
Abstract
Pneumatosis intestinalis (PI) is characterized by the presence of air within the walls of the small intestine, large intestine, and sometimes the gastric wall. The mechanism and pathogenesis of PI are poorly understood. The discovery of PI can occur in the form of an incidental finding, such as a benign course or a life-threatening condition, such as intestinal ischemia. Point-of-care ultrasonography (POCUS) for pneumatosis intestinalis (PI) is rarely reported in adults, with only 1 previous poster presentation. However, POCUS is well-documented in the pediatric population, particularly for the diagnosis of intussusception. We present a 78-year-old man with longstanding uncorrected severe pulmonary stenosis, right-sided heart failure, atrial fibrillation on dabigatran, diabetes, and cirrhosis who presented with progressive abdominal distension. POCUS and computerized tomography of the abdomen showed ascites, diffusing small-bowel wall thickening with edema, and pneumatosis intestinalis, without portal venous gas or vascular occlusion. Patient was transitioned to palliative care on diuretics, lactulose; follow-up ultrasound showed only mild ascites but persistent small-bowel PI. This case report marks the second instance of POCUS being utilized for PI in an adult population. POCUS can play an essential diagnostic role at the bedside, ruling out serious underlying etiologies and guiding physicians in further diagnostic testing.
Keywords
Introduction
Gas in the intestinal wall, known as pneumatosis intestinalis (PI), is typically observed by imaging modalities such as plain abdominal X-rays or computed tomography (CT). 1 This condition can arise from various underlying diseases of varying significance, ranging from a serious illness to an incidental, benign finding. 1
We are sharing this case of advanced liver cirrhosis with anticoagulation therapy because of underlying atrial fibrillation (AF). Point-of-care ultrasound (POCUS) revealed the presence of the PI. CT of the abdomen ruled out intestinal ischemia and confirmed that the PI was benign. This case highlights the importance of POCUS in evaluating the PI in adult patients within the context of their overall clinical picture.
Case Presentation
A 78-year-old man with a history of uncorrected congenital heart disease (severe pulmonary stenosis since age 18) and severe pulmonary hypertension with right-sided heart failure presented with progressive abdominal distension and lower limb edema. His past medical history also included paroxysmal atrial fibrillation on 110 mg dabigatran twice daily, diabetes mellitus on dapagliflozin, and liver cirrhosis with portal hypertension and ascites (high serum albumin ascites gradient (SAAG)) for 10 years.
The results of the laboratory tests revealed a total protein concentration of 52 g/L (normal range: 60-83 g/L), an albumin concentration of 33 g/L (35-55 g/L), and a lactate concentration of 1.2 mmol/L (less than 2.0 mmol/L).
Point-of-care ultrasound (POCUS) revealed significant ascites and hyperechoic dots within the wall of the small bowel, suggestive of a small bowel wall air bubble (pneumatosis intestinalis (PI)), Figure 1, Supplemental Video 1). The small and large intestines were normal in diameter and exhibited active peristalsis. No air in the portal vein was detected. Computerized tomography (CT) of the abdomen revealed a normal caliber and distribution of the celiac, superior mesenteric, and inferior mesenteric arteries with satisfactory postcontrast opacification (Figure 2). No intestinal vascular filling defects were detected. However, diffuse thickening and edema of the small bowel loops were noted, along with a few air locules within the bowel wall.

Ultrasound of small bowels showing free air (long arrows) within the wall.
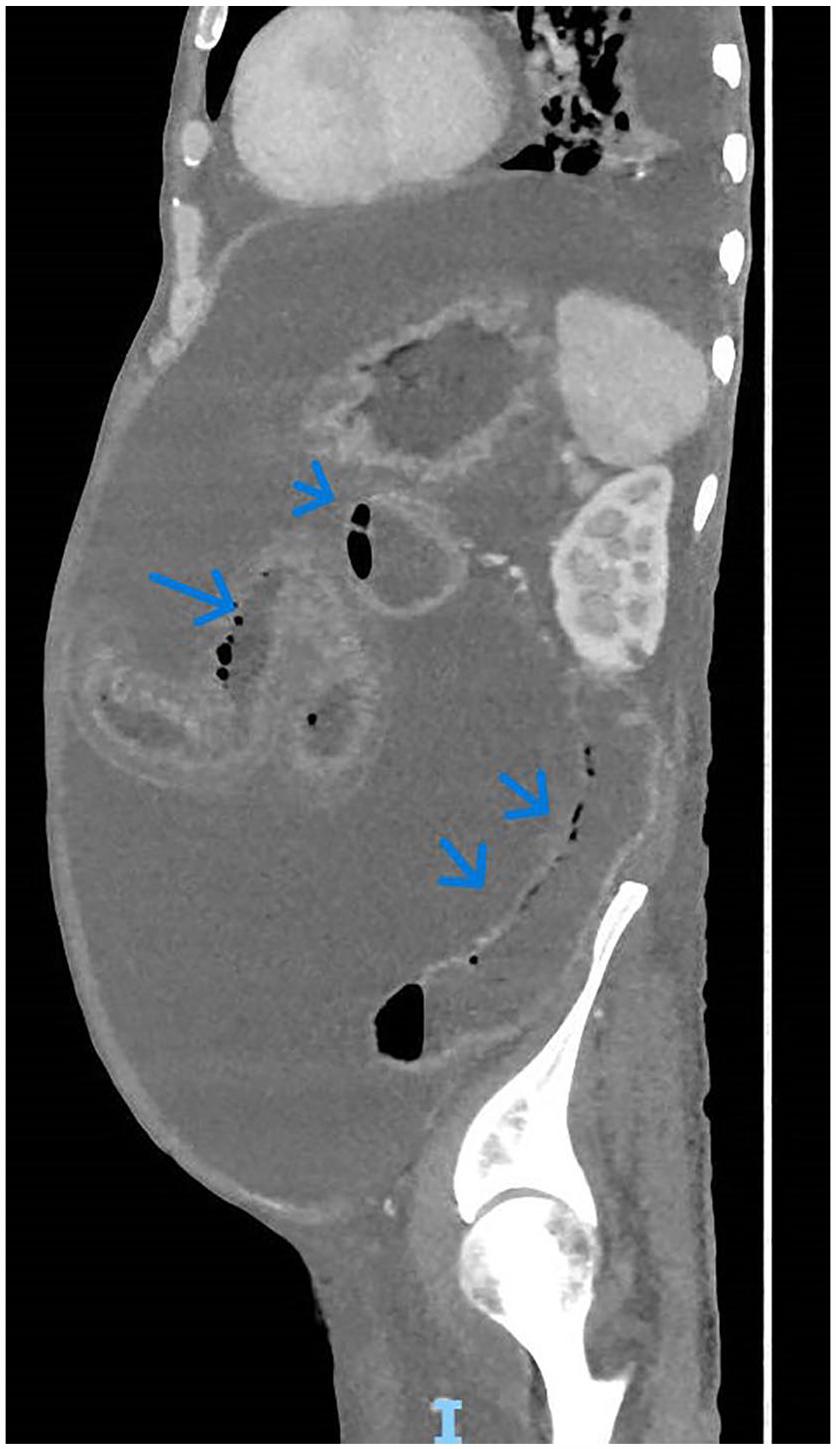
Abdominal computerized longitudinal image with extraluminal gas tracking along the small bowel wall (arrows).
Abdominal tapping revealed bloody fluid, with no white blood cells and many red blood cells, with a high SAAG. Three liters of this fluid were drained.
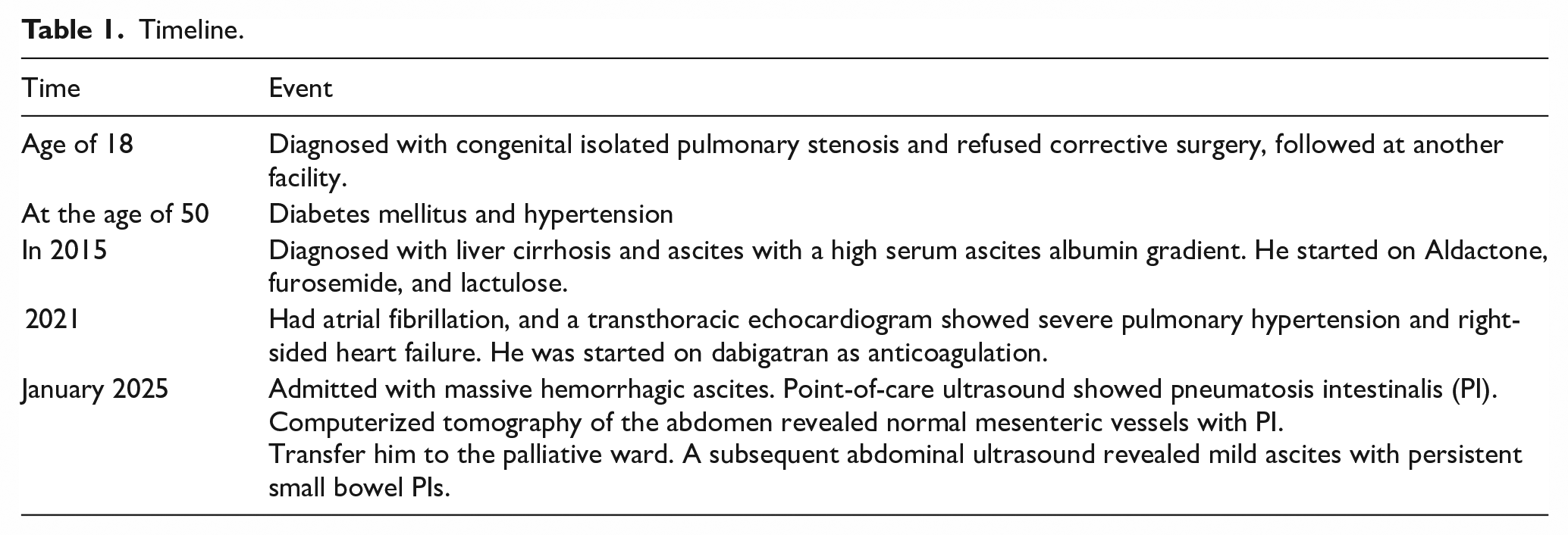
Given the patient’s overall condition, the family agreed to transfer him to the palliative ward. He was maintained on diuretics, lactulose, and spironolactone. A subsequent abdominal ultrasound revealed mild ascites with persistent small bowel PIs (Table 1).
Timeline.
Discussion
PI is a gut condition in which gas accumulates under the mucosa or submucosa of the intestinal wall. PI is a finding of uncertain significance unless correlated with other clinical and radiological evaluations and can include both life-threatening ischemic bowel and benign pneumatosis associated with other conditions, chronic obstructive pulmonary disease, immunosuppression, endoscopic intervention, and bone marrow transplantation. 2 PI has been reported in chronic lactulose use and after liver transplantation.2,3 The incidence of PI after adult living donor liver transplantation is approximately 1% and usually involves the right ascending colon. 2 Most patients recover with supportive care. 4 PI has been reported as a complication of connective tissue disease and is attributed to high H2 production. 5
The use of bowel ultrasound narrows the differential diagnosis and expedites care in patients presenting with abdominal pathology, with comparable diagnostic accuracy to CT in certain types of abdominal pathology. The underlying serious conditions include small bowel obstruction (SBO), inflammatory bowel disease, and diverticulitis.6 -8
The use of POCUS is on the rise in areas with limited resources. The adoption of POCUS is largely due to the growing availability of affordable, portable ultrasound devices and the development of standardized, evidence-based procedures. 9 In many of these settings, POCUS is often the sole imaging tool accessible, making it a potentially transformative asset for patient care. 9 POCUS has been commonly used for common health issues, including pediatric pneumonia, extrapulmonary tuberculosis, ectopic pregnancy, and various tropical parasitic diseases like echinococcosis, schistosomiasis, and amebiasis. The existing literature suggests that POCUS holds significant promise for improving both the diagnosis and treatment of numerous medical conditions in these challenging environments. 9
The role of ultrasound in PI was first described in the radiology field in 1985. 10 In summary, intramural gas can be diagnosed by ultrasonography, and in some instances, it may even be more sensitive than plain radiographs. Clinically, the true value of recognizing this sign is in the early diagnosis of bowel ischemia. The use of POCUS for diagnosing PI in adults has been rarely reported, with only a single poster presentation previously documented. 11 However, POCUS is well described in the pediatric population, especially in cases of intussusception. 12 The present case report is the second case report in which POCUS was used for PI in an adult population.
Ultrasonography can also be used to detect PI, as noted in the radiology literature.10,13 The ultrasonography identifies PI as either linear or focal echogenic regions within the bowel wall. Additionally, it may present as a continuous echogenic ring surrounding the intestine wall.14,15 Gases within the intestinal tract lumen are typically mobile and shift with the peristaltic movement of intestinal contents. 14
The presence of additional findings, such as bowel wall thickening, dilated bowel, ascites, and hepatic portal or porto-mesenteric venous gas, increases the possibility of PI due to a life-threatening cause.16,17 PI that is confined to a portion of the small or large bowel within a specific vascular distribution also increases the likelihood that ischemia is the cause of PI. 16
The finding of bloody ascitic fluid with a high SAAG, in the context of PI, raised concerns for potential bowel ischemia that CT of the abdomen has ruled out despite the absence of other overt signs.
Limitations
This is a single-case report, which limits generalizability; however, it is the first time this condition has been reported in the adult population using POCUS. While pneumatosis intestinalis (PI) was identified, the report does not fully clarify its underlying pathophysiology in this context. The presence of multiple comorbidities (uncorrected congenital heart disease, severe pulmonary hypertension, liver cirrhosis, and atrial fibrillation) makes isolating causal relationships for PI challenging.
Conclusion
POCUS, as a bedside tool, enables physicians to determine whether the PI is a benign condition or a catastrophic condition, and is clinically directed, followed by evaluation for the presence of dilated bowel, abnormal peristaltic movement, and portal vein gas. CT abdomen confirmation remains the gold standard, and any ultrasonographic findings should be interpreted with caution in the context of the clinical picture and physical examination.
Footnotes
Acknowledgements
We thank the Management of Ahmadi Hospital, Chief Clinical Officer Dr. Ibrahim Al-Kandary, and Manager Dr. Mobarak Alajmi for their support in preparing this report.
Consent to Participate
The patient provided written informed consent and was permitted to publish his Clinical history.
Author Contributions
ZB: Project Administration, Conceptualization, writing the original draft, and Validation. OM: Investigation, review, and editing. MAF: Data Curation, Methodology. BA: Validation, Investigation, and resources.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing does not apply to this article, as no datasets were generated or analyzed during the current study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.