
Abstract
Background:
The emphysema interventional treatment involves mainly lung volume reduction surgery (LVRS) and endobronchial valve (EBV) implantation. Few institutes discuss these cases at a dedicated emphysema multidisciplinary team (MDT) meeting.
Objectives:
To investigate the impact of a newly established dedicated emphysema MDT meeting on the interventional treatment of such patients.
Methods:
During a study period of 4 years, the outcome of 44 patients who underwent intervention according to the proposal of the emphysema MDT (group A) was compared with the outcome of 44 propensity score matched patients (group B) treated without the emphysema MDT proposal.
Results:
More LVRS and less EBV insertions were performed in group A (P = .009). In group B, the interventions were performed sooner than in group A (P = .003). Postoperative overall morbidity and length of in-hospital stay were similar in the 2 groups (P = .918 and .758, respectively). Improvement of breathing ability was reported in more patients from group A (P = .012). In group B, the total number of re-interventions was higher (P = .001) and the time to re-intervention had the tendency to be less (P = .069). Survival was similar between the 2 groups (P = .884). Intervention without discussion at the MDT and EBV as initial intervention was an independent predictor of re-intervention.
Conclusions:
Interventional treatment for patients with chronic obstructive pulmonary disease (COPD) after discussion at a dedicated MDT involved more LVRS performed, required fewer interventions for their disease, and had longer re-intervention-free intervals and better breathing improvement.
Introduction
Chronic obstructive pulmonary disease (COPD)/emphysema is a leading cause of morbidity and mortality worldwide and represents a significant financial burden and strain on the resources of the health care system.1,2
As no causal therapy exists, treatment focuses on the reduction of the severity of symptoms and the exacerbations, as well as the improvement of the general health status. Despite the alteration of life style (ie, smoking habit) and the pharmacological therapy, the long-term lung function decline has long been perceived as a non-modifiable3,4 event that led to a pessimism regarding exploration of new treatments. 5
Surgical intervention for emphysema was shown to produce a survival benefit over medical treatment, selectively in patients with upper lobe predominant emphysema and poor exercise capacity. 6 Bronchoscopic interventions (mainly endobronchial valves [EBVs]) have been developed to produce a similar lung volume reduction effect and are shown to achieve improved results against medical treatment.7,8 Despite the fact that such interventions (surgical or bronchoscopic) are nowadays recommended as a treatment of choice for selected patients and the fact that an improvement in morbidity and mortality trends has been documented,6-11 the number of procedures performed remains low. 5
This event possibly reflects a sense of nihilism among physicians and a reluctance to offer invasive intervention in emphysema. 12 In addition, no clear strategy exists to identify the correct patients and the correct time to refer them, while only 30% of the participants had access to a dedicated emphysema multidisciplinary team (MDT). 13
A dedicated emphysema MDT has recently been implemented at our institute, following the need for patient selection and referral that arose from launching an EBV programme. Aim of this study was to investigate the impact of this dedicated emphysema MDT meeting on the interventional treatment of patients with emphysema in terms of practice change and outcomes.
Patients and methods
Study design
The medical records and the outcomes of 118 patients with emphysema who were treated with an intervention at our department within the period of 2012-2016 were retrospectively analyzed. Matched pairs of patients subjected to an intervention for emphysema were created producing 2 groups: group A included patients who received an intervention based on a proposal made after discussion at the emphysema MDT and group B included patients subjected to an intervention without discussion at this MDT.
Emphysema MDT setup
It is composed of respiratory physicians, thoracic radiologists, and thoracic surgeons who meet once per calendar month. Referrals are accepted from general practitioners, respiratory physicians, or thoracic surgeons provided that the below-mentioned investigations have been submitted to the MDT:
Lung perfusion scan
Chest-computed tomography with 1 mm thickness slices
Full pulmonary function tests (ie, forced expiratory volume in 1 second [FEV1], forced volume vital capacity [FVC], total lung capacity [TLC], residual volume [RV], diffusional lung capacity for carbon monoxide [DLCO])
COPD assessment test (CAT score)
6-minute walking test
Performance score (PS, 0-3) after consultation with the patient
Routine pre-assessment blood tests and an electrocardiogram
More recently, quantitative computed tomography (CT) scan analysis and an echocardiogram in selected cases have been added
An intervention treatment is then proposed (EBV or lung volume reduction surgery [LVRS]) based on the patient’s operability and the BTS/NICE guidelines/NETT findings:6,9,14
Age: 40-80 years old
Dyspnea at rest or minimal physical activity
Severely affected quality of life (CAT score ⩾ 20)
Heterogenous emphysema
Completion of fissures
Moderate to severe obstructive pattern on spirometry
Hyperinflation (increased RV)
Smoking cessation for at least 6 months
At least one course of pulmonary rehabilitation
After discussion, a decision is reached whether either to offer EBV or LVRS. In some cases, a lung volume reduction intervention is offered, ie, EBV or LVRS, which is left to the discretion of the treating physician, who will take under consideration the patient’s wishes as well.
Perioperative details
According to our department’s programme, LVRS was performed via Video-Assisted Thoracic Surgery (VATS) using 2 or 3 ports with buttressed (Peristrips) endoscopic mechanical staplers. One or 2 intercostal chest drains were left into the pleural space after the operation as per surgeons’ preference.
For the EBV insertion, general anaesthesia and intubation with a rigid bronchoscope were performed. The rigid bronchoscope is positioned at the orifice of the lobar bronchus. A flexible bronchoscope with adequate size working channel was then passed through the rigid one, delivering the measurement catheter with the valve (Zephyr®, PulmonX Corporation, CA, U.S.A.) into the segmental orifices.
Postoperative care
All patients were treated in a dedicated thoracic surgical unit. The ward setting includes a high dependency unit. Analgesia, anti-embolism prophylaxis, and physiotherapy were provided to all patients as per our department’s standardized pathways of care in accordance with the type of intervention (EBV or LVRS).
Patient data
The data investigated were the demographics; the preoperative pulmonary function (FEV1, DLCO, TLC, RV); the co-morbidities (other than COPD/emphysema); the exercise tolerance (in yards) and the performance status (0-3); the number and the type of interventions (EBV or LVRS) and re-interventions (including re-interventions for morbidity); the time to initial intervention and re-intervention (in months); the postoperative morbidity (for all in-hospital stays for all interventions when more than 1); the breathing quality postintervention as stated by the patient during the last recorded follow-up appointment (graded as same, better, or worse); the total length of stay (LOS), ie, the LOS of all in-hospital stays (total number of days of all admissions); the 30-day mortality (mortality documented throughout all in-hospital stays for all interventions when more than 1); and the survivorship (late deaths).
For patients with LVRS, a re-intervention was considered any procedure needed to be done for the disease progression or re-operation for morbidity, ie, bleeding, prolonged air leak, etc. For patients with EBV, the need to reposition the valve or change it either because it has been coughed out or because it failed to produce the desired result and had to be substituted was additionally considered as a separate re-intervention. Chartis catheter assessment for collateral ventilation alone was not considered as a separate intervention.
The morbidity comprised respiratory (chest infection), cardiac (atrial fibrillation), and surgical (surgical emphysema, pneumothorax, wound infection, prolonged air leak) complications.
Methods
To exclude biased patient selection for treatment by physicians/surgeons or by the MDT (Table 1), patient pairs were created after matching for age, sex, body mass index (BMI), pulmonary function, performance status, and exercise tolerance by generating propensity scores with binary logistic regression and using the ‘nearest neighbour’ technique accepting a matching tolerance of 0.2 (pool of 118 total patients). Forty-four matched pairs were yielded and were used for the analysis.
Population characteristics before propensity score matching.

Percentages shown are observations divided by the number of patients of the group. Bold values are the statistical significance if P < 0.05.
Abbreviations: BMI, body mass index; DLCO, diffusional lung capacity for carbon monoxide; FEV1, forced expiratory volume in 1 second; MDT, multidisciplinary team; RV, residual volume; TLC, total lung capacity.
Student’s t test.
Chi-square test.
Mann-Whitney test.
Endpoints
The primary endpoint was the impact on the practice, ie, the change, if any, to the type of the initial intervention proposed. The secondary endpoint was to show whether this change was beneficial to the patients, ie, we investigated the time-to-initial intervention and the re-interventional outcomes (type, total number, and time interval from initial intervention to re-intervention), the breathing quality on follow-up, the survival probability between the groups, the overall interventional outcomes (LOS, morbidity, and 30-day mortality as previously described), and the calculation of independent predictors of re-interventions.
Study approval
The study was discussed at our Clinical Governance Meeting at Leeds Teaching Hospitals Trust, which waived the need of review by a NHS Research Ethics Committee. It also waived the need for informed/signed consent, which was therefore not obtained.
Analysis
Statistical analysis was performed with IBM SPSS Statistics for Macintosh, Version 22.0 (Armonk, NY: IBM Corp.). All numerical data were investigated for normality of distribution with Shapiro-Wilk’s test (normally distributed when P > .05) and Q-Q plots (acceptable figures for normality of distribution) and were presented as mean ± standard deviation (SD). Skewed data were presented as median (lower value-higher value). Categorical data were presented as percentages.
Statistical significance was determined with student’s t, Mann-Whitney (when Levene’s test P < .05 and not normally distributed according to the previous normality testing), chi-square, and Fisher’s exact tests (when cells were calculated with a value <5 of the expected value).
The statistical significant level was set to a P value < .05. A univariate analysis of possible predictors with the re-intervention as the dependent factor was performed with binary logistic regression. A multivariate analysis of the predictors found to be significant was then performed to create a model of re-intervention prediction based on these independent factors. Log-rank was used to investigate differences in Kaplan-Meier’s survival curves. The last date investigated for survival before submission was October 18, 2017.
Results
As previously mentioned, over the study period, a pool of 118 total patients was investigated with a mean age of 61.64 ± 10.06 years while 71 (62.7%) were men. Patients surgically treated without a discussion at the MDT were mainly women; younger in age; with higher BMI, better PS, higher DLCO, and lower RV; and with better exercise tolerance than patients who were treated after a discussion at the MDT (Table 1).
From this pool, 44 matched pairs (44 patients in group A and 44 patients in group B) were generated. The basic characteristics of the 2 groups after matching were similar (Table 2).
Population characteristics after propensity score matching.

All variables shown above were included in the propensity score matching analysis; percentages shown are observations divided by the number of patients of the group.
Abbreviations: BMI, body mass index; DLCO, diffusional lung capacity for carbon monoxide; FEV1, forced expiratory volume in 1 second; MDT, multidisciplinary team; RV, residual volume; TLC, total lung capacity.
Student’s t test.
Chi-square test.
Mann-Whitney test.
Table 3 summarizes the comparison of treatment between the 2 matched groups. More LVRS and less EBVs were performed in patients from group A (P = .009) as an initial intervention offered. In group A, the time to initial treatment was longer (P = .003) whereas the time interval from the initial intervention to re-intervention had the tendency to be significantly longer (P = .069). A re-intervention was necessitated in more patients in group B and the total number of re-interventions in that group was also higher when compared with patients from group A (P = .001, respectively).
Practice and outcomes.

Percentages shown are observations divided by the number of patients of the group. Bold values are the statistical significance if P < 0.05.
Abbreviations: EBV, endobronchial valves; LOS, length of stay; LVRS, lung volume reduction surgery; MDT, multidisciplinary team.
Chi-square test.
Student’s t test.
Mann-Whitney test.
Fischer’s exact test.
Re-interventions after EBV insertion regarded the following: 10 cases in which removal of the valves was decided because they were not working (ie, patients in whom the an initial effect was lost), 12 cases in which additional EBVs had to be inserted because of disease progression (including the contralateral side), and 2 cases in which the valves were coughed out. In patients with LVRS, re-interventions regarded mainly morbidity reasons: 1 case with chest wall hernia, 3 cases with prolonged air leak, and 2 cases for empyema. In 1 case, a VATS had to be abandoned because of extensive adhesions, with the patient receiving a thoracotomy in another setting. In the rest 3 cases, a contralateral procedure was performed.
The breathing quality on follow-up showed improvement in more patients from group A (P = .012). The overall postoperative morbidity and LOS were similar in the 2 groups (P = .918 and .758, respectively).
Thirty-day mortality regarded 1 patient from group A, who developed empyema after LVRS and died from multi-organ failure, and another from the same group who developed respiratory failure after EBV insertion. The short and long-term hazard of re-intervention were higher in group B (log-rank test P = .007, Tarane-Wane test P = .011, Figure 1).
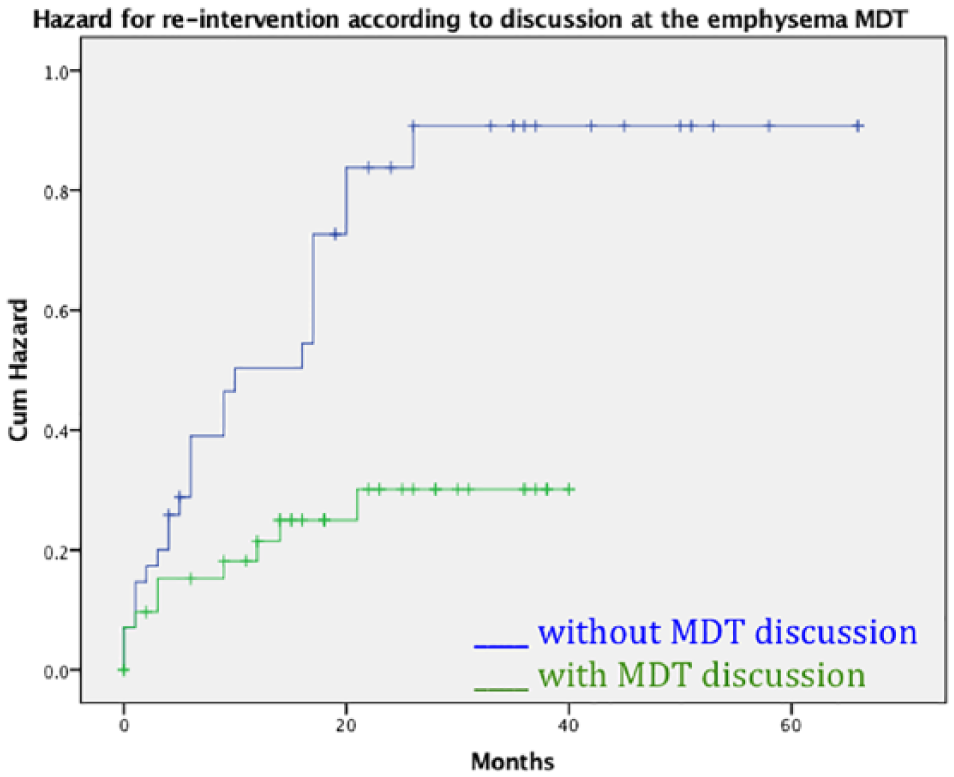
Re-intervention hazard by time according to discussion or not at the dedicated MDT over time. MDT indicates multidisciplinary team.
The subgroup characteristics of patients treated with EBVs or LVRS were similar (Tables 4 and 5). In the EBV subgroup, patients treated after MDT discussion had less re-interventions performed. More patients from this group reported having improved breathing ability while there was a trend for less overall morbidity. The initial treatment was offered with a delay in the same group (Table 6). Similarly, in the LVRS subgroup, patients treated after MDT discussion had less re-interventions performed and more patients reported improved breathing ability. Re-interventions and initial treatment were offered in a more delayed manner (Table 7).
Characteristics of patients undergoing EBV treatment.

All variables shown above were included in the propensity score matching analysis; percentages shown are observations divided by the number of patients of the group.
Abbreviations: BMI, body mass index; DLCO, diffusional lung capacity for carbon monoxide; EBV, endobronchial valves; FEV1, forced expiratory volume in 1 second; MDT, multidisciplinary team; RV, residual volume; TLC, total lung capacity.
Student’s t test.
Chi-square test.
Mann-Whitney test.
Characteristics of patients undergoing LVRS treatment.

All variables shown above were included in the propensity score matching analysis; percentages shown are observations divided by the number of patients of the group. Bold values are the statistical significance if P < 0.05.
Abbreviations: BMI, body mass index; DLCO, diffusional lung capacity for carbon monoxide; FEV1, forced expiratory volume in 1 second; LVRS, lung volume reduction surgery; MDT, multidisciplinary team; RV, residual volume; TLC, total lung capacity.
Student’s t test.
Chi-square test.
Mann-Whitney test.
Outcomes of patients treated with EBV.
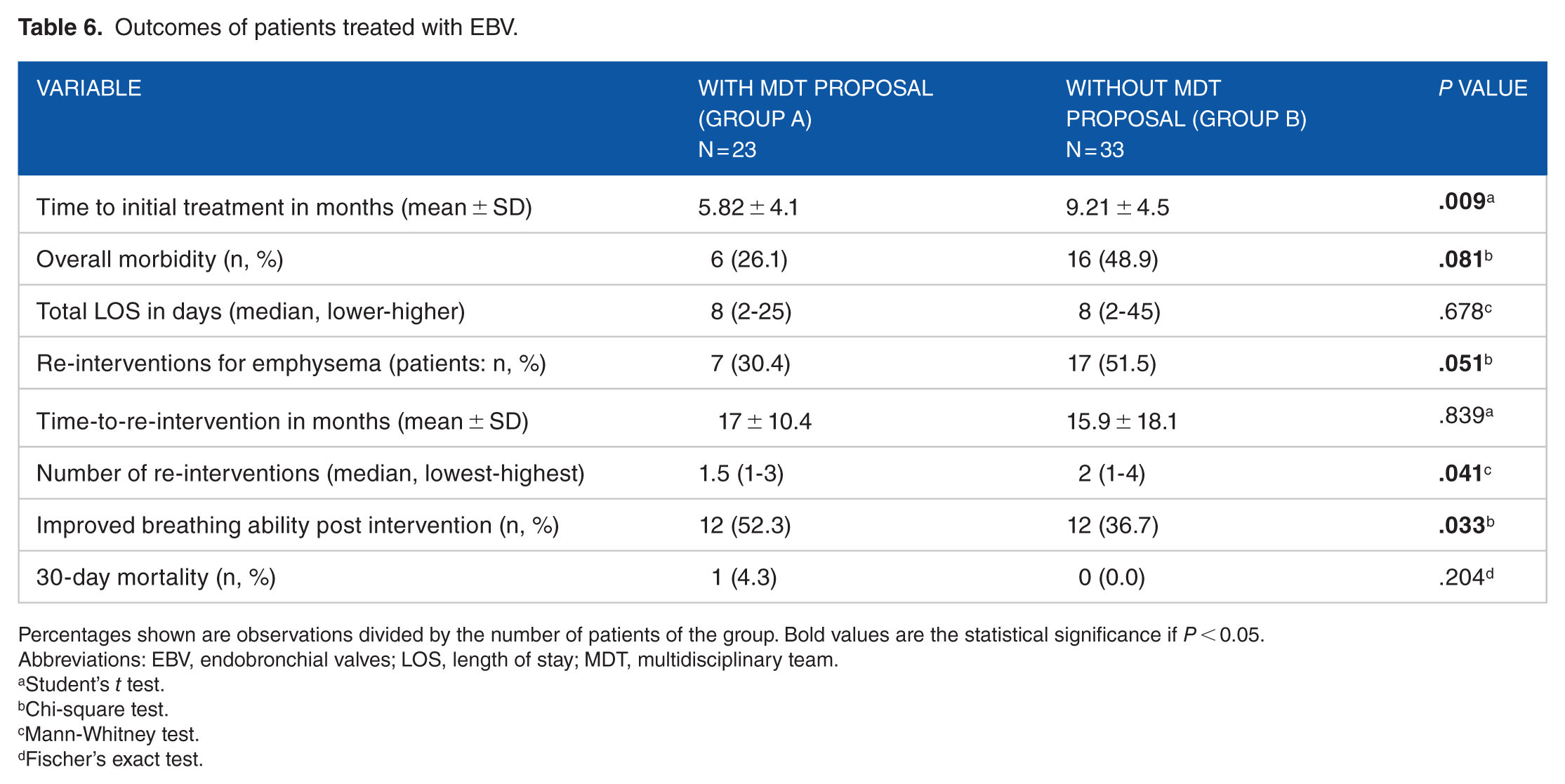
Percentages shown are observations divided by the number of patients of the group. Bold values are the statistical significance if P < 0.05.
Abbreviations: EBV, endobronchial valves; LOS, length of stay; MDT, multidisciplinary team.
Student’s t test.
Chi-square test.
Mann-Whitney test.
Fischer’s exact test.
Outcomes of patients treated with LVRS.

Percentages shown are observations divided by the number of patients of the group. Bold values are the statistical significance if P < 0.05.
Abbreviations: LOS, length of stay; LVRS, lung volume reduction surgery; MDT, multidisciplinary team.
Student’s t test.
Chi-square test.
Mann-Whitney test.
Fischer’s exact test.
Univariate analysis identified intervention without discussion at the MDT and initial intervention offered (if EBV) as potential predictors of re-intervention. On multivariate analysis, these factors remained strong predictors of re-intervention (Table 8). This model showed good fit (Cox-Snell R2 = 0.59% and Nagelkerke R2 = 68%).
Univariate and multivariate analysis of predictors of re-intervention.

Abbreviations: CAT, COPD assessment test; CI, confidence interval; DLCO, diffusional lung capacity for carbon monoxide; EBV, endobronchial valves; FEV1, forced expiratory volume in 1 second; MDT, multidisciplinary team; RV, residual volume; TLC, total lung capacity.
Bold values are the statistical significance if P < 0.05.
Up to the investigated date, 13 patients died from group B and 6 from group A (P = .070). Apart from the 30-day mortality cases described prior, the rest of the patients died due to disease progression and mainly from respiratory issues. However, no survival differences by time could be calculated between the 2 groups (log-rank test P = .884, Figure 2).

Survival probability according to discussion or not at the dedicated MDT. MDT indicates multidisciplinary team.
Discussion
The main finding of this study was that the emphysema MDT implementation changed the practice of interventional treatment of patients with emphysema by offering more LVRS as initial intervention and by offering the intervention at a later stage of the disease progression. In addition, the implementation of the emphysema MDT changed the outcomes of our practice by decreasing the number of re-interventions, increasing the re-intervention-free interval, and improving the breathing ability of the patients post-intervention. However, these did not affect the LOS, the morbidity, the 30-day mortality, and late mortality.
Based on the aforementioned findings, our initial experience on the impact of this recently implemented emphysema MDT shows that it has changed our practice of the treated patients with emphysema. The implementation of such an MDT has previously been shown to assist in the development of a successful LVRS programme. 13 In our study, a discussion at this MDT was proved to be an independent factor of re-intervention.
The re-intervention data were investigated in this study as an important outcome measure. Emphysema/COPD is not a curable disease and it is characterized by disease progression, including exacerbations over the years despite the best available care.15-17 This fact, apart from its financial aspect, impacts massively on the patients’ quality of life. 18 Re-interventions in patients who have already received interventional treatment, after having reached the ceiling of improvement with medical treatment, should be another indicator of initial correct decision making, appropriate timing of intervention, and adequate support thereafter, because it directly correlates with their quality of life.
More LVRS were performed when the MDT was involved in the decision making. Recommendations regarding LVRS or EBV interventions in stable patients with severe emphysema do exist.6,9,14,19,20 However, based on the fact that a referral pathway has not been finalized yet and that the emphysema MDTs, if existing, have not yet been proven to be beneficial, 12 many physicians prefer to practice as per preference. In addition, caring for a breathless patient who is seeking relief, without the contribution of an MDT, intensifies the pressure to provide an option of treatment, with that usually being, at least initially, the least invasive one, ie, EBVs. The EBV as initial treatment was an independent predictor of re-intervention but, without an MDT discussion adjusted for EBV as initial treatment, was not (Table 4). Therefore, these 2 factors were not correlated in our study. This finding suggests that in patients who can have both LVRS or EBV (as patients were matched for pre-interventional criteria), the initial intervention offered is a crucial event that enhances the need of a dedicated emphysema MDT implementation in this decision.
This study also shows that patients received their initial intervention in a more delayed manner when the MDT was involved in the pathway of care. One could argue that a referral takes longer, and for the MDT to reach a decision, numerous investigations are required, resulting in the delay of treatment. Even if this is valid, it must be borne in mind that the optimal time to offer the intervention, for the patient to experience its full benefit and for the longer period of time possible, is not yet known. Proceeding to an intervention fairly early in the progression of the disease could potentially abolish the benefits of this intervention at large. As health providers will accept the implementation of this MDT, it is expected that the referral and waiting times until a decision is made will be diminished.
We believe that the role of the MDT will augment the holistic consideration of each case, to minimize unnecessary interventions that are mainly performed under general anaesthesia and to offer interventions when appropriate. Bearing in mind that the patients referred for treatment have usually borderline respiratory reserve, one more intervention (even if performed under sedation) could potentially jeopardize their safety. 21 All these are supported additionally by the fact that practice changed towards more LVRS procedures in a delayed manner, after the MDT implementation. This event leads to the conclusion that the initial intervention needs to be tailored to each patient, taking under consideration the characteristics of each proposed intervention as well as the correct timing of the intervention. Overall, the involvement of the MDT in the pathway of care is more than just a proposal of initial treatment. In this way, the patient experiences the benefit of the intervention for the longest possible period of time, thus avoiding another intervention for as long as possible. 5
More patients treated after a discussion at the MDT reported that their breathing ability improved after the intervention. This is a crude and subjective way of measuring improvement and ideally an objective measurement should be performed, ie, the CAT score or the refined ABCD assessment tool when possible.18,19,22,23 Unfortunately, this was not possible because in the group of patients without a discussion at the MDT, an objective assessment of the symptoms or activities of the patients was rarely documented. Standard follow-up investigations are expected to be set by the MDT, to provide a common way of monitoring and quantifying the impact of the interventions.
No survival differences were observed in this study; observation that was expected as emphysema is not a curable disease, as stated before, and the basic recommendations for managing these patients were followed even in the group that the MDT did not participate. Although not included in this study, there are cases in which the surgeon, after the initial procedure, referred the patients to the MDT for further plan.
One important limitation of the study is that it is a retrospective, small, and single institute study, investigating a short period of study time without long-term data. Second, no financial data could be provided at this point, ie, comparing a long in-hospital stay after a complicated LVRS with 3 short stays after EBV insertion and re-insertions. Definitely, more objective follow-up investigations should have been performed (ie, calculation of CAT score, new pulmonary function tests, etc). Finally, our department does not provide the choice of other means of endoscopically collapsing the lungs, for instance, the endobronchial lung volume reduction coils.
In conclusion, patients treated for emphysema after discussion at a dedicated MDT were offered more LVRS and presented less re-interventions for their disease, longer time to re-intervention, and better breathing ability postintervention. These findings reinforce the need for introduction of dedicated emphysema MDTs in clinical practice. Following the paradigm of the implementation of MDTs for lung cancer, emphysema MDTs can establish the safety of interventional measures in the armamentarium of emphysema treatment.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
VK conducted the study and wrote the manuscript, PT and NC reviewed the data, changed and edited the manuscript, RM, EK, KP, AB, SK, DD, AH edited the manuscript