
Abstract
Paraneoplastic cerebellar degeneration (PCD) is a neurological syndrome that is likely caused by tumor-induced autoimmunity against the cerebellum. Neuroendocrine carcinoma (NEC) is a type of neoplasm with high-grade malignant histology and biological behavior. The prognosis for both PCD and NEC is typically poor. We report a case of PCD secondary to metastatic NEC in the lymph nodes, with an unknown primary origin. The case presented acute cerebellar manifestations with typical neuroimaging findings, but with atypical prognosis after lymph node dissection. Neurological symptoms can provide clues to potential tumors, and early antitumor treatment may have contributed to the positive prognosis of PCD secondary to NEC in the present case.
Keywords
Introduction
Paraneoplastic neurological syndromes (PNSs) are a heterogeneous group of neurological disorders that are likely caused by tumor-associated autoimmune responses. 1 Paraneoplastic cerebellar degeneration (PCD), which is one of the most common PNSs, begins subacutely and occurs because of autoimmune damage to the cerebellum.2,3 Neuroendocrine carcinoma (NEC) is a type of highly aggressive malignant carcinoma. It has an active proliferative capacity and expresses neuroendocrine markers, such as synaptophysin and chromogranin A. 4 The prognosis for patients with NEC is extremely poor. 5 In this case report, we present a rare patient with PCD secondary to NEC with acute-onset cerebellar manifestations and a good prognosis.
Case presentation
A 48-year-old man with no medical history presented to our hospital in March 2013 with acute onset of progressive cerebellar ataxia and dizziness, which had started approximately 80 days earlier. He reported dysarthria and difficulty with ambulation. He was unable to walk without assistance on admission. He also reported an 18-day history of dysphagia and a weight loss of 5 kg from symptom onset.
The patient denied a family history of similar diseases. Physical examination revealed a severe cerebellar syndrome, including dysarthric speech, unsteady gait, bilateral vertical nystagmus, bilateral finger-to-nose and heel–knee–tibia dysmetria, bilateral dysdiadochokinesia, and a positive Romberg sign. Neither muscle weakness nor sensory damage was detected except for bilateral weakness of the soft palate. Deep tendon reflexes were normal in the upper and lower limbs. In addition, two palpable, enlarged lymph nodes measuring about 2.5 cm in diameter had been present in the right submandibular area for approximately 2 years. Based on the clinical manifestations, a diagnosis of PCD was probable, although further exclusions were required for diagnoses such as Miller Fisher syndrome, glutamic acid decarboxylase 65 (GAD65) antibody-related cerebellar ataxia, multiple sclerosis, stroke, and ataxia with vitamin E deficiency.
The results of a routine blood test, biochemical examination, and tumor biomarkers were generally unremarkable, except that the patient’s neuron-specific enolase was 12.8 ng/mL (normal values: 0–12.5 ng/mL). A lumbar puncture was performed, and cerebrospinal fluid (CSF) analysis revealed a normal leukocyte count, a protein level of 1144 mg/L (normal: 150–450 mg/L), and negative oligoclonal bands. Onconeuronal antibodies, including anti-Hu, anti-Yo, anti-Ri, anti-Ma2, anti-crossveinless-2 (CV2), anti-amphiphysin, anti-Tr, anti-ZIC4, anti-sex determining region Y-box 1 (SOX1), anti-recoverin, anti-titin, and anti-GAD65, were measured by immunoblotting and were not present in the serum or CSF. Brain magnetic resonance imaging (MRI) displayed marked cerebellar atrophy (Figure 1). Electroencephalography, electromyography, nerve conduction velocities, chest computed tomography (CT), and thyroid ultrasonography were normal. A positron emission tomography/computed tomography (PET/CT) scan showed that the atrophic cerebellum had diffusely reduced 18F-fluorodeoxyglucose (FDG) metabolism, and that the two enlarged right submandibular lymph nodes had abnormally high 18F-FDG metabolism (Figure 2). The patient then underwent an ultrasound-guided biopsy of the enlarged lymph nodes, and the pathological diagnosis was metastatic NEC with a high proliferation rate (Ki-67 index >90%) (Figure 3). To find the origin of the metastasis, a bronchoscopy, nasal endoscopy, gastroscopy, and colonoscopy were all performed, but no primary tumor was identified. Based on these findings, the patient was diagnosed with PCD secondary to NEC.

Brain magnetic resonance T2-weighted imaging showing marked cerebellar atrophy (arrow).
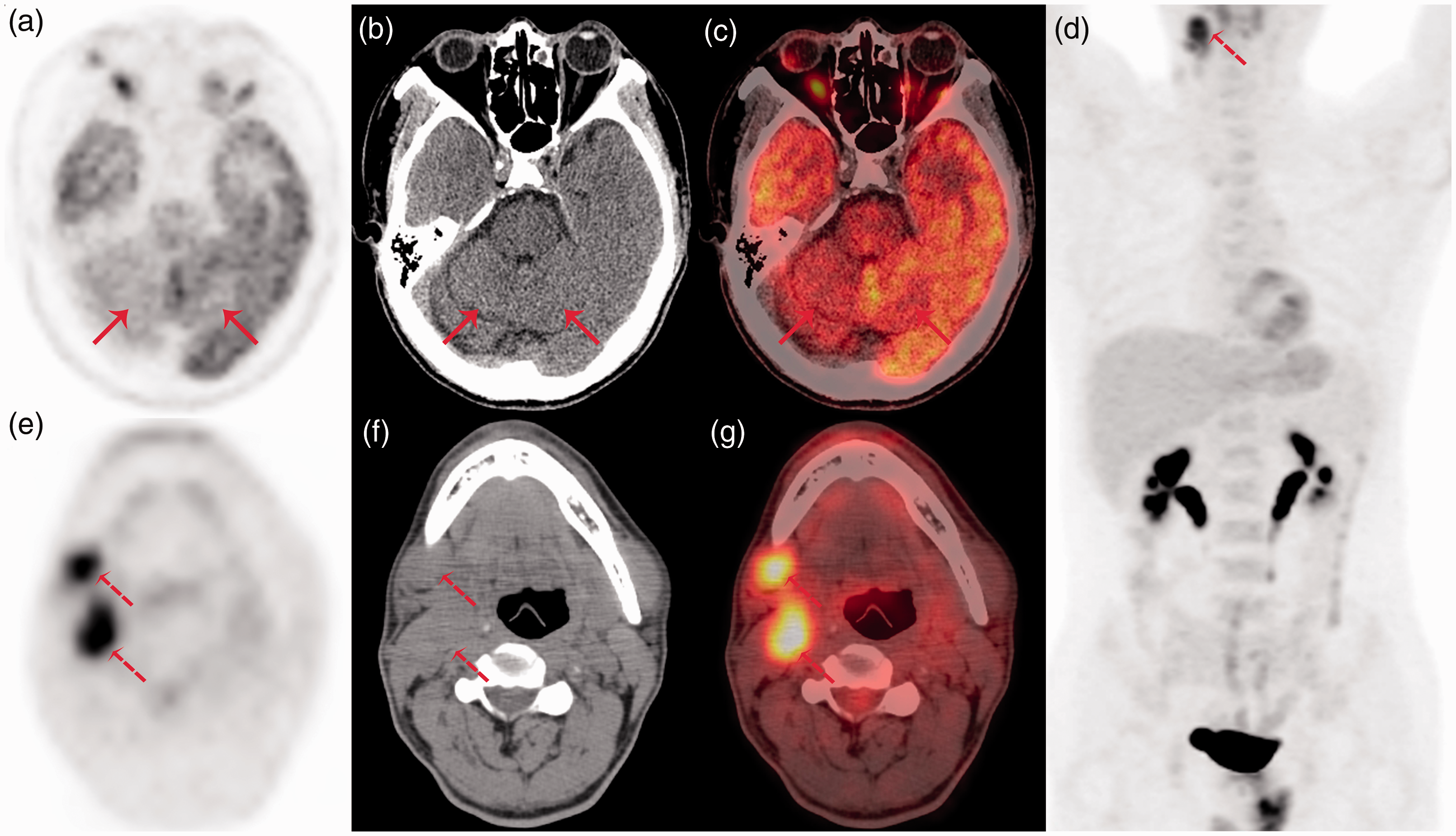
18F-fluorodeoxyglucose positron emission tomography (PET)/computed tomography (CT) scans. (a–c) Scans showing that the atrophic cerebellum had diffusely reduced metabolism (solid arrows). (a) PET; (b) CT; (c) fusion. (d–g) Scans showing that two right submandibular lymph nodes had abnormally increased metabolism (dashed arrows). (d) and (e) PET; (f) CT; (g) fusion.

Histological and immunohistochemical findings of the two enlarged right submandibular lymph nodes. Hematoxylin and eosin staining showing nests of small cell carcinoma (a). Immunohistochemical staining showing that carcinoma cells were positive for synaptophysin (b) and chromogranin A (c). The Ki-67 index was more than 90% (d). The original magnification was ×200. Scale bar = 100 µm.
The patient then underwent a radical right neck dissection, and pathological examination via cryosection was performed. Of 32 cervical and one submandibular lymph nodes, two cervical lymph nodes were positive for metastatic NEC (Ki-67 > 90%); these lymph nodes were removed. The patient’s neurological symptoms were gradually relieved within 1 week after the operation. The patient was discharged with mild dizziness and dysarthria. At discharge, he was able to walk very slowly unassisted, and his symptoms of dysphagia and nystagmus had disappeared. Over a follow-up period of 7 years without further treatment, a brain MRI, chest CT, and abdomen CT were performed every 6 months. No indication of a tumor was found, and the patient’s neurological symptoms did not progress.
Discussion
PCD is an uncommon neurological syndrome that results from tumor-induced autoimmunity against the cerebellum. It is characterized clinically by progressive cerebellar deficits with a subacute onset, with symptoms and signs that include dizziness, ataxic gait, dysarthria, and nystagmus, which present over several weeks.6,7 In addition, symptoms of dysphagia, diplopia, and cognitive and psychiatric morbidity have also been noted.8,9 The proportion of patients with acute onset—as occurred in our patient—is small, occurring in 8.3% of patients according to a recent retrospective analysis. 10 Early on, brain MRI in PCD is usually unremarkable, with later stages showing cerebellar atrophy. An 18F-FDG PET/CT scan shows a reduced mean metabolic rate in the cerebellum. 7 Onconeuronal antibodies in either the serum or CSF are significant indicators of tumors and primary tumor-related sites. 11 However, an absence of antibodies is not sufficient to rule out PCD. In the present case, based on the typical clinical manifestations consistent with PCD and tumor and the typical neuroimaging results, a diagnosis of PCD was suspected immediately. The pathological biopsy from the enlarged submandibular lymph nodes indicated metastatic NEC. We therefore diagnosed definite PCD according to the diagnostic criteria for PNSs, established in 2004. 11
The gastrointestinal tract, pancreas, and lungs are the most frequent sites of NEC, but the primary origins are unknown in 41.3% of patients with NEC.5,12 In addition, although PCD can be secondary to any cancer, the vast majority of cases result from gynecological or breast cancers, small cell lung cancer, or Hodgkin’s disease.13–15 Based on the drainage area of the submandibular lymph nodes, the typical sites of NEC, and the common cancers to which PCD is secondary, endoscopies for related organs were performed for this patient. However, no tumor was identified.
No evidence-based guidelines are currently available for the treatment of PCD because of its extremely low prevalence. Three major therapies have been used clinically: modulation of autoimmunity by immunosuppression (corticosteroids) or intravenous immunoglobulin G; removal of antibodies by plasma exchange; or antitumor therapy via surgery or chemotherapy. 13 One study has suggested that antitumor therapy is the only successful approach for improving neurological outcomes in patients with PNSs. 16 Recently, both a case of PCD and a case of autoimmune encephalitis have been reported with remarkable and unexpected improvement following antitumor treatment.17,18 In the present case, although the primary origin of the metastasis was not identified, a radical right neck dissection surgery was performed based on the limited literature, the advice of otorhinolaryngology head and neck surgeons, and our own experience. The neurological symptoms of our patient were alleviated after the surgery. The mechanism of the therapeutic effect may be that removal of the antigenic stimulus by surgery resulted in the cessation or reduction of the damaging autoimmune attack against the cerebellum. 16
Neuroendocrine neoplasms are divided into well-differentiated neuroendocrine tumors and NEC with high-grade malignant histology and biological behavior. 4 The mean survival of NEC is 1.2 years. 5 It was therefore unexpected that our patient remained alive, without a worsening of his neurological symptoms, during 7 years of follow-up. With early diffuse neuronal loss in the cerebellum, a late improvement in symptoms is rare. 19 To the best of our knowledge, no cases of PCD secondary to NEC with a better prognosis or longer follow-up time than our patient have been previously reported. 20 Acute onset and a rapid improvement of symptoms after lymph node dissection are not conventional characteristics of PCD. It is therefore important to elucidate atypical presentations. Good performance status, normal levels of platelets and lactate dehydrogenase, and antitumor surgery without delay may be factors that contributed to the positive outcome in our patient. 21 We continue to follow the patient closely.
In summary, this report presents a case of PCD secondary to NEC with a good prognosis and an extended follow-up. This case study indicates that special attention should be paid to patients’ neurological symptoms because they may suggest the existence of potential tumors.
Footnotes
Ethics statement
This report was approved by the Ethics Committee of Sixth Medical Center of Chinese PLA General Hospital, and the patient has provided informed consent.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by the New Technology and New Business Fund (No. HZXJS[2018]-10).