 and a lower radiation dose due to the shorter length of study (2 hours).43,44,46-48 A study at 2 large NET referral centers found that the sensitivity, specificity, NPV, and PPV of another radiopeptide 68GaDOTANOC were 87.1%, 97.7%, 79.6%, and 98.7%, respectively. 49 A study of 20 patients with NETs of an unknown origin showed that 68Ga-DOTATATE PET/CT could have localized 60% (12/20) of occult primary tumors, changed management of 15% (3/20) patients who underwent surgery, and confirmed that 85% (17/20) of tumors were SSTR positive, thereby suggesting the suitability for peptide receptor radionuclide therapy (PRRT; discussed below). 50
18F-flurodeoxyglucose (FDG) is another functional imaging modality that measures tissue glucose transport. It has limited use in well-differentiated (G1, G2) NETs but can be valuable for high-grade (G3) NETs.41,51-54 The most common pitfall of functional imaging is the misinterpretation of physiological uptake. Small lymph nodes are the most common location of non-NET-related functional activity. 55 Misinterpretation of physiological lymph node uptake may falsely upstage a patient’s disease.44,56
Endoscopy
Endoscopy plays an important role in diagnosing NETs of the stomach, duodenum, colon, and rectum. With the popularization of endoscopy, more intestinal NETs are diagnosed. 57 It is recommended to endoscopically assess the GI tract if NET liver metastasis is of unknown origin to identify the primary tumor and rule out concomitant malignancies. 58
Endoscopic ultrasound (EUS) is commonly used for diagnostic biopsy 59 and may have an interventional role in selected cases using adjunct procedures such as radiofrequency ablation. 60 EUS also plays an important role in preoperative staging by assessing tumor size, depth of invasion, and lymph node involvement. 61 Standard endoscopy is limited by the length of the endoscope in the diagnosis of small bowel NETs. Double balloon enteroscopy (DBE) or video capsule endoscopy (CE) can be considered in these cases. The sensitivity in identifying NETs by DBE is 60% to 90%; however, the PPV is only 20% to 30%.62-64
Biochemical markers
The National Institutes of Health (NIH) classifies biomarkers into 3 categories for different functions: type 0 for natural history of a disease, type I for effects of an intervention, and type II for prognosis. 65 Current biomarkers for NETs are useful as type 0 and type I biomarkers but not sufficient in the prognosis of NETs.66,67 However, they are not mandatory to establish the diagnosis of NET. 68 Currently, 5-hydroxyindoleacetic acid (5-HIAA) and CgA are the most commonly used biomarkers for GI NETs.
Most functional NETs secrete 5-hydroxytryptamine (serotonin). 5-HIAA is the metabolic breakdown of serotonin, levels of which can be measured in 24-hour urine collections or fasting plasma. 24-hour urine 5-HIAA has a sensitivity of 73% and a specificity of 100%. 69 A study of 31 patients comparing urinary to plasma 5-HIAA levels showed that there was no significant difference between the 2 measurements; however, fasting plasma 5-HIAA concentration was more convenient. 70 A retrospective analysis of 232 patients showed that high urinary HIAA level (⩾8.1 mg/24 h) was correlated with metastasis in patients with small intestinal NETs with high PPV (81.8%) and NPV (85.7%). 71 A 5-HIAA doubling time of <434 days has been associated with a higher rate of disease-specific mortality (P = .02), whereas a shorter doubling time in small bowel or occult primary NETs was correlated with a higher risk of disease progression. 72
Chromogranin A is an acid glycoprotein present in the secretory granules of most neuroendocrine cells and high in GI NETs. 73 It is now the most widely used biomarker for evaluating NETs. The sensitivity ranges between 60% and 100%; however, the specificity is as low as 10% to 35%. Chromogranin A is elevated in other neoplasia such as breast cancer and prostate cancer and can be falsely elevated in patients with impaired kidney function or taking proton pump inhibitors (PPIs). 74 Studies have shown that the level of CgA is associated with hepatic tumor burden and that a sudden increase to >1000 U/L can be associated with rapid tumor progression and shorter survival. 74 - 76 However, CgA may not be as useful for colorectal NETs. 77
More recently, a fragment of CgA known as pancreastatin has shown potential as a biomarker for NETs. A study of 103 patients evaluated by both pancreastatin and CgA found that pancreastatin has greater sensitivity (64%) and specificity (100%) than CgA (sensitivity: 43% and specificity: 64%). 78 Moreover, another study found that pancreastatin levels were unaffected by PPI. 79 Further evaluation of pancreastatin is warranted prior to widespread clinical use.
Type II gastric NETs are caused by gastrinomas and characterized by elevated fasting serum gastrin (FSG) and low gastric pH. Thus, FSG (>1000 pg/mL) can be applied for the identification of type II gastric NETs. However, a high gastrin level can be presented in other conditions such as chronic atrophic gastritis, renal failure, Helicobacter pylori infections, and PPI use. 73 Secretin stimulation test is the gold standard to confirm gastrinoma. Normally, secretin suppresses the release of gastrin, but will paradoxically stimulate the release of gastrin in the setting of a gastrinoma.
Current biomarkers have generally not proven to be clinically very useful. Multianalyte assays with algorithmic analyses (MAAAs) represent a novel method to use multiple measurements of different parameters and algorithmically improve sensitivity and specificity. 80 The NETest is a multianalyte liquid biopsy that measures the expression of a 51-gene panel linked to pancreatic and GI NETs. 81 Using this expression profile and computational machine learning, a NET score (0-8) is derived. A value of >2 is a positive tumor score. 82 Several studies showed that NETest was more accurate in the diagnosis of GI NET than CgA (93% vs 80%).83,84 However, these studies were all funded by the manufacturer and have not been independently verified. 80 A consensus of 33 multinational experts found that NETest has strong potential for clinical use (high sensitivity > 95% and specificity > 95%). However, circulating tumor cell technology and NET-specific gene panels require validation and further clinical investigation is needed prior to widespread adoption. 85
Management
Surgical management
Stomach
The National Comprehensive Cancer Network (NCCN) guidelines recommend type I hypergastrinemic patients with tumor ⩽2 cm be treated by local resection (endoscopic resection or wedge resection). Endoscopic treatment includes biopsy, polypectomy, endoscopic mucosal resection (EMR), and endoscopic submucosal dissection (ESD). Large tumors (>2 cm) have a higher risk of invasion and metastasis and should be treated with anatomic surgical resection. Gastric antrectomy can be considered for type I gastric NET with progressive, invasive, or recurrent disease. Antrectomy can reverse G-cell-mediated hypergastrinemia, leading to regression of tumor. 86 Type II NETs should be treated with resection of gastrinoma if possible; otherwise, endoscopic surveillance, endoscopic resection of prominent tumors, PPI use, and medical management are recommended. Type III and type IV NETs are generally treated with formal (partial or total) gastrectomy and lymphadenectomy if widespread metastases are not present.
Patients with type I or II gastric NETs are recommended to follow up every 6 to 12 months for the first 3 years and annually thereafter if no evidence of progression is seen. Type III gastric NETs should follow up 3 to 12 months after resection and then every 6 to 12 months for up to 10 years. 87 A study of 187 patients showed that, for gastric NETs ⩽10 mm, removal of tumor by piecemeal biopsy, polypectomy, EMR, and ESD achieved histological resection-margin-free rates of 45.5%, 45.5%, 68.8%, and 75% for G1 lesions and 33.0%, 50.0%, 100%, and 100% for G2 lesions, respectively. For G1 tumors sized 11 to 20 mm, endoscopic-margin-free rates of EMR and ESD were 100% and 100%, respectively. 88 Another single-center cohort study of 135 patients found that patients with gastric NETs after surgical treatment had 1-, 3-, and 5-year OS at rates of 82.4%, 59%, and 44.2%, respectively. 89 A study of 79 patients identified with gastric NETs (34 type I, 4 type II, 37 type III, and 4 type IV) showed that there was no difference in recurrence-free survival (RFS) between local resection (endoscopic or surgical wedge resection) and formal gastrectomy; however, OS may have been worse in the formal gastrectomy group. 22
Duodenum
These tumors often present as single small sessile pale lesions mostly in the first or second part of the duodenum.90,91 Recommended treatment for isolated NETs arising in the duodenum is endoscopic resection, if possible. 87 Subcentimeter G1 duodenal NETs in non-ampullary locations can be treated by endoscopic resection. Periampullary NETs and duodenal NETs more than 2 cm should be considered for surgical resection. Treatment for duodenal NETs between 1 and 2 cm in size remains controversial. 92 Endoscopic resection candidacy is determined by the shape and location of the tumor, as well as endoscopic expertise. Endoscopic submucosal dissection has a better rate of complete resection but has a longer procedural time and higher complications (eg, bleeding and perforation). Surgical treatment options include local excision with or without locoregional lymph node sampling or pancreatoduodenectomy (PD). Due to the possibility of lymph node metastases, PD is the first choice for curative intent. 93
Postoperative surveillance for those with locoregional disease includes history and physical examination beginning 3 to 12 months after resection with transition to every 12 to 24 months for up to 10 years. After 10 years, surveillance is done as needed. For those with non-invasive tumors, routine endoscopic surveillance is recommended. For those with invasive tumors, multiphasic abdominal CT or MRI and CT of the chest with or without contrast are recommended during follow-up in the first year after resection with imaging as clinically indicated with surveillance visits up to 10 years. If the invasive tumor was endoscopically resected, endoscopic surveillance is additionally recommended as indicated. 87
Small intestines
The surgical goals for treatment of small intestinal NETs are (1) complete oncologic resection of primary tumors and mesenteric adenopathy; (2) intraoperative staging by evaluation of the peritoneum, liver, and ovaries; and (3) optimization of safety, operative time, quality of life (QoL), and cost. 94 More than 50% of small intestinal NETs are metastatic at diagnosis.94-96 Small bowel NET lymphatic metastases can have a skip pattern and are more likely to metastasize to retropancreatic lymph nodes than lymph nodes along mesenteric vessels and the small intestine. 95 Because of the small size, multifocal, and metastatic nature of these tumors, the North American Neuroendocrine Tumor Society (NANETS) consensus guidelines recommend exploratory laparotomy with careful palpation as a standard approach to small intestinal NETs. 94 In 1 study of 603 (493 resected) small bowel NETs, the median OS for all patients was 8.4 years. The 5-year OS for resected tumors in this study was 75% vs 28% for the unresected ones, with a major morbidity rate for resected tumors of 5.8%. 97
Appendix
The appendix is the third most common site of GI NETs, after the small bowel and rectum. 98 The NCCN recommends appendectomy for localized appendiceal tumors of 20 mm and right hemicolectomy for tumors >20 mm. Treatment for tumors between 10 and 20 mm is a point of controversy. 87 A retrospective cohort study of 916 patients with appendiceal NETs (42% managed with primary resection vs 58% with right hemicolectomy) showed that, for 10- to 20-mm appendiceal NETs, right hemicolectomy does not improve survival. It was adequate for all appendiceal NETs <20 mm to be treated with simple appendectomy. 98 However, European Neuroendocrine Tumor Society (ENET) guidelines recommend considerations of some clinical scenarios in which an oncologic resection with a right hemicolectomy ought to be considered in tumors <20 mm (Table 2). Although worse prognosis has not been proven, the clinical presentation warrants consideration of more aggressive resection while simultaneously weighing the risk of higher complication rates with a more extensive surgery.
When to consider right hemicolectomy in T1 tumors. 12
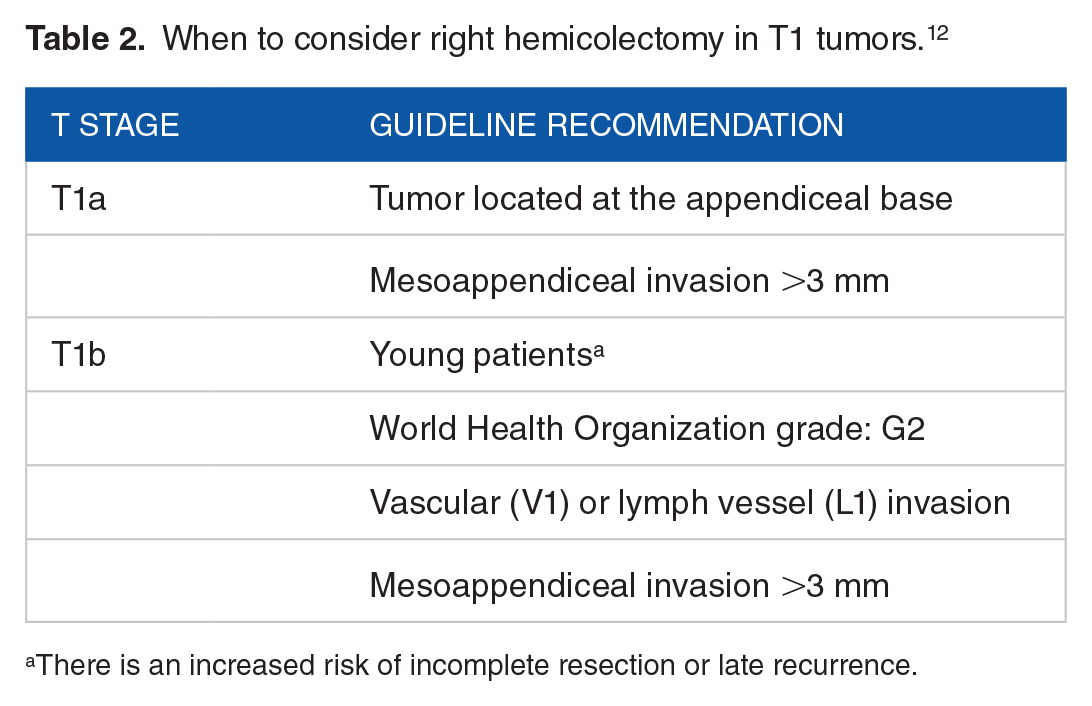
There is an increased risk of incomplete resection or late recurrence.
Finally, all appendiceal NECs (Ki-67 > 20%) should be resected with a right hemicolectomy irrespective of size and be managed as an adenocarcinoma. 99
Colon and rectum
Colonic NETs most frequently arise in the ascending colon. Colectomy with regional lymphadenectomy is recommended. 98 The survival rate at 5 years after surgical treatment is 62.7%. Vigorous surveillance post-resection is important. 100 Patients should be reevaluated 3 to 12 months after resection and then every 6 to 12 months for up to 10 years by multiphasic CT or MRI. 87
Rectal NETs ⩽10 mm are usually treated by conventional EMR, modified EMR, or ESD. Endoscopic mucosal resection is performed with a snare to grasp the target tissue and then transect the tissue with electrosurgical current with or without injection in the submucosa to lift the lesion from deeper layers. Endoscopic submucosal dissection is performed with injection in the submucosa and then dissection of the lesion from deeper layers with various specialized instruments (eg, ESD knives). 101 Several studies showed that endoscopic resection of rectal NETs has an excellent long-term prognosis.102-104
In 1 retrospective study, 181 patients with rectal NETs <10 mm were treated by endoscopic submucosal resection (ESR) with band ligation. Complete gross and microscopic resection was achieved in 180 cases (99.4%), and 77 patients out of a total of 136 patients had curative resection at long-term follow-up. 105
Endoscopic submucosal dissection has advantage over EMR of en bloc resection of lesions regardless of size and including some tumors extending into the submucosa. However, ESD is associated with a higher perforation rate compared with EMR. 101 Newer modified EMR techniques may have better outcomes than ESD. A meta-analysis of 14 studies including 823 patients showed that EMR with suction achieved a significantly higher complete resection rate than ESD for subcentimeter rectal NETs. 106 A retrospective study of 24 rectal NETs showed that there were no differences in therapeutic outcomes between EMR with ligation (EMR-L) and ESD. However, the hospitalization period was significantly shorter in the EMR-L group (1.8 ± 3.1 days) than the ESD group (6.2 ± 2.1 days). 107 Underwater endoscopic mucosal resection (U-EMR) is another novel method to overcome difficulties with resecting tumors extending into the submucosal layer. In traditional EMR, the bowel lumen is insufflated with air, which distends and thins the colonic wall, and subsequently requires a submucosal injection to decrease the risk of ensnaring of muscularis propria, resulting in colonic perforation. With U-EMR, water is used instead to fill the colorectal lumen, which keeps colonic muscularis propria circular and “floats” the mucosa and submucosa away from the deeper muscularis layer eliminating the need for submucosal injection. 108 A case report of 6 patients with rectal NETs treated with U-EMR found that 5 of 6 patients had depth of tumors in the submucosal layer. The en bloc resection rate was 100% and the R0 resection rate was 83% (5/6). The 6-month follow-up colonoscopy in non-R0 resection patients showed no residual tumor. 109
Transanal endoscopic microsurgery (TEM) may also be considered for <20-mm lesions superficial to the muscularis propria. In this procedure, a full-thickness resection can be performed transanally and the defect closed by a continuous running suture. In 1 study, 59 patients treated with TEM showed no recurrence during a median of 3-year follow-up. 110
Tumors of size between 10 and 19 mm carry a risk for metastasis and require histological examination of specimens retrieved via endoscopy for lymphovascular invasion. Formal surgical resection is recommended for tumors that are between 10 and 19 mm with high-risk features.111,112 Additional criteria for formal surgical resection for rectal NETs include tumors ⩾20 mm, positive endoscopic resection margin(s), and lymphovascular invasion in patients receiving local treatment. 112 Formal resection options include low anterior resection (LAR) and abdominoperineal resection (APR).
Surgical management of liver metastasis
The most common metastatic site for GI NETs is the liver. Of all liver NET metastases, 56% are from the small intestine. 17 Most hepatic metastases present with numerous bilobar diseases, occupying a median of 10% to 19% of the total liver volume. 113 Neuroendocrine tumor liver metastases are classified as type I (single metastasis), type II (isolated metastatic bulk accompanied by small deposits), or type III (disseminated metastatic spread). 114 Type I should be considered for surgical resection, whereas types II and III may be addressed with various modalities. 115
Hepatectomy
Liver resection is recommended the first choice for resectable G1 or G2 liver metastases with no extrahepatic disease. 13 Studies have shown that hepatectomy for NETs is safe, achieves symptom control, and extends survival. A study of 38 patients with liver-only metastases from NETs showed that patients who underwent liver resection had a higher 5-year survival (73% vs 29%). 116 Results from multiple studies have found that overall 5- and 10-year survival rates after liver resection are 60% to 70% and 35% to 42%, respectively, and that operation controls symptoms in most of the patients. A large single-institution study of 939 patients with NET liver metastases showed that hepatic resection is associated with a longer OS than chemoembolization (160 vs 66 months). 117 However, nearly all patients will recur.113,118-121 Non-anatomic resection may be associated with a higher incidence of recurrence than formal anatomic hepatectomy, but has a similar impact on OS. 122
Surgical cytoreduction
For unresectable NET liver metastases, surgical cytoreduction can be considered. 13 A retrospective study of 120 patients (79 patients with GI or unknown primary NETs) showed that surgical cytoreduction provided longer symptomatic relief (35 ± 22.0 vs 22 ± 13.6 months, P < .001) and longer survival (50 ± 27.6 vs 32 ± 18.9 months, P < .001) than embolization. 123 Selected patients may derive benefit if more than 70% of overall disease burden can be cytoreduced. 124 Liver tumor burden and extrahepatic involvement should be carefully considered in decision making of hepatic cytoreduction. 125
Liver transplantation
Liver transplantation has been offered to selected patients with unresectable NET liver metastases with no unresectable extrahepatic disease. 13 Less than 1% of patients with liver metastases from NETs are susceptible to liver transplantation. 126 With mixed results and not widely practiced, ENET guidelines do not recommend transplantation as a treatment option unless in highly selected patients with carcinoid syndrome or refractory to multiple systemic treatments. 127
Resection of primary tumor
Resection of primary tumor also has an important role in the management of NET liver metastases. Studies suggest that primary tumor resection is associated with prolonged survival across all stages (hazard ratio [HR]: 0.38-0.66, P < .01) even when metastatic disease was not removed.128,129
Management of carcinoid syndrome
Somatostatin analogs
Somatostatin analogs are the first-line treatment of carcinoid syndrome and act by inhibiting the secretion of hormones and vasoactive substances. Biological somatostatin degrades rapidly in vivo (half-life < 4 minutes). Synthetic analogs (eg, octreotide and lanreotide) are more stable (half-life of 1.7 hours) and have deposition formulations that allow for convenient every 4-week dosing.39,130
Telotristat
Telotristat ethyl (Xermelo) is a tryptophan hydroxylase 1 inhibitor, which is the rate-limiting enzyme in GI serotonin synthesis. It can be used for SSA-refractory diarrhea in patients with carcinoid syndrome. The phase 3 TELESTAR and companion TELECAST trials showed significant reductions of both urinary 5-HIAA levels and mean bowel movement frequency per day. Increases in transaminases and nausea were observed in these studies.131,132
Management of tumor progression
Somatostatin analogs
In addition to reducing bioactive substances, SSA is the first-line systemic treatment of NETs to inhibit tumor growth. The PROMID trial showed that octreotide LAR 30 mg given intramuscularly in monthly intervals inhibits tumor growth in treatment-naïve patients with metastatic G1 well-differentiated functionally active and inactive midgut NETs. Median progression-free survival (PFS) rates in the octreotide LAR and placebo groups were 14.3 and 6 months, respectively (P = .000072). 133 There was no long-term survival benefit in patients receiving octreotide LAR comparing with placebo treatment. 134 The CLARINET trial tested extended-release aqueous-gel formulation of lanreotide at a dose of 120 g against placebo in patients with advanced, non-functioning, SSTR-positive G1 or G2 (Ki-67 < 10%) gastroenteropancreatic NETs. Lanreotide was associated with a significantly longer median PFS (not reached vs 18.0 months, P < .01). 135
Targeted therapies
Everolimus is an inhibitor of the mammalian target of rapamycin (mTOR), a regulator of cell cycle and metabolism. The RADIANT-4 trial showed that everolimus significantly improved PFS over placebo in advanced well-differentiated, non-functional lung or GI NETs (11.0 vs 3.9 months, P < .00001). 136 Although everolimus has some risks for severe and life-threatening or disabling adverse events, health-related QoL is comparable to placebo. 137 In addition, the activity of everolimus is not affected by previous SSA use. 138
Vascular endothelial growth factor (VEGF) and platelet-derived growth factor (PDGF) expression occurs in NETs, especially in midgut tumors.139,140 Bevacizumab is a VEGF inhibitor, which was shown in the BETTER trial to be safe and potentially efficacious in progressive, metastatic, well-differentiated GI NETs. 141 Sunitinib is a tyrosine kinase inhibitor with activity against angiogenic factors in the hypervascularized NETs. In advanced well-differentiated pancreatic NETs, it has shown to improve PFS (11 vs 5 months, P < .001).142-145 These findings may not apply in non-pancreatic NETs. 146 Cost of targeted therapy is of concern as it is generally the most expensive systemic therapy (US$158 397/person vs US$134 912 for cytotoxic chemotherapy and US$99 691 for SSAs). 147
Cytotoxic chemotherapy
Advanced NETs (locoregional or metastatic) are often incurable. Multiple cytotoxic agents are used in the treatment of advanced diseases and treatments tend to be tailored according to pathologic grade of the tumor. Agents used include alkylating agents (streptozocin, dacarbazine, and temozolomide), antimetabolites (5-fluorouracil and capecitabine), and anthracyclines (doxorubicin and epirubicin). Multiple phase II and III trials have looked at individual agents and combinations of agents. Older studies had looked at streptozocin compared with its use in combination with 5-fluorouracil or doxorubicin. Combined therapy yielded improved response rates and median survival rates. 148 A more recent phase II/III study comparing outcomes between combined therapy of 5-fluorouracil with doxycycline or streptozocin found that there is improved survival when using a combined therapy of 5-fluorouracil and streptozocin compared with 5-fluorouracil with doxycycline. 149 In addition, a phase II trial comparing outcomes between oral capecitabine, the prodrug of 5-fluorouracil, with 5-fluorouracil infusion found comparable outcomes with a well-tolerated side effect profile (mostly diarrhea and fatigue).148-150 Irinotecan/cisplatin (IP) and etoposide/cisplatin (EP) are the most common chemotherapy regimens for progressive advanced GI NETs. 151 Several studies have shown that capecitabine combined with temozolomide (CAPTEM), 152 bevacizumab, 153 5-fluorouracil, 154 and streptozotocin 155 can be also applied in unresectable GI NETs. Given the current level of evidence of cytotoxic chemotherapy, there remains much controversy about their use. Debate remains on whether the associated toxicities of existing regimens are warranted for widespread use; however, it remains an important option for patients with no alternatives.38,87
Peptide receptor radionuclide therapy
Peptide receptor radionuclide therapy is performed by conjugating a β-emitting radioisotope to an SSA. The radiolabeled SSA can selectively target NETs by binding the overexpressed SSTRs, subsequently be internalized, thereby irradiating the tumor cells. 156 Treatment response is related to tumor expression of SSTR. Several SSA radioconjugates have been studied, including 111In-DTPA, 90Y-DOTATOC, and 177Lu-DOTATATE. 157 The NETTER-1 trial found in patients with advanced, progressive, SSTR-positive midgut NETs that 177Lu-DOTATATE with concurrent LAR octreotide had improved PFS over increased dose of LAR octreotide alone after the data cut-off date of 20 months (65.2% vs 10.8%). Neutropenia, thrombocytopenia, and lymphopenia were observed in the 177Lu-DOTATATE treatment group. 158
Interferon-α
Interferon-α (INF-α) is generally considered a last resort for patients with advanced, progressive NETs. 159 A randomized clinical trial of 65 patients with midgut NETs after surgical management or arterial embolization showed no difference in survival between patients treated with octreotide alone or the combination of octreotide and INF-α. However, INF-α significantly reduced the risk of tumor progression (HR: 0.28; 95% confidence interval [CI]: 0.16-0.45). 160 A recent phase III randomized trial by the Southwest Oncology Group (SWOG) showed no significant difference in PFS between the bevacizumab and INF-α arms; however, time to treatment failure was significantly longer in the bevacizumab group than the interferon group. 161 The common adverse effects of INF-α are fatigue and flu-like symptoms. Better tolerability of pegylated interferon (PEG-IFN) can improve patients’ compliance. 162 Despite this, low efficacy and associated adverse effects limit the use of INF-α.
Liver-directed therapy
Thermal ablation is widely achieved by radiofrequency ablation. Other energy sources such as laser 163 and cryoablation 164 have been reported to be used in the treatment of NET liver metastasis. The locally ablative techniques require laparoscopy or imaging guidance (US, CT or MRI, 163 PET/CT 165 ) of the needle/probe to the target lesion to deliver energy. 166 A study of 63 patients with NET liver metastases showed that laparoscopic radiofrequency ablation provides effective symptomatic relief (70% had significant or complete relief), however with no significant survival benefit. 167
Irreversible electroporation (IRE) is non-thermal ablation. It has the promising advantage of preserving collagenous structures (vessels and ducts) and reducing the heat sink effect. 168 A study of 65 malignant liver tumors (3 were NET liver metastases) showed that local RFS rates at 3, 6, and 12 months were 87.4%, 79.8%, and 74.8%, respectively. However, the overall complication (such as liver hematoma and liver abscesses) rate was 27.5%. 169 Further evaluations of IRE in NET liver metastases are needed.
The intra-arterial therapies (IATs) are used for liver-dominant metastatic NETs. The general goal of IATs is selective embolization of the hepatic artery branches supplying the tumor to induce ischemic necrosis. Intra-arterial therapy modalities include (1) transarterial embolization (TAE) using a bland embolizing agent, (2) transarterial chemoembolization (TACE) using drug-eluting embolizing agents, and (3) selective internal radiotherapy (SIRT) using a radiation-emitting embolization agent such as the β-emitting isotope Yttrium-90 (90Y). 166 Several studies have shown that NET liver metastases respond well to IAT.170-172 For liver metastases with large (>25%) burden, a study of 753 patients showed that patients benefit more from IAT than surgical management. 173 There is no level 1 evidence determining if IAT or surgical cytoreduction achieves better survival or QoL outcomes. 174
External beam radiotherapy
External beam radiotherapy (EBRT) is rarely used in GI NETs. A systemic review of EBRT showed that OS of patients with NET ranged from 9 to 19 months after EBRT. The radiological response rate was 46% and grade 3+ toxicity rates were 11% (acute) and 4% (late). 175 More studies should be conducted to clarify the role of EBRT in GI NETs.
Future targeted therapies
Several potential NET therapies have been identified, with some examined in clinical trials. Histone deacetylase inhibitors thailandepsin-A (TDP-A) and valproic acid (VPA) have been shown to induce Notch1 signaling in vivo. Thailandepsin-A was associated with a dose-dependent increase in Notch1-3, as well as a dose-dependent reduction in NET markers across multiple NE cancer cell lines. 161 The same authors demonstrated that TDP-A caused a 75% to 82% NET weight reduction compared with controls in a mouse xenograft model. A pilot phase II study found that VPA upregulated previously absent Notch1 signaling in all patients, with a 40× increase in Notch1 mRNA in 1 patient. Valproic acid was well tolerated and improved NET markers in 5 out of 7 patients. 162 The Raf-1 activator leflunomide (LFN), a drug that is FDA approved for rheumatoid arthritis treatment, inhibited NET growth in a mouse xenograft model and reduced levels of the NET marker ASCL1. 163
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
RW, HAC, and RZP performed the inital literature review. All authors contributed to the writing and editing of the manuscript.