
Abstract
Background:
Uterine fibroids are common benign smooth muscle tumours that may complicate pregnancy with pain and pressure symptoms. While conservative management is preferred due to the risk of haemorrhage and pregnancy loss, antepartum myomectomy may be indicated in selected cases with intractable symptoms.
Case Presentation:
We report 2 cases of successful antepartum myomectomy performed in the second trimester for severe, unrelenting pain secondary to large fibroids. The first case involved a 27-year-old primigravida at 15 + 2 weeks’ gestation with a 22 × 16 × 17 cm pedunculated fibroid causing respiratory compromise. The second case involved a 41-year-old multigravida at 14 weeks’ gestation with multiple fibroids, the largest measuring 19 × 21 cm. Both patients underwent open myomectomy following multidisciplinary evaluation and counselling. Estimated blood loss was minimal, and postoperative recovery was uneventful. Pregnancies progressed to term, resulting in favourable maternal and fotal outcomes.
Conclusion:
Antepartum myomectomy, though rarely indicated, can be safely performed in well-counselled, carefully selected patients with severe symptoms and favourable fibroid characteristics. Preoperative imaging, multidisciplinary planning and meticulous surgical technique are crucial for optimal outcomes.
Introduction
Fibroids are benign tumours of the uterine muscle and common among women of reproductive age. Although fibroids that are present during pregnancy are largely asymptomatic, they can complicate pregnancy, with pain as the most common symptom. Conservative management is the standard of care in most cases until after delivery due to the risk of significant haemorrhage and disruption of the pregnancy. However, antepartum myomectomy may be indicated in rare cases when there is intractable pain and/or unbearable pressure symptoms such as respiratory compromise that cannot be treated with when conservative measures. In this article, we present 2 cases of antepartum myomectomy to increase the knowledge on indication for this procedure, including its surgical considerations. This information should broaden the management options that patients have, including elective pre-pregnancy myomectomy in women with large uterine fibroids to minimise complications associated with fibroids during pregnancy.
Case Presentation
Case 1
A 27-year-old Afro-Caribbean patient (primigravida at 15 + 2 weeks of gestation) with a body mass index (BMI) of 21.0 kg/m2 was referred with a 2-month history of recurrent abdominal pain of worsening severity. She described the pain as the ‘worst ever’ at the peak of episodes. She stated it radiated to her lower back with little or no relief with non-opioid and opioid analgesics. She also complained of poor sleep as she could only sleep in the cardiac position due to the significant pressure of the uterus and fibroid on the diaphragm in the recumbent position. She had been admitted to the hospital multiple times for pain management. She had no other personal or family medical history of concern. On examination, though limited by pain and poor patient positioning, her abdomen was grossly distended with palpable mobile abdominopelvic mass.
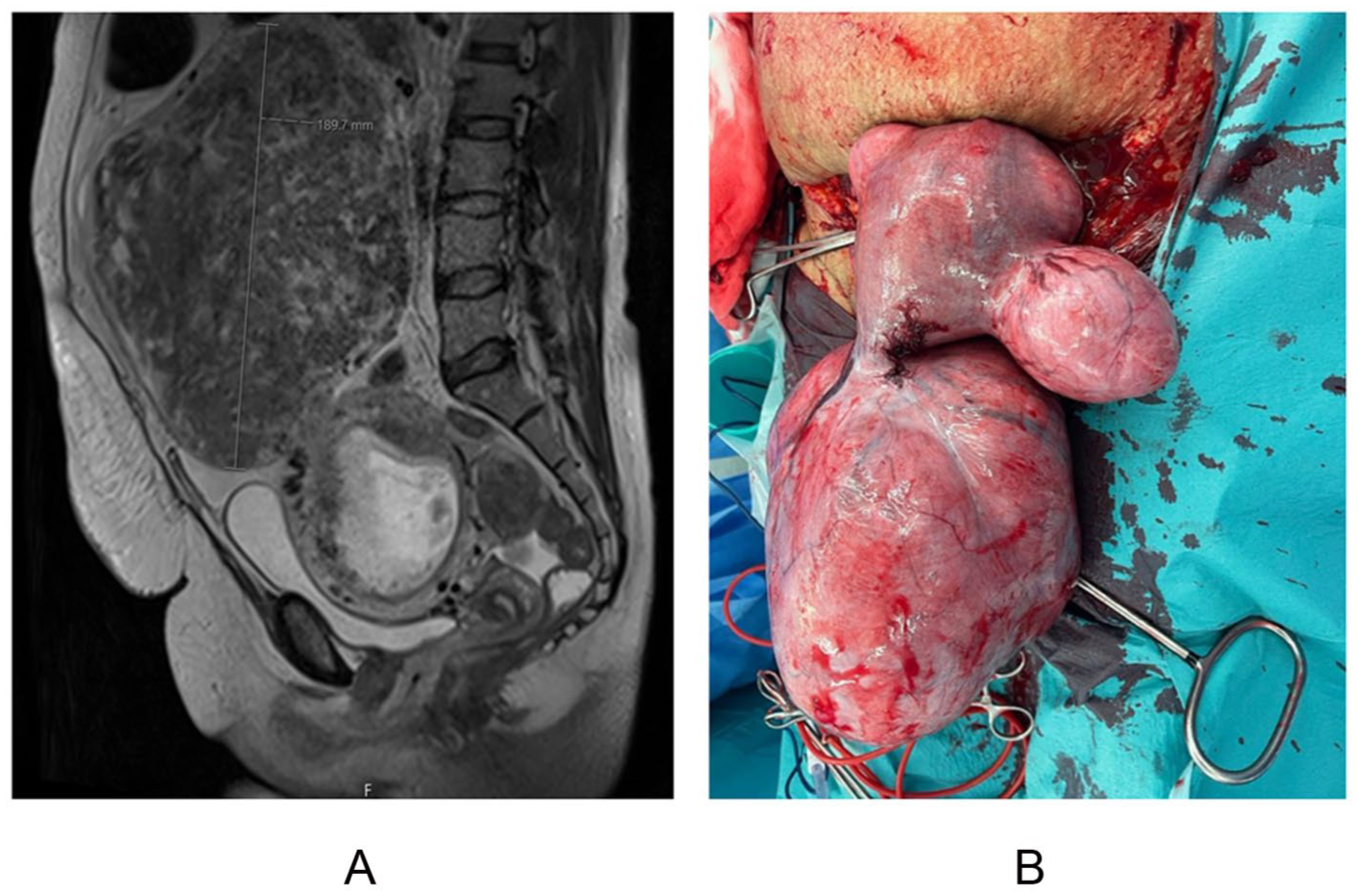
Magnetic resonance imaging (Figure 1A) revealed a large pedunculated fibroid superior to the uterus on the right side measuring 22 × 16 × 17 cm, with multifocal degenerative changes and no sign of malignant transformation, and a subserosal anterior wall fibroid measuring 6.5 cm at the widest diameter. The foetus was visualised in utero. A fibroid multidisciplinary team meeting recommended antepartum myomectomy in view of worsening cardiorespiratory compromise and pain. Following a detailed discussion with the patient about the risks and benefits of conservative versus surgical management especially increased risk of pregnancy loss and life-saving hysterectomy, she consented to have an open myomectomy.

Case 1: (A) preoperative MRI and (B) postoperative specimen.
The myomectomy was performed on the sixth day of admission under general anaesthesia through a midline incision. The 22 cm myoma was removed from the peritoneum, and 30 ml of diluted argipressin (prepared by diluting 20 IU in 200 ml of normal saline) was injected into the pedicle to prevent an inadvertent intravascular injection. The smaller 7 cm FIGO stage 6 fibroid was also enucleated. The myometrial incision was closed in layers with Vicryl 1/0 suture to ensure no dead space while avoiding the endometrium and Monocryl 3:0 to serosal layer. Floseal was applied over site of uterine incision to ensure haemostasis. The total estimated blood loss was 150 ml. She made an uneventful recovery and was discharged on postoperative day 2. Her pregnancy progressed uneventful, 20-week ultrasound showed anterior high placenta. She had ventouse vaginal delivery at 40 + 0 weeks with fetal weight of 2795 g and APGAR score of 9 and 10 in the first and fifth minute.
She was seen at the sixth week postnatal clinic and had no concern. She is currently pregnant and being managed in a consultant-led care unit.
Case 2
The patient was a 41-year-old Asian woman – gravida 4, para 3 and at 14 weeks gestation. Her current pregnancy was unplanned but desired (her last pregnancy was 16 years earlier). She presented with worsening abdominal pain with no urinary or bowel symptoms. She had a history of a 10.2 cm asymptomatic uterine fibroid diagnosed 6 months prior to presentation. She had a previous caesarean birth. Her other personal and family history did not indicate any concerns.
The examination revealed that she was in obvious pain despite taking multiple analgesics, including morphine administered every 2 to 4 hours. Her abdomen was distended with an abdominopelvic mass that extended midway between the umbilicus and the xiphisternum. The mass was mobile and tender, factors that limited the examination.
An urgent ultrasound scan revealed multiple fibroids. The largest was a right fundal subserosal fibroid measuring 19.9 × 14.2 × 16.5 cm. There was also a large left lateral fibroid measuring 8.3 × 8.2 × 5.7 cm. The scan also showed a single viable intrauterine pregnancy. Abdominopelvic MRI (Figure 2) showed a bulky multifibroid uterus measuring 29 × 16 × 20.5 cm with a large subserosal fibroid measuring 19 × 21 cm; a subserosal/pedunculated fibroid (8.3 × 7.6 cm); a subserosal fibroid (4.6 × 3.7 cm); and several other small fibroids. There was no evidence of sarcomatous degeneration. A singleton intrauterine fetus was seen.
Case 2: (A) preoperative MRI and (B) intraoperative finding.
Because her pain remained without any relief or break, she was offered an open myomectomy following a multidisciplinary meeting. The risks of bleeding, pregnancy loss, hysterectomy and uterine scar dehiscence were explained to her before obtaining her consent. The intraoperative findings included a 12-week-sized uterus with a 20 × 15 cm pedunculated fibroid (not torted), 5 × 5 cm left fundal subserosal fibroids, a 5 × 5 cm posterior subserosal fibroid and other small seedlings. The large pedunculated fibroid showed omental adhesion. The large pedunculated fibroids were resected from their stalk after injection of vasopressin (20 IU diluted in 100 ml of normal saline). The subserosal fibroids were enucleated. The cavity was closed in layers to ensure haemostasis. Floseal was applied over the uterine incision, and tranexamic acid (1 g, intravenous) was given to ensure haemostasis. Fibroid and omental biopsy specimens were sent for histology, which showed benign leiomyoma with hyaline degeneration and marked red degeneration. She was subsequently discharged on postoperative day 5 after making an uneventful recovery. Pregnancy progressed uneventfully with no concern of placental location or placenta accreta spectrum. She delivered via an elective caesarean section at 38 + 1 weeks due to the risk of uterine rupture with tubal sterilisation as she requested a permanent method of contraception. A 3255 g female infant was delivered with Apgars score of 10 and 10 in first and fifth minute.
The patients expressed profound satisfaction with the multidisciplinary care they received, emphasising the compassionate support and clear communication provided throughout their pregnancy from a surgical emergency to achieving their desired obstetric outcomes. Her sixth week postnatal visit was uneventful and was subsequently discharged from the outpatient clinic.
Discussion
Uterine fibroids or myomas (leiomyomata uteri) are histologically defined as benign monoclonal tumours of the smooth muscles and fibroblasts of the uterus. They contain large amount of extracellular matrix (collagen, proteoglycan and fibronectin) with a thin pseudo-capsule of areolar tissue and compressed muscle fibres. 1 They are the most common pelvic tumours in women of reproductive age and have an incidence of 10.7% during pregnancy.2,3 Fibroids are usually asymptomatic during pregnancy; when symptoms do occur, they include pain, pressure symptoms and vaginal bleeding.
Pain is the most common symptom of uterine fibroids during pregnancy and, according to one study, was responsible for 11% of hospital admissions. 4 That same study indicated that the frequency of admission for pain management increases as the size of the fibroid increases. The authors reported that up to 23% of fibroids were 7 to 10 cm in diameter. 4 Red degeneration of uterine fibroids is commonly responsible for pain in pregnancy and typically presents in the late first or early second trimester, which corresponds to the period of greatest fibroid growth and, in turn, the propensity to degeneration. 5 Red degeneration may also be associated with mild leucocytosis, fever and nausea and vomiting, perhaps due to the release of prostaglandins. 6 Large fibroids lead to early pregnancy loss, preterm labour, placental abruption, malpresentation, placenta praevia, dysfunctional labour, caesarean birth and postpartum haemorrhage, among other complications.
Conservative management is considered the gold standard of treatment of fibroids during pregnancy. Successful use of epidural analgesia for severe pain refractory to other therapy have been described. 7 The general approach is to avoid myomectomy during pregnancy, especially when an intramyometrial incision is required, unless the procedure cannot be delayed such as in deteriorating clinical state. The 2 patients described in this case report were offered antepartum myomectomy due to their intractable pain (it could not be relieved with analgesia), pressure symptoms and the pedunculated and serosal locations of the fibroids. The procedures were done midtrimester as this has been historically considered the best time for elective surgery during pregnancy due to a reduced risk of spontaneous miscarriage compared with the first trimester, and a reduced incidence of preterm labour and delivery compared with the third trimester.8,9
For both patients, a multidisciplinary team was responsible for comprehensive surgical planning. This process was supported by counsellors and included informing the patients of the potential complications of the surgery. MRI mapping of the myomata served as an important tool in surgical planning. MRI has proven to be essential for surgical planning as it helps determine the size, location and number of fibroids. This imaging modality also allows clinicians to determine the characteristics of the fibroid, the presence of other pathology and their anatomical relationship to other structures, especially the foetus. 10 Laparotomy is the most used approach during antepartum myomectomy, although laparoscopy has also been reported.9,11 A midline abdominal incision was used in both cases due to fibroid uterus size, greater access and minimal handling while exteriorising the pregnant uterus.
Haemostasis, prevention of impaired uterine perfusion and the prevention of uterine contraction are among the most feared complications during antepartum myomectomy. To minimise blood loss, the patients were given preoperative intravenous tranexamic acid, and argipressin was injected into the stalk closer to the fibroid than the gravid uterus. Note that some authors feel this may compromise placental blood flow. 5 Floseal, a gelatine thrombin matrix sealant, was used over the uterine incision to further achieve haemostasis. A short course of indomethacin – a non-selective cyclooxygenases inhibitor and a potent analgesic – was administered to prevent myometrial contractility and pregnancy loss with an incidence of 5.2% reported in a systematic review. 9 This short course offered was to reduce the fetal complications of oligohydramnios, pulmonary hypertension and platelet dysfunction. 6
Some limitations to this report include the number of cases presented which limits the generalisability of findings and comparison to other treatment options. The severity of symptoms and characteristics of fibroid helped in decision making, and this may introduce selection bias as a predominantly intramural fibroid may constitute greater risks such as bleeding, pregnancy loss. Cost constraints in low resource setting may limit the availability of MRI which is essential in surgical planning.
This article is aimed to broaden the conversation on antepartum myomectomy (ie, the indications, techniques and surgical pitfalls) in carefully selected cases and well-counselled patients. It also highlights the possible complications of large uterine fibroids during pregnancy and the consideration of pre-pregnancy myomectomy of large uterine fibroids. The physiological changes that the uterus undergoes during pregnancy may trigger acute symptoms in previously asymptomatic large uterine fibroid, thus requiring surgical intervention during pregnancy. This should be carefully balanced with the associated risk of intrauterine and pelvic adhesions which may compromise fertility. Previous myomectomy also increases risk of uterine rupture, preterm birth and placenta accreta syndrome. 12 There is a consensus on removal of uterine cavity fibroid in women planning assisted reproductive conception. 13
Conclusion
The cases presented illustrate that removal of uterine fibroid during pregnancy although generally avoided, can be a management option in carefully selected patients with refractory symptoms unresponsive to conservative management. A thorough preoperative evaluation in a multidisciplinary setting with consideration of patient’s preferences and expectations, surgical removal of pedunculated or subserosal fibroid may provide symptomatic relief and support successful obstetric outcomes. The report also highlights the importance of counselling women with known large fibroids about potential pregnancy-related issues and possible need for surgical intervention. Although current evidence is still limited, these cases add to research suggesting that myomectomy during pregnancy could be a reasonable option for certain patients experiencing persistent pain, rapid fibroid growth or risks to maternal health. More extensive studies and long-term follow-ups are needed to clarify indication for this procedure, improve surgical methods and better understand its effects on future fertility.
Footnotes
Acknowledgements
The authors wish to acknowledge the contributions of the multidisciplinary teams involved obstetrics, gynaecology, anaesthesia, radiology among others for their expertise and coordination in management of these cases. We also appreciate the patients for their willingness to allow their clinical experiences to be shared for the advancement of medical knowledge.
Consent to Participate
The case report has been fully explained to the patients, and all questions answered to their satisfaction. The patients have been informed of the risks and benefits, if any, of allowing their information to be used in this case report.
Consent for Publication
Consent to publish the information has been obtained from the patients.
Author Contributions
GIT: original manuscript writing, manuscript review and editing. AN: operating surgeon and lead consultant, manuscript review and editing. MS: manuscript review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.