
Abstract
Solitary fibrous tumors of the pleura (SFTP) are rare mesenchymal neoplasms that originate from mesenchymal growth in the pleura, tend to be single tumors, usually have an indolent course and show nonspecific symptoms. SFTP can be often diagnosed from an incidental finding of a single mass in the thorax and should be confirmed by biopsy and immunohistochemistry. A minority of cases may present Doege–Potter syndrome (DPS, episodes of refractory hypoglycemia) associated with production of insulin-like growth factor 2 (IGF-2). Both SFTP and DPS are rare occurrences with less than 2000 cases reported worldwide. The curative treatment is tumor resection. Two cases of patients with DPS caused by SFTP are presented below.
Introduction
Solitary fibrous tumors of the pleura (SFTP) are rare mesenchymal neoplasms that originate from mesenchymal growth in the pleura (visceral or parietal).1-6 SFTP tend to be single tumors, and to date, no genetic predisposition or relationship with tobacco exposure or other environmental factors has been found. 7 Only 10% of SFTP are extra-thoracic, and in rare cases they can present as an intrapulmonary mass.8-10
SFTP usually have an indolent course and occasionally show nonspecific symptoms such as cough, dyspnea, thoracic pain, weight loss, and hemoptysis. 11 A minority of cases can coexist with Doege–Potter syndrome (DPS) or Pierre Marie–Bamberber syndrome (hypertrophic pulmonary osteoarthropathy).12-17
DPS is a paraneoplastic syndrome characterized by refractory hypoglycemia, suppressed serum insulin levels, low serum C-peptide and growth hormone (GH), associated to increased production of insulin-like growth factor 1 (IGF-1) and IGF-2 levels. IGF-1 and IGF-2 have an insulin-like amino acid sequence of approximately 50%. 18
Under normal conditions, IGF-2 is usually bound in a ternary complex with insulin-like growth factor-binding protein-3 (IGFBP-3) and an acid-labile subunit, forming a molecule that cannot pass through the endothelial membrane. 19 The gene encoding IGF-2 is located in chromosome 11 next to 2 tumor suppression genes: H19 and p5. These genes have a genomic imprint, that is, only the paternal allele is expressed for IGF-2 and the maternal allele for H19 and p5, which is why it is necessary to maintain both H19 and p5. 20 When this relationship is lost, it results in overexpression of IGF-2, increasing the levels of the high-molecular-weight aberrant IGF-2. 20 This high-molecular-weight IGF-2 forms an abnormal binary complex of lower molecular weight that has less affinity for the serum-binding proteins and is capable of crossing the endothelial membrane.21,22 On binding to insulin receptors, it facilitates glucose transport to the muscles and inhibits gluconeogenesis in the liver and lipolysis in the adipose tissues, leading to the development of hypoglycemia in patients with tumors that secrete large amounts of high-molecular-weight IGF-2.23-25
Definitive diagnosis of DPS is established by measuring serum GH, IGF-1, and IGFBP-3 levels, which are usually decreased, along with IGF-2 levels, which can vary, and high-molecular-weight IGF-2 levels, which are increased. 20 The IGF-2/IGF-1 ratio can be calculated, which tends to be <10. Hypokalemia can also result from potassium translocation within cells. 20 Symptomatic treatment includes replacement with dextrose fluids and the use of analogs of somatostatin, recombinant GH, diazoxide, and corticosteroids. However, their use is still disputable. The curative treatment is tumor resection.26-30 Two cases of patients with DPS caused by SFTP are presented below.
Case Report
Case No. 1
A 71-year-old woman with no relevant history visited a primary care center for generalized tonic-clonic seizure caused by severe hypoglycemia. According to her medical history, she had been experiencing weight loss, dyspnea, and cough with whitish expectoration for the past 10 months as well as seizures that were treated with dextrose.
On admission, her blood pressure was 142/82 mmHg, temperature was 37.2°C, heart rate was 106 beats per min, and respiratory frequency was 32 breaths per minute. She was alert, with increased inspiratory effort. Auscultation findings included decreased breath sounds in both lung fields with right prevalence and asymmetrical thoracic expansion. She presented nail clubbing. Neurological and physical examination results were normal. Laboratory study results are reported in Table 1. During hospitalization, it was necessary to administer 50% dextrose via central venous catheter, with partial improvement of glycemia measurements. Thoracic X-ray and computed tomography (CT) revealed a large mass with right basal predominance that was encapsulated and non-homogeneous; it occupied 50% to 70% of the right hemithorax (Figures 1 and 2). CT-guided percutaneous biopsy results revealed a malignant SFTP, hemangiopericytoma type. She underwent surgery for tumor resection, and a tumor approximately 30 cm in diameter with a pedicle that was dependent on the right lower lung lobe and with lax adhesions to the thoracic wall, diaphragm, and mediastinum was found.
Laboratory test results of 2 patients with Doege–Potter syndrome at hospital admission.


Chest CT. Mediastinal window; a, b, c. A solid heterogeneous 18×19×12 cm mass can be seen within the 2 lower thirds of the right hemithorax, causing left shifting of the cardio mediastinum, with compression of the bronchus towards the right middle and lower lobes, causing atelectasis of these 2 lobes. The mass has border enhancement, there are mediastinal adenomegalies of up to 16 mm in the subcarinal station. No pulmonary infiltrates are seen.
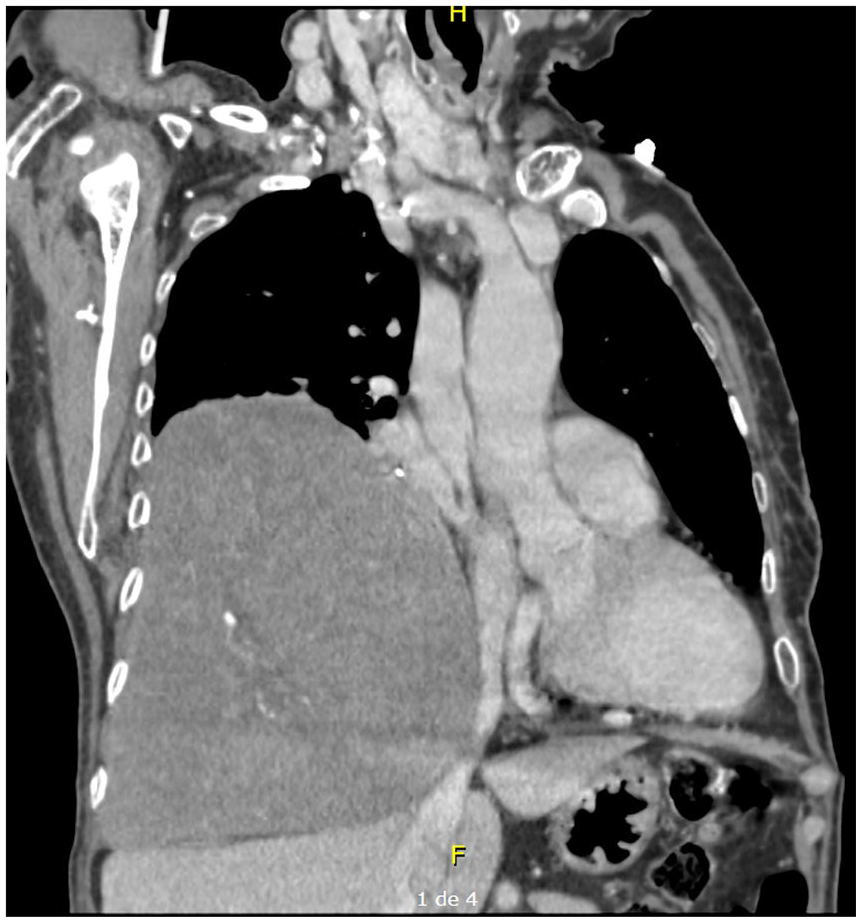
Chest CT. Sagittal reconstruction; the mass is seen in the lower right hemithorax, causing eversion of the right diaphragm.
The dried mass measured 21 × 17 × 8 cm, had a brown color, smooth surface, and firm consistency. The interior showed a grayish-brown color with a central necrotic area. Microscopically, small, slightly elongated cells that were arranged in a pericytic pattern were identified, in the middle of which abundant collagen bridges were present. Areas of interstitial hyaline fibrosis were also observed, as well as highly vascularized areas and a large area of ischemic necrosis in a central location. The mitotic index was >10 per 10 high-power fields. An immunohistochemistry study was conducted with BCL2, CD34, CD99, and vimentin as diffuse positives, CD117, EMA, CK AE1-AE3, S-100, desmin, actin, and Mart-1 as negative, and Ki-67 of 10%. These results revealed the presence of a malignant fibrous tumor of the pleura and related DPS (Figures 3 and 4). Glucose measurements were normal after surgery.

(a) H&E 4X. Histological sections show a mesenchymal lesion that is arranged in a fascicular and occasionally storiform pattern. The large, hyalinized and thick walled vessels are very evident. There is no cytological atypia or signs of mitosis. (b) H&E 10X. At higher magnification, cells alternate between spindle-cell and round, with regular contours, without cytological atypia or mitosis.
(a) BCL2 10X. Immunohistochemistry (IHC) shows intense and global positivity for BCL2 in neoplastic cells. (b) CD34 10X. IHC shows intense and global positivity for CD34 in neoplastic cells. (c) Ki-67 10X. Ki-67 proliferative index is up to 40% in some areas.
At a 1-year follow-up consultation after the diagnosis, the patient showed no signs of relapse. No adjuvant therapy was considered at the time as the surgeon was able to perform a complete resection. During the next few years, she discontinued clinical follow-up and revisited the hospital because of respiratory difficulties, hypoglycemia, and hypokalemia 4 years after the initial tumor resection. Pulmonary embolism was ruled out, and lung lesions were identified as SFTP recurrence (Figure 5). Immunohistochemistry analysis confirmed that it was the same histological pattern, with Ki-67 of 40% (vs. 10% previously). Tumor resection was performed again via open surgery. Although complete resection could not be achieved because of pericardial compromise, the patient showed symptom improvements and remains stable, still being closely followed by the thoracic surgeon. Due to the patients preferences, adjuvant chemotherapy was no initiated, although it was proposed to use Doxorubicin as the best option in her scenario.

Chest CT. Four years after initial mass resection image shows (a, b, c, d) a 15×9×10 cm right pleural mass that causes inversion of the right diaphragm, extrinsic compression of the intermediate bronchus, with atelectasis of the middle and lower right lobes. Additionally, another 4-cm pleural mass is seen in the upper right anterior area (b, c).
Case No. 2
A 72-year-old woman with controlled chronic obstructive pulmonary disease and hypertension underwent thoracic X-ray at another health center due to a non-productive cough for 18 months. Results showed a lung mass on the right hemithorax with biopsy, indicating SFTP. She was referred to our hospital for refractory hypoglycemia and heart failure due to extrinsic compression of the tumor.
On admission, her blood pressure was 128/50 mmHg, mean arterial pressure was 76 mmHg, heart rate was 73 beats per min, respiratory frequency was 20 breaths per minute, temperature was 36.4°C, and SatO2 88%. She had signs of dehydration, grade 2 edema, and decreased breath sounds in the entire right lung field. Her physical examination results were normal. Laboratory test results are shown in Table 1. Thoracic X-ray revealed radio-opacity that occupied almost the entire right hemithorax, which could correspond to pleural effusion and/or pleural thickening. Because her glucose level was 55 mg/dL, treatment with 10% dextrose was initiated. Following an adequate glycemic control, she was taken to surgery.
In the surgical procedure, a large lesion occupying 80% of the right hemithorax that originated from the right lower pulmonary lobe was found. This lesion was attached to the pericardium and right lower pulmonary vein, which tore during dissection, causing massive bleeding that was temporarily controlled while advanced resuscitation maneuvers were performed. However, the patient presented coagulopathy and died. It might have been useful to perform an angiography and embolization of the tumor prior to resection, in order to prevent such complications.
In the pathological analysis, 2 tissue fragments were macroscopically reported. The largest was 20 × 16 × 10 cm (1850 g), and the smallest was 9 × 7 × 4 cm (132 g). They had a smooth, light-brown, multinodular surface with dark and hemorrhagic areas. When cut, the surface was homogeneous and had a light brown color that was yellowish in the middle. Microscopically, the tissue was a neoplasm composed of large cells, with a fusiform tendency that comprised of alternating areas of high cellularity and lax areas. Cells were arranged in long bundles and were surrounded by hyalinized tissue in some areas and necrotic tissue in other areas owing to ischemic changes. There were abundant thin-walled blood vessels with a hemangiopericytic aspect in some areas. Additionally, there were foci with lymphocyte accumulations and abundant eosinophils. The more cellular areas showed an epithelioid appearance with round nuclei. The mitotic index was 0 to 2 per high-power field. No nuclear pleomorphism was observed. In the immunohistochemical analysis, expression of vimentin, BCL2, and CD34 in neoplastic cells were noted. No expression of desmin, actin, S100, CD117, cytokeratins CK20, CK7, CK AE1/AE3, CD10, HMB45, CD99, and calretinin was observed. The Ki-67 was approximately 20% (Figure 6). This report confirmed the diagnosis of a SFTP, which, considering the associated hypoglycemia, was interpreted to be DPS.

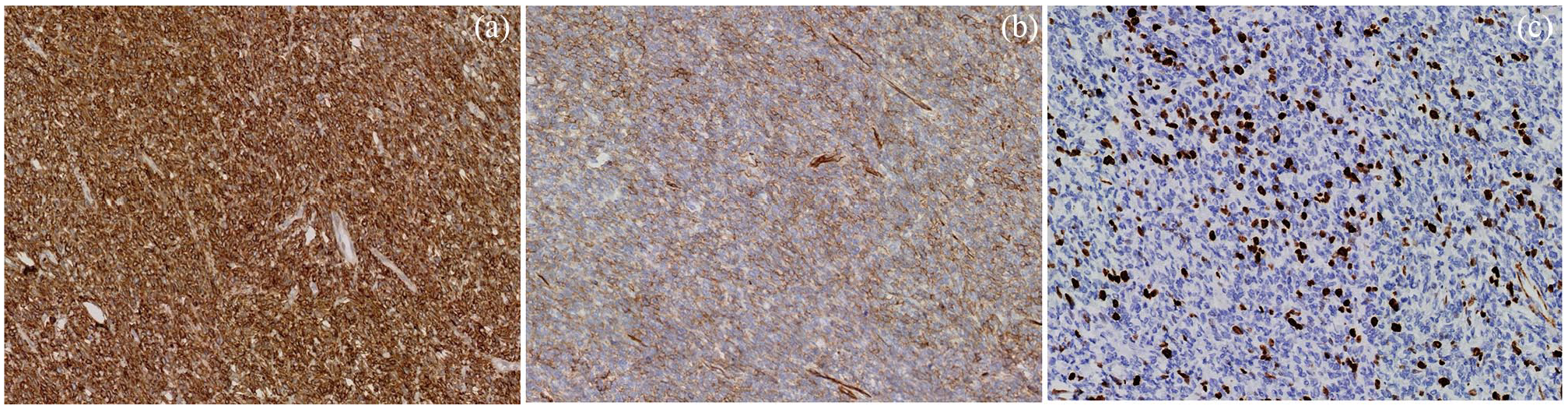
(a) H&E 4X. Histological sections show a mesenchymal lesion arranged in a fascicular and occasionally storiform pattern. Thick and large-walled vessels are evident. (b) H&E 10X. Histological sections show a mesenchymal lesion arranged in a fascicular and occasionally storiform pattern. Neoplastic cells do not have cytological atypia or mitosis. (c) CD34 10X. IHC shows intense and global positivity for CD34 in neoplastic cells. Vessel walls (except for endothelium) are CD34-negative. (d) BCL2 10X. IHC shows intense and global positivity for BCL2 in neoplastic cells.
Discussion
Both SFTP and DPS are rare occurrences with less than 2000 cases reported worldwide.31,32 The peak incidence reported for this tumor is at 60 to 70 years, which is consistent with our patients. SFTP are mostly pleural and single, with no gender predilection.33-35 The epidemiology of DPS remains unknown.
SFTP can be asymptomatic, and the first symptoms to manifest are usually respiratory, followed by hypoglycemia.11,25 In the present cases, both patients initially had respiratory symptoms with subsequent recurring hypoglycemia. However, these tumors generally tend to have a benign course. 11 In this report, patient No. 1 was diagnosed with a malignant tumor of the hemangiopericytoma type, with recurrence 4 years after tumor resection. Patient No. 2 died as a result of surgery complications given the size of the tumor and the mass effect that resulted in heart failure.
SFTP can be often diagnosed from an incidental finding of a single mass in the thorax and should be confirmed by biopsy and immunohistochemistry.36,37 DPS diagnosis, on the other hand, can be confirmed using serum tests capable of differentiating normal IGF-2 from high-molecular-weight IGF-2 via chromatography or western immunoblot and by identifying low levels of IGF-1. 20 In the 2 cases, the patients underwent imaging, and histological and immunohistochemistry diagnoses of SFTP were made, but no serological tests were performed to confirm the diagnosis of DPS due to their unavailability in our laboratory at the time of the patients’ consultation. DPS was diagnosed as patient No. 1 presented refractory hypoglycemia and hypokalemia, as well as a solitary fibrous tumor, and no other causes that could produce her decrease of glycemia levels were found. Her condition was resolved after tumor resection. In patient No. 2, a solitary fibrous tumor was also diagnosed in the absence of other causes of hypoglycemia.
For definitive treatment, total resection of the tumor is the gold standard,20-38 although in some circumstances the mass is too big and has great vascularity leading to intra-operative bleeding as one of the main complications. In these situations, it is best to evaluate preoperatively the tumors vascularity using an angiogram and decide whether embolization to reduce vascularity is the best option, prior to resection.39,40 Co-adjuvant treatment with chemotherapy and/or radiotherapy following complete resection is unusual, being reserved as an option for irresectable and metastatic tumors. Although evidence is scarce, coming primarily from descriptive studies, anthracycline based chemotherapy appears to have the best antitumor activity and is the most frequently used.41,42 Radiotherapy is even more debated for these patients, although some descriptive studies and case reports have proposed it is benefitial, both preoperatively and postoperatively, using doses ranging from 50 to 56 Gray (Gy). 43
DPS can be temporarily treated in a symptomatic manner with continuous dextrose 10% infusion to restore normal glycemic levels.26-30 In addition, the use of glucocorticoids has proved to be effective in dextrose-refractory cases as they stimulate gluconeogenesis and suppress the production of IGF-2. 20
Conclusion
Both SFTP and DPS are rare occurrences with less than 2000 cases reported worldwide. Due to the rare incidence, evidence comes mainly from descriptive studies. However, the gold standard for treatment is total resection of the tumor, while other therapeutic options such as chemotherapy and/radiotherapy are debated and should be considered in patients with more advanced disease. Presurgical embolization of highly vascularized tumors might be beneficial to prevent intra-operative bleeding and further complications.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The authors declare that they have no competing interests. This manuscript has not been published and is not under consideration for publication elsewhere. Additionally, all of the authors have approved the contents of this paper and have agreed to the journal’s submission policies.
Authors’ contributions
All authors have read and approved the manuscript, and significantly contributed to this paper. LFT: Conception and design, literature review, manuscript writing and correction, final approval of manuscript. JEB: Literature review, manuscript writing and correction, final approval of manuscript. CA: Literature review, manuscript writing and correction, final approval of manuscript. JG: Literature review, manuscript writing and correction, final approval of manuscript. MV: Conception and design, literature review, manuscript writing and correction, final approval of manuscript. VZR: Literature review, manuscript writing and correction, final approval of manuscript. BP: Literature review, manuscript writing and correction, final approval of manuscript. LFS: Conception and design, literature review, manuscript writing and correction, final approval of manuscript
Ethics approval and consent to participate
This manuscript was written in compliance with the ethical standards of the institutional ethics committee and with the 1964 Helsinki Declaration. We have approval of the Ethics Committee in Biomedical Research from Fundación Valle del Lili. This is supported in letter No. 436 of 2019. Act No. 25 of December 4, 2019, which is available if needed with the Corresponding Author.
Consent for publication
Written informed consent was obtained from patients for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Availability of data and materials
All data and material are available for sharing if needed.