
Abstract
Acute exacerbations of chronic obstructive pulmonary disease (AECOPD) are the most devastating events in the course of the disease. Our aim was to investigate the value of early warning scoring systems: National Early Warning Score (NEWS) and Modified Early Warning Score (MEWS) in AECOPD. This is a prospective observational study of patients with AECOPD who were admitted at hospital. The NEWS and MEWS scores were registered at admission (NEWS-d1, MEWS-d1) and on the second day (NEWS-d2, MEWS-d2). A nasopharyngeal and sputum sample was taken for culture. Follow-up was done at 3 and 6 months after hospitalization. Any possible correlations between NEWS and MEWS and other parameters of COPD were explored. A cohort of 64 patients were included. In-hospital mortality was 4.7% while total mortality at 6 months was 26%. We did not find any significant correlation between in-hospital mortality and any of the scores but we could show a higher mortality and more frequent AECOPD at 6 months of follow-up for those with higher NEWS-d2. NEWS-d2 was associated with higher pCO2 at presentation and a more frequent use of NIV. Higher NEWS-d1 and NEWS-d2 were predictive of a longer hospital stay. The presence of pathogens in the nasopharyngeal sample was related with a higher reduction of both scores on the second day. We therefore support the superiority of NEWS in the evaluation of hospitalized patients with AECOPD. A remaining high NEWS at the second day of hospital stay signals a high risk of hypercapnia and need of NIV but also higher mortality and more frequent exacerbations at 6 months after AECOPD.
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the leading causes of morbidity and mortality worldwide with an increasing prevalence and burden of disease over time. 1 COPD is considered a significant public health challenge since it is regarded as a preventable and treatable disease. Acute exacerbations of COPD (AECOPD) are the most devastating events of the disease leading to disease progression, contributing to morbidity and mortality in COPD, impairing quality of life and also causing a high burden on health care systems.2,3 Risk factors for exacerbations include severity of underlying COPD and frequency of previous exacerbations, the presence of co-morbidities, dyspnoea severity, malnutrition, low socioeconomic status, smoking and higher age.4‐7
AECOPD can be precipitated by several factors. The most common causes appear to be respiratory viral infections and in this case exacerbations tend to be more severe and last longer. 1 Bacterial infection and other environmental factors such as pollution, are also well recognized risk factors for AECOPD.8,9 Impaired mucociliary clearance, damaged epithelium and impaired function of airway immune cells such as neutrophils and alveolar macrophages that is well described in COPD, are factors contributing to bacterial infection which can further escalate inflammation in the airways and lead to AECOPD. 10
Bacteria are isolated from sputum in up to half cases of AECOPD with Haemophilus influenzae, Moraxella catarrhalis, and Streptococcus pneumonia, being the most prevalent, while Pseudomonas aeruginosa is more often found in patients with most severely impaired lung function and requires specific antibiotic treatment. 10 Whether isolation of a potential pathogen represents simple colonization or a real respiratory infection causing the AECOPD remains a controversial topic. However, studies have shown more frequent isolation of pathogens during AECOPD than in patients with stable COPD, indicating a pathogenic role of bacteria at least in a proportion of AECOPD.11,12 The rational for sputum collection is to identify respiratory tract infection and of course its sensitivities to antibiotics. The upper respiratory tract, especially the nasopharynx and the mouth, is densely colonized by a large variety of bacteria and a number of these bacteria have a potential pathogenic role when they move into the lower respiratory tract by micro-aspiration of secretions. 10 While sputum samples are often the first-line investigation used in the identification of infectious causative factors of AECOPD, the role of pathogens from nasopharyngeal samples during AECOPD has not been widely investigated with the most studies on upper respiratory tract infections and COPD exploring the role of viruses.13‐15
The severity of AECOPD is highly variable. Severe exacerbations implicate that the patient requires hospitalization or other utilization of emergency department resources, and they may also be associated with respiratory failure. 1 AECOPD constitute one of the most common medical conditions at emergency, internal medicine and pulmonary departments alike. Early recognition of severe AECOPD or associated acute medical deterioration is crucial. This can often be detected by recognition of changes in physiological parameters such as pulse, blood pressure, respiratory rate and temperature. By recognizing these changes in time, adverse events and death may be prevented. 16
The Early Warning Score (EWS), and the later developed National Early Warning Score (NEWS), are based on different physiological parameters (vital signs) and are validated assessment tools designed for easy use in various medical settings such as pre-hospital, acute medical unit and in-hospital settings in order to identify acute illness severity or a deteriorating condition and help nursing staff detect critical illness that require an urgent intervention. 17 Higher scores indicate the need for escalation of medical monitoring and possible clinical intervention. A modification of NEWS in 2017 called NEWS2, included a second oxygen saturation score for hypercapnic respiratory failure to ensure the most appropriate prescription of supplemental oxygen treatment, when required. 18 The Modified Early Warning Score (MEWS) is a five scaled assessment tool which was developed for the purpose of early identification of patients in need of a higher level of care and those at risk of complications and death.19‐20 Both NEWS and MEWS have generally shown favourable results in various endpoints. They have been used in several medical settings such as sepsis, acute trauma, surgical conditions, acute heart disease and more recently COVID-19.21‐27 Predictor scoring systems have been used to assess AECOPD to a lesser extent while their prognostic value during AECOPD is not clearly determined.28‐32
We hypothesized that the early warning scoring systems NEWS and MEWS would correlate with the severity and the mortality from AECOPD and we further supposed a superior role of the NEWS score in these correlations given its inclusion of oxygen saturation. The aim of this study was therefore to investigate the value of NEWS and MEWS in the prognosis of AECOPD and more specifically to explore any possible correlations between NEWS and MEWS and other parameters of COPD severity both at stable state and during an AECOPD. We further aimed to examine the eventual superiority of one of the scores for this patient group. Finally, we intended to explore any correlation between the early warning scoring systems and the presence of pathogens in the nasopharyngeal and sputum samples, thus the microbiological profile in the AECOPD.
Material and Methods
Study Design and Participants
This is a prospective observational study. Patients were recruited from Vrinnevi hospital in Norrköping, Sweden from January 2019 to January 2021. The COVID-19 pandemic affected and slowed the recruiting procedure. The study population consisted of adult patients with an established COPD diagnosis confirmed by spirometry regardless of COPD stage that visited the emergency department and were admitted to in-hospital care for at least 24 hours with an AECOPD diagnosis. Patients who were diagnosed with another cause of deterioration of COPD such as pneumonia, pneumothorax, pleural effusion, pulmonary embolism, heart failure, myocardial infarction, pericardial effusion and cardiac arrhythmias were excluded. Patients who were tested positive for COVID-19 were not included.
The study was approved by The Swedish Ethical Review Authority, registration number 2018/304-31. A written and informed consent was obtained from all participants.
Clinical Assessment
Patients were evaluated according to routine hospital clinical assessment upon arrival at the emergency department. Physiological parameters (vital signs) were taken by nursing staff at arrival also according to the hospital protocols. Radiology (X-ray or CT thorax), electrocardiogram (ECG) and necessary laboratory investigations were taken after medical evaluation.
For patients with a prior COPD diagnosis and a clinical presentation compatible with AECOPD a nasopharyngeal sample was taken at presentation for culture and in some cases nasopharyngeal swabs were analysed for influenza A, influenza B virus and respiratory syncytial virus (RSV) depended on seasonal epidemiology and hospital infectious protocols. All patients with respiratory symptoms were examined for SARS-CoV-2 during the pandemic according to regional recommendations. The patients were also asked to give at least one sample of spontaneously expectorated sputum for microbiological evaluation at the first day of admission and as soon as possible. Sputum specimens not fulfilling the criteria for suitability for bacterial cultures were not included in the analysis. 33
The most common laboratory tests included haemoglobin, white blood cell count, creatinine, C-reactive protein (CRP), albumin, pro-B-type natriuretic protein (NT-proBNP) as well as arterial blood gas analysis in order to detect hypercapnia. Specific blood tests were not a requirement within the study protocol.
When other diagnosis than AECOPD could be excluded with certainty, the patient entered the study. Physiological parameters were re-evaluated by nursing staff the next day according to medical protocol approximately 24 hours after the initial scores. Regardless of the study protocol, physiological parameters were evaluated according to medical instructions for all these patients. The physiological parameters were then evaluated by a study physician and were interpreted as NEWS (7 simple physiological parameters: respiration rate, oxygen saturation, supplemental oxygen, systolic blood pressure, heart rate, level of consciousness or new confusion, temperature) and MEWS (5 physiological parameters: respiration rate, heart rate, systolic blood pressure, temperature, level of consciousness or new confusion) regardless of the already registered scores from regular nursing staff. The NEWS and MEWS score at presentation (day 1) at the emergency department was called NEWS-d1 and MEWS-d1 respectively while the NEWS and MEWS from the next day (day 2 of hospital stay) were referred as NEWS-d2 and MEWS-d2. The difference between NEWS-d1 and NEWS-d2 was calculated and called as N1N2D while the difference between MEWS-d1 and MEWS-d2 was named M1M2D. NEWS saturation SpO2 Scale 2 (NEWS2) was not implemented.
Data Collection
The patient`s medical records were reviewed at the end of the hospital stay by study-associated physicians in order to ensure the diagnosis of AECOPD and to register the following parameters: demographics and co-morbidities, previous spirometry values, regular medication for COPD, previous exacerbations in the last 2 years, mMRC (modified Medical Research Council) dyspnoea scale and COPD Assessment Test™ (CAT) if they were available in the last 6 months, outcome and duration of hospitalization, biochemical markers, medication, need of oxygen treatment, HFNC (high flow nasal cannula) or non-invasive ventilation (NIV), ICU (intensive care unit) admission. The above information was also confirmed by the patient interviews. The results of the nasopharyngeal and sputum samples were also documented.
Follow-up
Follow-up was conducted after 3 and 6 months by re-evaluation of electronic medical records or phone-contact. Mortality at 3 and 6 months as well as frequency of new exacerbations at respective time intervals were registered.
Statistical Method
The R-language was used for all calculations and visualizations. 34 Demographic data and clinical characteristics are presented as mean with standard deviation (SD) for normally distributed continuous variables, median with interquartile range (IQR) for non-normally distributed continuous variables, and absolute value with the percentage for categorical variables. Parameter normality was evaluated using the Anderson–Darling test for normality. Statistical significance of the association between two or more numerical parameters and/or factors across one or more groups was performed with regression analysis. Statistical significance of numerical parameters compared across two groups was performed with the parametric t-test if the parameters were normally distributed and with the non-parametric Wilcoxon test if the parameters were non-normally distributed. Comparison pairs with the largest absolute Pearson correlation coefficient (r) were considered the winners. Statistical significance of factors compared across two or more groups was performed with the parametric the Fisher exact test.
Results
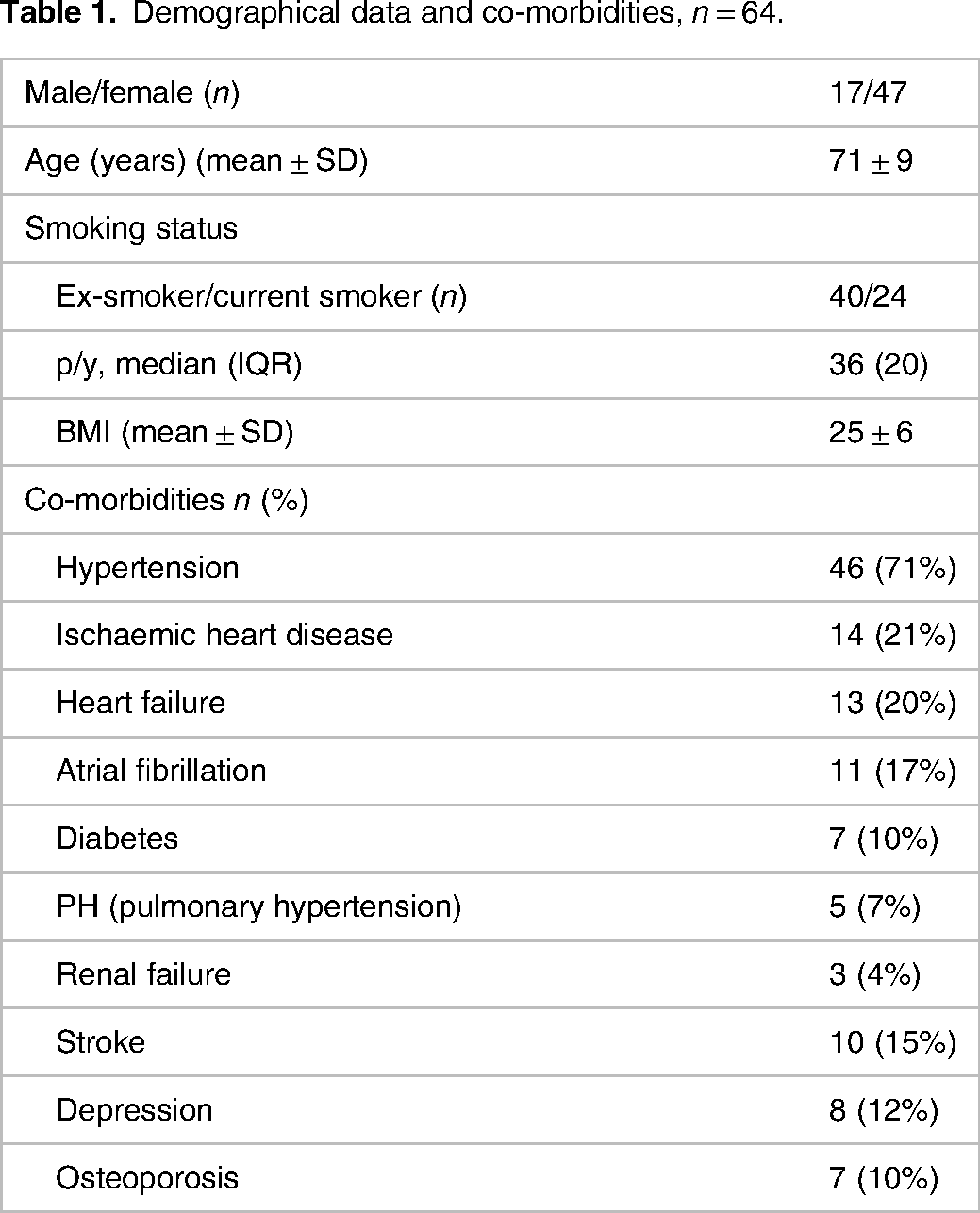
The population studied comprised of 64 patients. The demographic and clinical characteristics of the study population at baseline are given in Table 1. Mean age was 71 ± 9 years (mean ± SD) while 73% were women. The most common co-morbidity was hypertension (71%) followed by ischaemic heart disease (21%). A fairly large number of patients were current smokers (37%) (Table 1). Only 3 patients had no exacerbations in the last 2 years (both home and hospital treated) before the current hospitalization, while the majority had approximately 3 exacerbations the last 2 years (Table 2). Half of the population suffered from chronic bronchitis. Mean FEV1% was 36 ± 13 (mean ± SD). Other characteristics of COPD status at baseline inclusive medications are listed in Table 2.
Demographical data and co-morbidities, n = 64.
COPD characteristics at baseline, n = 64.

Table 3 shows the parameters that were assessed under the hospitalization period. The early warning scores are also shown in Table 3. Median CRP was 12 (42) mg/L while NT-proBNP was examined in 41 patients with a median value of 445 (1297) ng/L. All the patients had undergone either X-ray or CT thorax without signs of pneumonia or other acute pathological condition. The nasopharyngeal sample was positive in a quarter of patients (5 Haemophilus influenza, 5 Moraxella catarrhalis, 2 Streptococcus pneumonia, 3 with influenza A virus and 1 influenza B virus). A high proportion of patients were though not able to give a sputum sample for examination (39%). A sputum sample was obtained from 39 patients with a positive result in 10 patients (Table 3). The most common pathogen was Haemophilus influenza (7 cases) followed by Moraxella catarrhalis (2 cases) and Streptococcus pneumonia (2 cases). In one patient both Haemophilus influenza and Streptococcus pneumonia was cultured.
Hospitalization characteristics and EWS, n = 64.

Almost all patients were treated with corticosteroids and antibiotics (Table 3). Twenty-three patients needed NIV because of respiratory acidaemia and 8 received HFNC. Only 2 patients were admitted in the ICU (Table 3). Table 4 shows the outcome of hospitalization and the 3 and 6 months follow-up as well. In-hospital mortality was 5%. The median length of hospital stay was 5 days. At 3 months of follow-up 9 patients had died while at 6 months 5 additional patients had died. The rate of the new exacerbations at 3 and 6 months of follow-up is also shown in Table 4. A higher number of exacerbations at 6 months of follow-up was correlated with a lower FEV1% (P = 0.03).
Hospitalization outcome, 3- and 6-month follow-up outcome.

Table 5 shows the study parameters which had at least one significant correlation with any of NEWS and MEWS scores, the p value and the Pearson correlation coefficient is also given. Higher BMI was correlated with higher NEWS-d1 score. A higher CRP was related to a higher NEWS-d1 and MEWS-d1 and also a higher N1N2D and M1M2D. A lower pH in the blood gas analysis was found significantly related with NEWS-d2. A higher pCO2 at presentation at the emergency department was found significantly related to high NEWS-d2 score (Figure 1), low N1N2D and even M1M2D, with NEWS-d2 having the strongest relation to pCO2 (winner). Both NEWS-d1 and NEWS-d2 but not MEWS-d1 or MEWS-d2, were correlated with a longer hospital stay, with NEWS-d2 having the strongest correlation (Figure 2A). Higher NEWS-d2 and MEWS-d2 were also associated with a more frequent need of NIV at hospital (Figure 2B). In addition, N1N2D was lower for patients who needed NIV during their hospital stay while a longer period of NIV use was related to lower N1N2D as well, indicating a stable clinical status at the second day of hospitalization without improvement. We did not find any significant relation between NEWS and MEWS and in-hospital mortality, but we could verify a higher mortality rate and more frequent recurrent AECOPD at 6 months of follow-up for those who had a higher NEWS-d2 score (Figure 3A and B).

Scatter plot showing that higher pCO2 at presentation at the emergency department was significantly related with higher NEWS-d2 (P < 0.001).

(A) The duration of hospital stay was best correlated with NEWS-d2 (P = 0.002), scatter plot. (B) Higher NEWS-d2 was also associated with a more frequent need of NIV at hospital (P < 0.001), violin plot.

(A) Violin plot showing that a higher mortality rate within six months after AECOPD was correlated with higher NEWS-d2 score (P = 0.008). (B) Higher NEWS-d2 was associated with more frequent acute exacerbations at 6 months of follow up as well (P = 0.03), scatter plot.
The significant correlations of NEWS and MEWS scores with the study parameters.
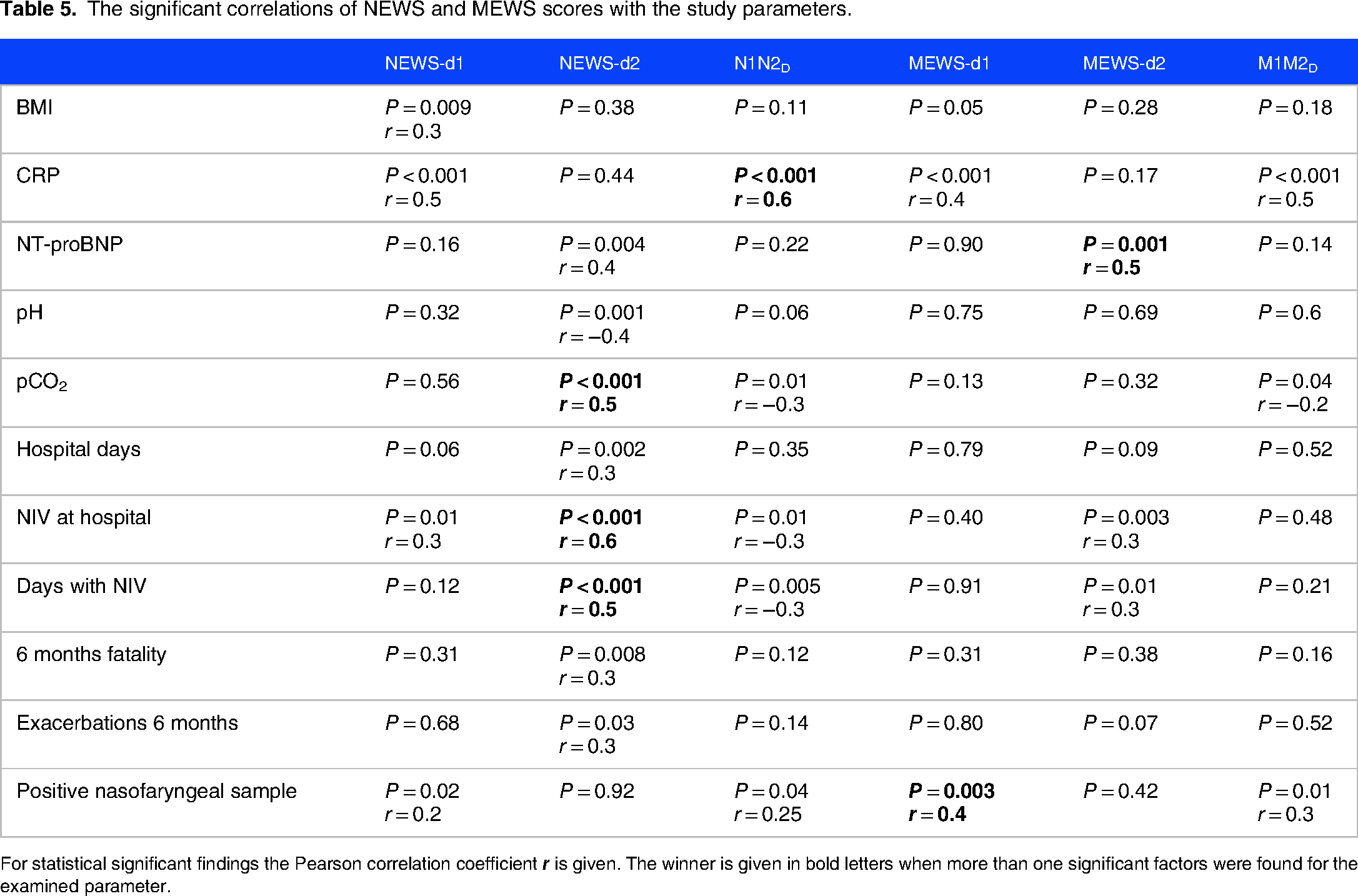
For statistical significant findings the Pearson correlation coefficient
The presence of pathogens in the nasopharyngeal sample was most significantly associated with a higher MEWS-d1 score, but also with a higher NEWS-d1, N1N2D and M1M1D (Table 5), while no association was found between a positive sputum culture and any of the scoring systems. A positive sputum culture was also correlated with higher survival rate at 3 months of follow-up while those who could not give a sputum sample had a higher mortality risk at 3 months (Fisher exact test, P = 0.04). We found no association between the presence of pathogens in the nasopharyngeal and sputum samples and the in-hospital mortality, the duration of hospital stay, the need of NIV or ICU care (data not shown). We further analysed the relationships between the pathogen profile of nasopharyngeal and sputum samples and other COPD parameters. We found a significant positive correlation between CRP and a positive nasopharyngeal sample (P = 0.004). No correlation could be seen between COPD severity based on the spirometry values and the patient´s microbiological profile (data not shown).
Discussion
In this study we aimed to examine the usefulness of the early warning scores NEWS and MEWS in the prognosis of AECOPD. We did not find any significant correlation between in-hospital mortality and any of the scores but we could show a higher mortality rate and more frequent new acute exacerbations at 6 months of follow-up for those who had a higher NEWS score on the second day of hospital stay (NEWS-d2) during an AECOPD. NEWS-d2 was also associated with higher pCO2 at presentation in the emergency department and a more frequent need of NIV during hospitalization. Higher NEWS at presentation and on the second day as well was predictive of a longer hospital stay in contrast with MEWS. In addition, the higher the CRP at presentation, indicating an infectious profile of the acute exacerbation of COPD, the higher the NEWS and MEWS were at presentation but also a bigger difference between both scores on the second day was seen, which implicates a faster response to therapy for infectious exacerbations. The presence of pathogens in the nasopharyngeal sample was related with a higher difference of both scores at the second day as well while notably, a high proportion of the population studied were not able to give a spontaneously sputum for culture. Interestingly, those with microorganisms in sputum had a higher survival rate at 3 months of follow-up in contrast to those who were not able to expectorate sputum. Neither NEWS nor MEWS were correlated with the patient´s latest spirometry values, therefore the severity of lung function impairment.
AECOPD are classified as severe when the patient requires hospitalization or visits the emergency department while acute respiratory failure is a frequent manifestation. 1 Mortality in the following months after a severe AECOPD is quite high with studies showing up to 13% mortality at 6 months and 26% at 1 year after hospitalization.35,36 In our study we found a high total 6-month mortality of 27% which we can relate to the severe impairment of lung function of this study population with a mean FEV1% of 36% and the history of frequent previous exacerbations.37‐39 Our population consisted mostly of women which can reflect the increased prevalence of smoking among women in Sweden compared with other countries. 40 In the study of Lisspers et al. conducted in Swedish COPD patients, women had a greater risk of COPD-related hospitalizations than men but no difference for mortality due to COPD was seen between genders over the study period. 40 Other studies have also showed that female COPD patients are more prone to have severe exacerbations and a higher number of hospitalizations.41,42 In a large European COPD Audit of hospital-admitted COPD exacerbations it was found that higher age, co-morbidities, the presence of acidotic respiratory failure at presentation and subsequent need of ventilatory support were risk factors associated with high in-hospital and post-discharge mortality, while COPD readmission risk was associated with the history of previous admissions. 5 The mortality rate during the observational period of 90 days was around 11% with barely half of them dying in hospital. The spirometry GOLD stage was not found predictive of mortality, though only the half population studied had available spirometry variables on admission. 5 A systematic review and meta-analysis investigating the all-cause hospital readmission following hospitalization for exacerbation AECOPD identified co-morbidities, previous exacerbations and increased length of stay as major risk factors for both 30- and 90-day all-cause readmission. 43 In a recent study on prognostic markers for AECOPD, the diffusing capacity of the lung for carbon monoxide (DLCO) but not FEV1 was associated with mortality. 44 Our population had both high rate of co-morbidities and frequent previous exacerbations of COPD which can also explain the high mortality rate, though the investigation of mortality risk factors in the AECOPD was not among the aims of this study.
The purpose of introduction and application of the early warning scores is to ensure the timely identification of deteriorating patients in order to provide the appropriate management in general hospital wards but they later proved to be mortality prognostic markers for various medical conditions as well. 45 The concept of EWS was introduced in the late 1990s when routinely measured physiological measurements were used for bedside evaluation. 46 Their role has nowadays been expanded in the pre-hospital ward as a rapid and simple triage method to identify high risk patients who are in need of hospital admission where clinical judgement alone has shown a low sensitivity for severe disease in the pre-hospital level.19,27,47 To date, EWS are internationally widely used in several medical situations and units such as the emergency departments, acute medical units, cardiac, medicine and also surgical care units, although not to the same extent worldwide, with a limited application in low-income countries. 48 In addition various algorithms on scoring of vital signs are used composing the different early warning scoring systems with NEWS and MEWS being among the most frequently used. 49 In a recent study on the predictive value of NEWS in septic patients with community-acquired pneumonia in emergency department, a score of NEWS ≥9 were strongly associated with the 28-day mortality, ICU admission and mechanical ventilation. 24 In the COVID-19 era, in a study exploring the prognostic value of the MEWS for in-hospital mortality among older adults with COVID-19, MEWS was shown an efficient tool for predicting in-hospital mortality, while in another study MEWS calculated at emergency department triage was shown effective in predicting 28-day mortality in patients requiring hospitalization due to COVID-19.26,27 An observational study of acutely dyspnoeic patients presenting at the emergency department, showed that NEWS on arrival correlated closely with the need of treatment in ICU, need of mechanical ventilatory support and short- and long-term survival as well. 28 The main limitation of EWS is their intermittent and user-dependent nature. 50 Furthermore, the validation and comparison of different EWS has been difficult to perform and interpret because of a great variation across EWS studies in different patient groups and medical settings.49,51
Different early warning systems have been evaluated in exacerbations of COPD.28–32 The DECAF score (dyspnoea, eosinopenia, consolidation, acidaemia and atrial fibrillation) measured at the time of hospital admission was shown to predict in-hospital mortality in patients with AECOPD. 32 However, the inclusion of pneumonic consolidation can be confusing in the diagnosis of AECOPD and additionally, in-hospital mortality rate of pneumonic AECOPD has been shown significantly higher than non-pneumonic AECOPD.6,35,52,53 Furthermore, blood eosinophil count is not a routine biochemical test for patients with AECOPD. In the study of Murphy et al., 60 AECOPD related in-hospital deaths were reviewed and EWS consisting of 6 physiological parameters (heart rate, systolic blood pressure, respiration rate, temperature, level of consciousness, urine production) was shown independently predictive of mortality. 30 Several years later, Hodgson et al. evaluated the prediction of in-hospital AECOPD mortality over a 2-year study period by NEWS at admission by 7 parameters (respiration rate, oxygen saturation, supplemental oxygen, systolic blood pressure, heart rate, level of consciousness, temperature) and even with 2 additional scores adjusted for patients with COPD and chronic hypoxia (the Chronic Respiratory Early Warning Score (CREWS) and the Salford-NEWS) compared with unselected patients admitted to acute medical units. 31 The study showed that the adjusted for COPD scores were not superior compared to NEWS as predictors of mortality on admission. In addition, a cut-off level of 5 points in NEWS was rather predictive of survival but not mortality. The authors argue that assigning lower oxygen saturation thresholds for scoring can potentially result in the risk of improper categorization. This issue was also addressed by Smith et al. stating that the adjusted SpO2 scale 2 (NEWS2) might be applied in error to other patient groups highlighting the need for further exploration of NEWS2. 54 Another argumentation on the above topic is that the adjusted NEWS2 should be restricted to patients with a confirmed either current or prior hypercapnic respiratory failure and moreover the decision to use NEWS2 should be made by a competent clinical decision maker while in all other circumstances the regular NEWS should be used. 55 However, this presupposes that an adequate clinical assessment should be done even by the ambulance or the triage staff which is not always feasible. Furthermore, the access to the patient’s medical record is not always possible at the initial evaluation especially in countries where electronical medical records are not available. One can also assume that the use of different scoring systems in the same medical environment can potentially lead to misunderstanding or misinterpretation and goes against the attempt for a more universal scoring system. The use of the adjusted NEWS2 is though fully acceptable in special medical environments such as pulmonary departments, after the patient is evaluated by experienced medical staff or when the diagnosis of AECOPD is made with confidence. Echevarria et al. investigated the use of NEWS and adjusted NEWS2 in patients who were admitted for AECOPD. 29 In their study, the NEWS2 score was re-calculated with the assumption that all patients with COPD should have a target oxygen saturation of 88%–92%. This intervention reduced the alert frequency as expected and in addition the adjusted NEWS2 for all COPD patients was shown superior as a mortality predictor. 29 The authors concluded that NEWS2 scale should be used for monitoring of all patients with AECOPD. This presumes as mentioned above a confident diagnosis of AECOPD. The high rate of co-morbidities in the COPD populations which reasonably leads to a relative high rate of hospital admissions for reasons other than AECOPD should be taken in consideration. 56 Our study was conducted in a general hospital without a specialized acute department for acute pulmonary cases and we therefore decided not to apply the NEWS2 score in the studied population because of the above considerations with the acceptance of the possibility of higher false alerts.
In this study, we found no correlation with early warning scores and in-hospital survival possibly due to the small number of hospital deaths. Mortality in COPD exacerbations is influenced by many different factors as mentioned above that may not be solely reflected in the early warning scores. Though, we could show that both mortality and number of exacerbations at 6 months after AECOPD was significantly correlated with high NEWS score on the second day of hospitalization for AECOPD (NEWS-d2). This is implicative of a new, long-term perspective in the prognostic role of NEWS in AECOPD which is not previously explored. When we further analysed the relationship of NEWS and MEWS with other parameters of the severity of the AECOPD, we could show that the NEWS-d2 score was superior in its correlation with a number of variants, such as the presence of hypercapnia and the severity of acidosis, the duration of hospital stay, the need and the duration of NIV. This means that patients with AECOPD and a high score of NEWS on the second day of hospitalization run a high risk of treatment failure with a longer hospital stay. In everyday medical care, the interpretation of the results of this study is a need of increased supervision for those patients who are assessed to be at higher risk based on their NEWS score, while at the same time these patients should be planned for admission in suitable care units where NIV, respiratory specialist team or anaesthesiologist should be available. Especially, patients with hypercapnic respiratory failure have been shown to run a greater risk of readmission and death. 57 High levels of both NEWS-d2 and MEWS-d2 were related to higher NT-pro-BNP which may be indicative of more severe and difficult to treat exacerbations in the cases of cardiac stress as patients with AECOPD and elevated NT-pro-BNP levels are at risk for longer hospital stay and need for intensive care. 58 NEWS was better correlated with other parameters of severity of the acute exacerbation showing superiority compared with MEWS. This is obviously explained by the inclusion of oxygen saturation in the vital signs of NEWS which reasonably is of high significance for a pulmonary disease such as COPD. This study is the first one comparing the usefulness of NEWS and MEWS in the AECOPD.
Regarding our findings on the microbiological profile of patients with AECOPD, results highlight the difficulty in giving spontaneous sputum samples, as about 40% could not give a sample. It is therefore difficult to interpret the results of sputum cultures. To our knowledge, this is the first rapport on the association of early warning scores and the infectious profile in the AECOPD. Interestingly, patients with pathogens in the nasopharyngeal samples had high scores in both NEWS and MEWS at the emergency department but also a rapid and significant decline of scores on the second day. This probably reflects a satisfactory response to treatment, although a relation with the overall outcome was not found. In addition, the presence of pathogens in the nasopharyngeal samples was associated with higher CRP reflecting an active infectious condition in this group. Although there is plenty of research on prognostic markers for the outcome of in-hospital AECOPD, the prognostic role of respiratory infections in the AECOPD is less clear. 59 The presence of fever and higher procalcitonin have been correlated with worse prognosis in the course of acute exacerbation of COPD. 60 Shimizu et al. showed prolonged hospitalization in AECOPD caused by Gram-negative bacilli. 61 The presence of pneumonia among patients hospitalized for AECOPD has been associated with more severe clinical and laboratory parameters.6,35,52,53 However, in our study no one of the participants had pneumonic lung infiltrations on radiology.
This study included a homogeneous population of COPD patients with demographic and functional characteristics comparable to previous studies. The main limitations of this report are the relatively small number of participants, the small number of in-hospital deaths that weakens the results for this outcome and the incomplete data of the sputum analysis. The introduction of routine procedures such as sputum induction methods early in the in-hospital care of COPD patients might therefore be of high importance. Nevertheless, this is a prospective report based on a well-selected group of COPD patients and the first comparison study of NEWS and MEWS in the AECOPD with respect to infectious parameters.
Conclusion
In conclusion, we support the superiority of NEWS as a prognostic tool in the evaluation of hospitalized patients with acute exacerbation of AECOPD in comparison to MEWS. A remaining high NEWS score on the second day of hospital stay signals a high risk of hypercapnia, prolonged hospital stay and need of NIV but also higher mortality and more frequent exacerbations at 6 months after AECOPD which emphasizes a potential, long-term perspective of the role of NEWS in AECOPD. Finally, the presence of pathogens in the nasopharyngeal samples was associated with a rapid and significant decline of warning scores on the second day, reflecting probably a satisfactory response to treatment for exacerbations with an identifiable causative factor, though the relationship of EWS and sputum cultures was not satisfactory investigated due to the difficulties in obtaining spontaneous sputum samples in the investigated patient group.
Footnotes
Acknowledgments
On behalf of all authors, we would like to thank Lena Ekström, head of the Department of Internal Medicine at Vrinnevi Hospital, Norrköping, for her support and encouragement for the implementation of this work.
Author Contribution(s)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethics Approval and Informed Consent
The Swedish Ethical Review Authority granted ethical approval for the study, registration number 2018/304-31. A written and informed consent was obtained from all participants.
Consent for Publication
Not applicable.
Availability of Data and Materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.