
Abstract
Background
Studies investigating the effects of announcing spirometric lung-age (SLA) on the smokers’ self-reported smoking status reported conflicting results.
Main objective
To evaluate the effects of a single session intervention including an education conference about smoking harms and announcement of SLA on the participants’ self-reported smoking status.
Methodology
An interventional study was conducted in a cable factory. The intervention included four steps: PowerPoint presentation about raising smoking hazards awareness; general questionnaire; measurement of the anthropometric and spirometric data, and announcement of SLA; and evaluation of the smokers’ self-reported smoking status 10 months later (quitted smoking, decreased consumption; stable consumption, increased consumption).
Results
Thirty-six smokers completed the four steps. Ten months after the intervention, 11.1% of smokers quitted smoking, 52.7% decreased their consumption by 7 ± 4 cigarettes/day, 30.5% kept a stable consumption, and 5.5% increased their consumption by 9 ± 6 cigarettes/day.
Conclusion
Providing an education conference combined with announcing SLA motivated 64% of smokers to quit smoking or to reduce their cigarette consumption.
Keywords
Indroduction
In 2015, around a quarter (24.9%) of the global population aged 15 years, were current-users of some form of tobacco.
1
The costs of smoking have been estimated to drain around US$ 1.4 trillion dollars from the global economy in a single year.
2
Compared to non-smokers, smokers are 10 times more likely to develop chronic lung cancer and chronic obstructive pulmonary disease (COPD), and three times more likely to die due to ischemic heart disease before the age of 65.
3
Therefore, reducing tobacco-use is not only a global health urgency, but also an economic, sustainable development and human rights issue.
1
Smoking prevention and/or cessation are the most effective ways to fight against the increasing epidemic of cigarette smoking.
4
Smoking cessation reverses the aforementioned risks such that a smoker who ceases smoking by the age of 50 has a one-half reduced risk of dying in the next 15 years as compared to a continuing smoker.
3
Among the means usually applied to help smokers quit smoking, are medical interventions (
Interventional studies using SLA as a motivational tool for smoking cessation are scarce, especially in Africa and the underdeveloped countries. To the finest of the authors’ knowledge, only 10 original papers had investigated the effects of confronting smokers with SLA on their smoking attitudes.10,11,14–21 The aforementioned studies reported conflicting results. While some authors reported that communicating SLA prompts smoking cessation,11,14–17,21 others highlighted its ineffectiveness.10,18–20 For example, while Parkes et al. 16 concluded that “telling smokers their SLA promoted successful smoking cessation”, Foulds et al. 18 reported that “baseline SLA feedback did not improve quit rates or compliance at 28-day follow-up in smokers seeking intensive treatment”. These discrepancies could have at least three explanations. On the one hand, some studies10,14–16,19,20 have applied old SLA norms established more than 35 years ago by Morris and Temple. 22 The use of these old norms to calculate SLA 22 is widely questionable for at least six reasons.9,23,24 First, the Morris and Temple norms 22 were performed on an unrepresentative sample of a “normal” population with 79% of participants recruited from two churches in rural America. The principles of these churches prohibit the use of tobacco, alcohol and caffeine and promote a vegetarian diet. 9 Second, Morris and Temple used historical data established 50 years ago, 22 and the age distribution of their participants was biased towards younger ages (30% of participants were between 20 and 30 years old). 22 Third, the participants’ height was measured in “inches’, and the conversion from inch to centimeter, as done in some studies,10,14–16,19 can generate errors.9,23 Fourth, the spirometric data were collected with a very old equipment and by applying guidelines that differ from those currently recommended by learned societies. 25 Fifth, the statistical method applied to establish the SLA norms is criticized. 9 Indeed, Morris and Temple 22 applied a circular argument and estimated the SLA from the regression equations predicting the spirometric reference values. In summary, using the norms published by Morris and Temple 22 would be a source of over/underestimation of SLA.9,23 Sixth, till December 2020, at least five additional SLA norms have emerged worldwide (Japan, USA, Australia; North-Africa),26–30 and some of them26–29 did not reliably predict chronological-age data in the North-African population. 24 On the other hand, the effects of announcing SLA to smokers may be influenced by multiple factors, including the differences in racial backgrounds and cultural practices, smoking cessation programs, participants’ characteristics (especially age, socioeconomic-level), and so on.15,17,21,31 Finally, various types of interventions were implemented: announcing SLA only,11,14–16 announcing SLA associated with other means, such as pharmacotherapy, or RC.10,17–19–21 Interventions and anti-smoking campaigns aiming at encouraging cessation often debate the damaging health effects of smoking. 32 Nevertheless, numerous participants are unlikely to become interested in quitting without a convincing proof that smoking is damaging their health. 19 To the best of the authors’ knowledge, no previous African study has assessed the self-reported smoking status of factory employees following a single intervention consisting in announcing SLA combined with an education session about the harmful effects of smoking.
In Tunisia, the 2018 “current tobacco-use” rates among people aged ³ 15 years was 25.6%.
1
The direct and indirect economic cost of smoking (
Population and methods
Study design
This interventional study was conducted in DRÄXLMAIER group in Sousse, Tunisia. The latter is a factory specialized in coating and assembling interior parts of automobiles (n = 587 employees). All the study procedures were in accordance with the Helsinki Declaration. All the employees were invited to an intervention program to raise awareness with respect to the smoking hazards. Approval for the study was obtained from the Farhat HACHED Hospital Ethical Committee (approval number 12092018). Oral consent was obtained from all the participants in the presence of at least one witness. The participants were individually informed about the study proposes, about their right to refuse to participate and/or to withdraw from participating in the study, and they were informed that their data are confidentially protected.
Sample size
The sample size was estimated using this formula
36
: N = [(Zα/2)
2
× P × (1 – P) × D]/E2; where «
Population
The target population was the employees who were working the day of the intervention and who volunteered to undergo the study. Only current male exclusive cigarette-smokers were included. In order to assess the “stage of change”, the participants were asked whether they intend to quit smoking in the next year.
37
The integrative model of change introduced by Prochaska and Diclemente, which includes six “stages of change” (
Protocol
The protocol comprised two parts

Study protocol. FEV1: forced expiratory volume in one second. FEV6: forced expiratory volume in six seconds. SLA: spirometric lung-age.
The second part of the intervention, with respect to the outcome measures, was carried out 10 months after the intervention (July 2019). The participants were contacted by phone by a trained interviewer (KD in the authors’ list) having no prior contact with them in order to evaluate their self-reported smoking status: quit smoking (yes/no), decrease smoking, maintain stable consumption or increase consumption. In the cases involving a decrease or an increase in cigarette consumption, the change in daily consumption (cig/day) was noted.
Data management
The corpulence status was identified 42 : underweight (BMI < 18.5 kg/m²), normal weight (BMI: 18.5 - 24.9 kg/m²), overweight (BMI: 25.0 - 29.9 kg/m²), and obesity (BMI ≥ 30.0 kg/m²). For the cigarette-dependence status, two groups of participants were identified: nondependent (FTCD score ≤ 2) and dependent (FTCD score ≥ 3). For the spirometry test, three spirometric patterns were possible 43 : “no” bronchial obstruction (FEV1/FEV6 ≥ 0.80), “possible” bronchial obstruction (0.70 ≤ FEV1/FEV6 < 0.80) and “most likely” bronchial obstruction (FEV1/FEV6 < 0.70). According to the SLA values, two scenarios arise. If the SLA matched the chronological-age, the physician (KHM in the authors’ list) informed the participant that the test results were normal and that his lungs seemed to be normal at that time. Yet, the physician informed the participant that the risk of having other smoking-related health problems would remain, and that continuing to smoke would lead to having higher SLA in the future. 17 If the SLA was greater than the chronological-age, the physician announced the SLA to the participant and informed him that his SLA is suggestive of a possible harm due to smoking. The participant was also informed that smoking cessation would slow down the worsening rate of his lung function, bringing it to a physiological age-related decline. However, the smoking-related lung harms would not be restored. 17
Ten months after the intervention, participants were divided into two groups: participants who quit or decrease smoking; and participants who maintain stable or increase consumption.
Statistical analysis
Categorical data (
Results
Fifty-three male participants attended the education session and volunteered to take part in the study. Among these participants, 11 were not included (seven narghile-smokers and four participants did not answer the FTCD). Among the 42 participants who completed the four steps of the intervention protocol, only 36 (86%) answered the phone call 10 months later. The six remaining participants were contacted at least five times during a week, but they could not be reached. Therefore, they were excluded from the analysis

Study flow chart. FTCD: Fagerström test for cigarette dependence. SLA: spirometric lung-age.
Table 1 presents the baseline characteristics of the participants. Thirty (83.33%) and six (16.67%) participants were, respectively, nicotine-dependent and nicotine-nondependent. The dependent and nondependent groups had similar chronological-age and SLA values. Compared to the nondependent group, the dependent one had lower BMI and higher daily cigarettes consumption. The SLAs of the total sample and the dependent group were higher than their chronological-ages by 4.54 (p = 0.01) and 5.11 (p = 0.044) years, respectively.
Baseline characteristics of the participants.

‘Change in age’: difference between the chronological-age and the spirometric lung-age. P: probability.
Quantitative and categorical data were expressed as mean ± SD and number (%), respectively.
Applied statistical tests for comparison:
Between the chronological-age and the spirometric lung-age for the same group: Wilcoxon test (*p < 0.05). Of categorical data between the 2 groups: Two-sided Chi-square Of quantitative data between the 2 groups: Student test.
Table 2 presents the participants’ spirometric data. All participants had a FEV1/FEV6 ³ 0.70. The dependent and nondependent groups had similar spirometric data and included similar percentages of participants with “no” or “possible” bronchial obstruction.
Spirometric data of the participants.
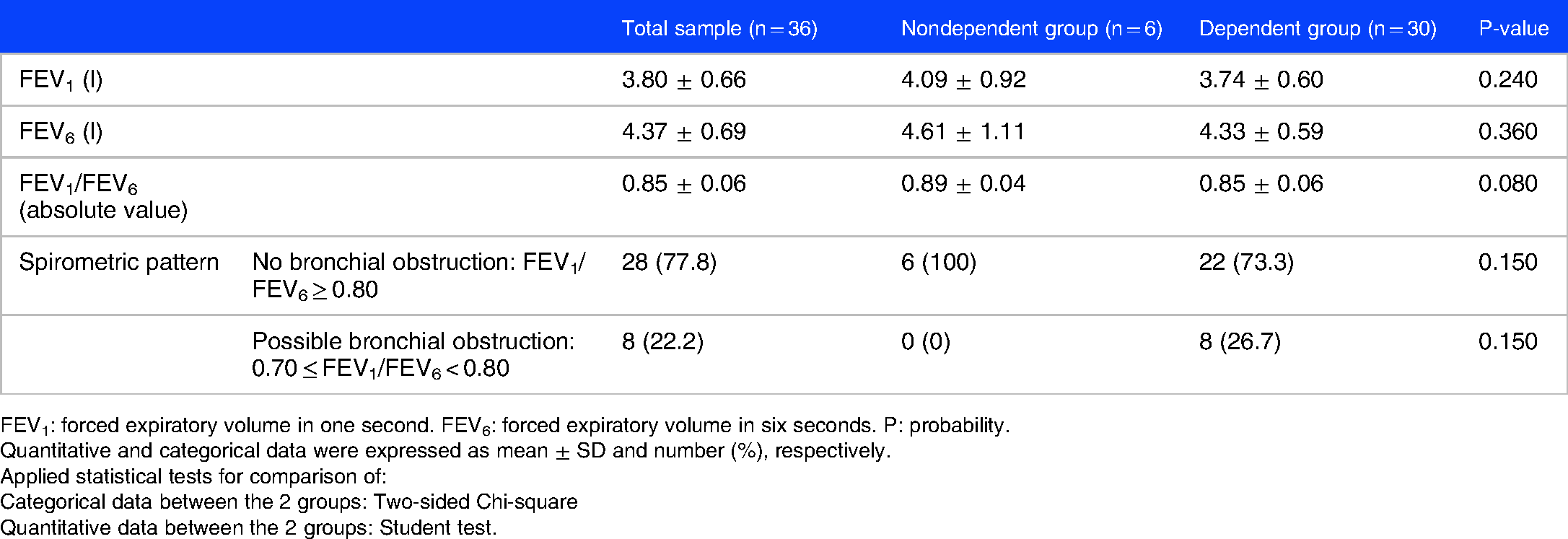
FEV1: forced expiratory volume in one second. FEV6: forced expiratory volume in six seconds. P: probability.
Quantitative and categorical data were expressed as mean ± SD and number (%), respectively.
Applied statistical tests for comparison of:
Categorical data between the 2 groups: Two-sided Chi-square
Quantitative data between the 2 groups: Student test.
Ten months after the intervention, four (11.1%) and 33 (88.9%) participants reported that they quit smoking and did not quit smoking, respectively. Among the 33 participants who did not quit smoking, 19 (52.7%) decreased their consumption, 11 (30.5%) maintained stable their consumption, and two (5.5%) increased their consumption. In the groups who decreased and increased their consumption, the mean ± SD of cig/day were 7 ± 4 and 9 ± 6, respectively.
Compared to the group who maintain stable or increase its consumption, the group who quit smoking or decrease its consumption had significantly higher SLA by ≈10 years (p = 0.010) and higher “change in age” by ≈8 years (p = 0.020) (Table 3).
Characteristics of the participants 10 months after the intervention (n = 36).

‘Change in age’: difference between the chronological-age and the spirometric lung-age. FEV1: forced expiratory volume in one second. FEV6: forced expiratory volume in six seconds. P: probability. Quantitative and categorical data were expressed as mean ± SD and number (%), respectively.
Applied statistical tests for comparison of:
Categorical data between the 2 groups: Two-sided Chi-square
Quantitative data between the 2 groups: Student test.
Discussion
The announcement of SLA combined with an education session about smoking harms had motivated 23 (64%) participants to improve their self-reported smoking status: four participants (11%) quitted smoking and 19 (53%) decreased their consumption by 7 ± 4 cig/day. The profile of participants who quit smoking or decrease cigarette consumption was characterized by a significantly higher SLA and a significantly worse “change in age”.
Ceasing and eliminating smoking requires integrated, multi-faceted strategies addressing both physical dependence and social context. 15 These strategies often include prevention measures (ie; helping to prevent non-smokers from starting this habit, which is the most important strategy) involving quitting (ie; helping quit and avoid relapse, which is vital for an active and healthy lifestyle), and protection (ie; protecting from the harmful effects of smoking and from the tobacco industry marketing influences). For smoking cessation, numerous procedures of evidence-based treatments for tobacco-dependence [brief-advice, short information from health specialists, telephone call quit lines, pharmacotherapy] are available in many countries. 44 While brief-advice is the method having the best cost/efficiency ratio in public health if it is systematically delivered, middle- and low- income countries appear in the penultimate position in the international ranking with regard to the frequency of advice given to smokers. 45 Among the methods used to help smokers quit smoking, is the announcement of SLA. The concept of SLA was initially established as a psychological instrument to show smokers the apparent aging of their lungs.16,22 SLA is usually appraised from regression equations for the FEV1 in healthy non-smokers, and constitutes the age at which the FEV1 measured in an individual equals the predicted value of FEV1, taking into account age, height, sex and ethnicity. 9 More details about the conceptual framework for the use of SLA is developed in the Supplementary file 1.
Studies analyzing the effects of announcing SLA as a motivational tool for smoking cessation are scarce and presented conflicting results.10,11,14–21 The designs and the main results of the studies announcing SLA only11,14–16 or associated with other methods (eg, pharmacotherapy or RC),10,17–21 are exposed in Supplementary files 2 (Table 1S) and 3 (Table 2S), respectively.
Discussion of Results
Frequencies of participants who changed their smoking attitudes (tables 1s and 2s)
Our single intervention had motivated 64% of participants to improve their self-reported smoking status. This confirmed the privileged position of occupational physicians in smoking prevention.34,35 Results of the studies reporting the effects of announcing SLA (alone or in addition to some other interventions) on participants quit smoking are conflicting.10,11,14–21 First, studies lacking control-groups reported contradictory results.14,15,19 On the one hand, one study reported no effect of SLA and respiratory symptoms feedback on the desire to quit, although participants were divided into those having a SLA lower or higher than chronological-age. 19 On the other hand, it appears that 22.9% of participants quit smoking, 15 61.1% increased their motivation to quit, 14 and 48.6% had the intention to quit in the future. 15 Second, some case-control studies reported inconsistent results.11,16–18,20,21 While two studies identified a significantly higher percentage of cases who quit smoking compared to controls (13.6 vs 6.4%, 16 22.1 vs 12.0%, 21 respectively), three other studies noted similar percentages of cases and controls who quit smoking (32 vs 24%; 11 50.8 vs 52.4%; 18 59.6 vs 41.9%, 17 respectively). In addition, no significant difference was identified between cases and controls even when participants were divided into those having a normal (18 vs 33%, respectively) or a high (39 vs 17%, respectively) SLA. 11 Third, one study including four groups (usual care, SLA, SLA plus contingency management, contingency management) highlighted similar percentages of participants who quit smoking (4%, 0%, 0%, and 14%, respectively). 10 Fourth, Segnan et al. 20 reported similar frequencies of biologically verified smoking cessation 12 months after four different interventions [minimal intervention (4.8%), RC (5.5%), RC and use of nicotine gum (7.5%), RC and announcement of SLA (6.5%)].
Our conclusions are intermediate with those reported in the literature.10,11,14–19 First, our frequency of participants quit smoking (ie; 11.1%) is lower than the reported frequencies,14–16,21 which varied between 22.1
21
and 84.6%.
16
Second, our frequency of participants who did not quit smoking (ie; 84.6%) was significantly lower than the one observed in controls (90.4%).
16
Third, in participants who did not quit smoking, the means of daily cigarette consumption reported in our study (7 ± 4 cig/day) was lower than the ones reported in similar studies (
Profile of participants who quit or decrease cigarette smoking (tables 1s and 2s)
Investigating the profile of participants who quit or decrease cigarette smoking is rarely tackled in the literature. In our study, among all the evaluated data, only high SLA and high “change in age” appear to influence the smoking cessation (Table 3). Conflicting results have been advanced with regard to the factors influencing smoking cessation after telling participants their SLA (alone or in addition to other interventions).10,11,14–19 On the one hand, some studies reported similar findings to those identified in our study.14,19,21 First, Lorenzo et al. 14 reported that the presence of an “abnormal” SLA is related to the increased motivation to quit. Second, Lipkus and Prokhorov 19 identified that cases with SLA ≥ chronological-age increase their perceived comparative risk from baseline to follow-up. On the other hand, some studies reported different findings compared to our study. First, Parkes et al. 16 noted that participants with a high SLA are no more likely to quit. Second, Kaminsky et al. 11 reported no significant association between attempts to quit and the interaction of group assignment and SLA. Third, Ojedokun et al., 21 reported that within the intervention group, smokers with more advanced SLAs were just a likely to stop smoking as those with SLAs closer to their chronological-age. Fourth, Lipkus and Prokhorov 19 reported that increasing SLA is not related to the desire to quit after partialling baseline desire to quit. They also reported that cases and controls (with SLA < chronological-age) perceive a comparative risk decrease from baseline to the lab follow-up and that increasing SLA in cases is not correlated with any risk or worry outcome although the cases were divided into those having SLA lower or higher than chronological-age. Fourth, no significant difference in the clinical characteristics (SLA, “change in age”, FEV1, FEV1/FEV6, treatment status) was reported between the quit smoking and non-quit smoking in cases. 17 Finally, additional factors that influence smoking cessation have been advanced: less nicotine dependence, high socioeconomic-level, high schooling-level, Varenicline/nicotine patch, stage on the wheel of change, and age.11,15,17,21 For example, Tanihara and Momose 46 have reported that “nicotine dependence level of current smokers was negatively associated with cessation attempts during the previous 12 months”, and Ojedokun et al. 21 have reported that “stage on the wheel of change was a strong predictor of smoking cessation, with smokers in the action stage being much more likely to quit than those in pre-contemplation”.
Mechanism by which our intervention attained its effect remains
The precise mechanism by which our intervention attained its effect remains uncertain. While spirometric results would offer a perfect educational occasion for smokers to notice their lung health status, this method failed to encourage long-term smoking cessation.17,47 This may be because the lay public usually fails to comprehend the full connotation of spirometry in the context of long-term health and life span. 17 In contrast, the term “SLA”, predictable from some spirometric data seems to be cooler and more suitable for smokers. 17 Announcing SLA may successfully appeal to smokers as it informs them about the risk of developing lung conditions. 17 Helping smokers to recognize their lung health status would, then, encourage them to quit smoking. 17
What are the reasons for inconsistent results between-studies?
Three reasons for inconsistent results are exposed in the “Introduction”. Additional reasons related to the study design (
In our study, only males were included. In other related studies, the percentage of males varied between 35%
11
and 100%.
15
In Tunisia, smoking is a taboo subject for working females who often refuse to participate in interventions of this kind. It appears that there is a sex-related beliefs and attitudes about smoking cessation.
48
A recent study reported that females are ambivalent about quitting smoking or not, and males mention not needing professional support.
48
Moreover, one American study reported that “successful smoking quitters” were more likely to be older and male.
49
In this study, similar to another one,
15
the target population was composed of employees working in a factory. This was different from previous studies, where participants were recruited from those referred to a hospital lab,
11
an outpatient clinic
17
or a general practitioner's medical office.14,20,21 Other participants were recruited from colleges
19
or from the community.10,16,18 It is possible that for participants referred to a medical institution11,14,17,20,21 due to some breathing problems, finding a “normal SLA” may have reduced anxiety, thus leading to a diminished desire to quit.
11
This might not have been the case for participants included in our study as, by virtue of their consent; they might have been more open to health campaign.11,16,50 However, this study results should be interpreted vigilantly since it is uncertain whether they can be generalized to community and other employee population. The mean age (in years) of our participants (34 ± 6) was higher than the one of Lipkus and Prokhorov
19
(21 ± 2), closer to the one of Ben Mdella et al.
15
(36 ± 7) or Ojedokun et al.
21
(38 ± 15), and lower than those of other related studies (46,
14
47 ± 12,
18
52 ± 11,
17
53 ± 12
16
). It appears that with increasing age, many heavy smokers eventually stop smoking.
49
The mean of cigarette consumption (in PY) of our participants (14 ± 9) was closer to the one in other studies (16 ± 7,
19
16 ± 16
21
), but lower than the ones in other studies (26,
14
31 ± 18,
16
39 ± 25
17
). The mean of daily cigarette consumption of our participants (18.8 ± 6.2) was higher than those reported in other related studies (13.3,
14
16 ± 6,
15
16.5 ± 9.0,
16
17.6 ± 7.8
18
). One study had reported that a higher daily cigarette consumption was associated with lower odds of smoking cessation success.
51
In this study, the mean FTCD score was 5.3 ± 1.8, and 83.3% of participants were nicotine-dependent. In some related studies,10,14,18 different values were reported. The mean and the median of FTCD score were 4.6 ± 1.9
18
and 3.5 (2-4) for the SLA group,
10
respectively. In another study, only 36.4% of participants were nicotine-dependent.
14
According a recent study, having a lower nicotine dependence was among the significant predictors of sustained smoking abstinence.
52
In our study, all participants were at a pre-contemplative stage.
37
This was not the case of the participants included in the study of Ojedokun et al.,
21
where 19.7%, 42.5%, and 38.8% of cases were respectively, at the following stages: pre-contemplation, contemplation and preparation. In this study, an education session about the harmful effects of smoking preceded the announcement of SLA. In some related studies, SLA announcement was associated with different other interventions (
Study strength and limitations
One strong point of this study, as done in another one, 17 was the use of local SLA norms. 28 In two previous studies,11,18,21 the applied SLA norms were unspecified, and in six studies,10,14–16,19,20 old norms were applied. 20
This study presents some limitations. The first is related to the study design (before-after trial in a single group) and the lack of a control-group, which makes data interpretation “uncertain”. This situation limits the value of our results and restricts their interpretation to only strong trends. The inclusion of a control-group, as done in some studies,10,11,16–19 would have provided more solid and objective conclusions. The second limitation concerns the nature of the intervention itself (
To conclude, SLA announcement combined with an education session appears to be a practical tool for promoting smoking cessation since 64% of participants quitted smoking or reduced their smoking consumption. The profile of participants who quit smoking was characterized by a significantly higher SLA. Even though evaluating SLA does add four to five minutes to the consultation time, this can convert into clinically operative action, which can be simply integrated into routine first consultation lines.
21
In clinical practice, the authors recommend to perform a spirometry (FEV1, FEV6) on all smokers and to calculate their SLA in the first consultation lines (
Supplemental Material
sj-docx-1-cra-10.1177_11795484211047041 - Supplemental material for Self-Reported Smoking Status 10-Months After a Single Session Intervention Including an Education Conference About Smoking Harms and Announcement of Spirometric Lung-Age
Supplemental material, sj-docx-1-cra-10.1177_11795484211047041 for Self-Reported Smoking Status 10-Months After a Single Session Intervention Including an Education Conference About Smoking Harms and Announcement of Spirometric Lung-Age by Khansa Derbel, Chiraz Maatoug, Amira Mchita, Khaoula Hadj Mabrouk and Helmi Ben Saad in Clinical Medicine Insights: Circulatory, Respiratory and Pulmonary Medicine
Supplemental Material
sj-docx-2-cra-10.1177_11795484211047041 - Supplemental material for Self-Reported Smoking Status 10-Months After a Single Session Intervention Including an Education Conference About Smoking Harms and Announcement of Spirometric Lung-Age
Supplemental material, sj-docx-2-cra-10.1177_11795484211047041 for Self-Reported Smoking Status 10-Months After a Single Session Intervention Including an Education Conference About Smoking Harms and Announcement of Spirometric Lung-Age by Khansa Derbel, Chiraz Maatoug, Amira Mchita, Khaoula Hadj Mabrouk and Helmi Ben Saad in Clinical Medicine Insights: Circulatory, Respiratory and Pulmonary Medicine
Supplemental Material
sj-docx-3-cra-10.1177_11795484211047041 - Supplemental material for Self-Reported Smoking Status 10-Months After a Single Session Intervention Including an Education Conference About Smoking Harms and Announcement of Spirometric Lung-Age
Supplemental material, sj-docx-3-cra-10.1177_11795484211047041 for Self-Reported Smoking Status 10-Months After a Single Session Intervention Including an Education Conference About Smoking Harms and Announcement of Spirometric Lung-Age by Khansa Derbel, Chiraz Maatoug, Amira Mchita, Khaoula Hadj Mabrouk and Helmi Ben Saad in Clinical Medicine Insights: Circulatory, Respiratory and Pulmonary Medicine
Footnotes
Acknowledgments
Authors wish to express their sincere gratitude to all the employees for their cooperation. Authors wish also to thank Professor Samir BOUKATTAYA for his invaluable contribution in the improvement of the quality of the writing in the present paper.
Note
The abstract of the present paper was presented during the European Respiratory Society International Congress, ERS 2020 (Vienna [Austria]: 5-9 September 2020). First author: Helmi BEN SAAD.
Finding
This research received no specific grant from any funding agency in the public, commercial, or non-profit sectors. There is no restriction on data sharing.
Establishment Where the Work was Performed
DRÄXLMAIER group in Sousse, Tunisia.
Conflicts of Interest
Research Ethics Section and Patient Consent
Approval for the study was obtained from the Farhat HACHED Hospital Ethical Committee (approval number 12092018)
Authors’ Contributions
Data Availability Statement
Data will be available upon request from the corresponding author (helmi.bensaad@rns.tn)
Ethical Approval
Approval for the study was obtained from the Farhat HACHED Hospital Ethical Committee (approval number 12092018).
Informed Consent
Oral consent was obtained from all the participants in the presence of at least one witness.
Trial Registration
Not applicable, as no trial was conducted.
Supplemental material
Supplemental material for this article is available online.
List of Abbrevations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.