
Abstract
Pneumatosis intestinalis is a characteristic imaging phenomenon indicating the presence of gas in the bowel wall. The link between pneumatosis intestinalis and various kinds of autoimmune diseases has been reported anecdotally, while information regarding the cases with antineutrophil cytoplasmic antibodies (ANCA)–associated vasculitis complicated by concurrent pneumatosis intestinalis is lacking. In this report, we describe our serendipitous experience with one such case of pneumatosis intestinalis in a patient with ANCA-associated glomerulonephritis. We also discuss several therapeutic concerns that arose in the current case, which had an impact on the pathogenesis of the disease.
Keywords
Introduction
Pneumatosis intestinalis is a characteristic imaging phenomenon indicating the presence of gas in the bowel wall.1,2 It represents a wide spectrum of conditions, ranging from the innocuous to the fatal.1–3 In this report, we describe our serendipitous experience with a case of pneumatosis intestinalis in a patient with a recent diagnosis of antineutrophil cytoplasmic antibodies (ANCA)–associated glomerulonephritis. Several concerns regarding the pathogenesis of the disease in this patient are also discussed.
Case Report
A 75-year-old male was admitted to our hospital in the middle of February 2013 due to rapid deterioration of his renal function, general fatigue, and myalgia in his lower extremities. Although he had no history of renal disease, his serum creatinine (sCr) level was 0.9 mg/dL at the end of January 2013 and increased to 1.2 mg/dL at the beginning of February 2013. Four years prior to admission, the patient was found to have rectal carcinoma, which was treated successfully with surgical removal combined with transient postoperative chemotherapy. He had smoked for more than 20 years until 54 years of age, while he denied any history of drug abuse. The laboratory data obtained on admission are summarized in Table 1.
The laboratory data on admission.

An increase in the titer of antimyeloperoxidase–ANCA (MPO-ANCA) above 300 U/mL, but no increase in anti-proteinase 3–ANCA (PR3-ANCA) or antiglomerular basement membrane (GBM) antibodies, was also found, while tests for the presence of antinuclear antibodies, hepatitis B virus surface antigens (HBsAg), anti-HBsAg antibodies, and hepatitis C virus antibodies were all negative. No abnormal findings were detectable in either the chest or abdominal X-rays (Fig. 1A). A urinalysis revealed a urine protein level of 3

The serial chest and abdominal X-ray findings during the observation period. No abnormal findings were detectable on admission (
A renal biopsy performed 4 days after admission contained five cores of renal parenchyma with 23 glomeruli, 2 of which were globally sclerotic. Although vasculitic changes were absent in the blood vessels, cellular crescent formation was seen in the rest of the glomeruli, some of which exhibited a break in the GBM associated with fibrin extravasation (Fig. 2). An immunofluorescence analysis demonstrated a lack of immunoglobulin and complement deposition within the glomeruli. Based on the laboratory and pathological findings, the patient was diagnosed to have MPO-ANCA–associated glomerulonephritis, and oral prednisolone (PSL) at a dose of 40 mg/day was started. Despite the improvement of his general status and the successful relief from myalgia, his renal function gradually worsened, and intravenous pulse therapy with methylprednisolone at 500 mg/day was given for three consecutive days from the 22nd hospital day, when his sCr had increased up to 1.92 mg/dL.

Photomicrographs of the renal biopsy specimen. A light micrograph showed cellular crescent formation in several glomeruli (
At almost the same time, the cytomegalovirus (CMV) anti-genemia assay with monoclonal antibodies C10/C11 revealed that the patient had a CMV infection. He was subjected to preemptive treatment with ganciclovir, which was continued until the CMV antigen assays became negative. The peak titer of CMV antigenemia (CMV Ag) was 2/5 when the treatment had been terminated for 1 week, because we gave priority to treatment with oral famciclovir for a concurrent herpes zoster infection that developed on the 27th hospital day (Fig. 3). A laboratory analysis revealed that the patient had postprandial hyperglycemia (290 mg/dL) 12 days after the initiation of oral PSL, leading to a diagnosis of steroid-induced diabetes. Then, voglibose (single dose of 0.3 mg, given three times a day just before each meal) treatment was commenced on hospital day 18, resulting in good glycemic control.

The clinical course of the current patient. A prompt decrease in the serum C-reactive protein level was confirmed just after the initiation of oral prednisolone, while the sCr levels began to decrease approximately 7 weeks after the initiation of corticosteroids treatment. Ganciclovir treatment for the CMV infection was transiently switched to oral famciclovir, when overt herpes zoster (characterized by a vesicular rash with a dermatomal distribution) developed. The time points corresponding to each panel in Figure 1 are demonstrated at the top.
A routine chest X-ray performed 5 weeks after he had started oral PSL suggested the presence of right cervical subcutaneous emphysema and pneumomediastinum, while an abdominal X-ray showed remarkable gas collections along the bowel wall (Fig. 1B). Although the patient did not have any respiratory or abdominal symptoms, subsequent chest and abdominal computed tomography (CT) scans demonstrated intramural air in the bowel, gas collection in the mesentery, and an abnormal air density in the mediastinum, as well as in the cervical subcutaneous regions (Figs. 4A–E). Voglibose was ceased, and fasting was imposed when a diagnosis of pneumatosis intestinalis was made. Subsequently, fluid supplementation and oxygen inhalation were started, while a reduced dose PSL of 20 mg/day was continued. Thereafter, the radiological indications of the disease were gradually improved and were no longer present on the 57th hospital day, despite the resumption of normal dietary intake (Figs. 1C–E). His sCr levels were finally maintained around 1.9 mg/dL with 2-h postprandial blood glucose levels of 150–180 mg/dL when he was treated at the outpatient clinic with PSL at a dose of 15 mg/day, with a MPO-ANCA titer of 16.5–21.0 U/mL.
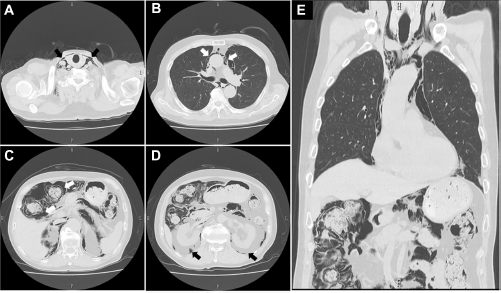
CT scans of the chest and abdomen. Abnormal air accumulations characterized by radiolucent areas (black or white arrows in each panel) were observed in the cervical regions (
Discussion
The combination of a rapid deterioration of the renal function and crescentic glomerulonephritis mediated by ANCA is a well-described clinical entity.4,5 The standard treatments for ANCA-associated vasculitis, which are based on the results of a series of clinical trials conducted by the European Vasculitis Study Group, consist of corticosteroids combined with oral or intravenous cyclophosphamide 6 ; however, there are some differences in the characteristics of Japanese ANCA-associated vasculitis patients compared with those in Europe. For instance, microscopic polyangiitis and MPO-ANCA are more common in Japan, while granulomatosis with polyangiitis and PR3-ANCA are more common in the United Kingdom.7–9 Meanwhile, it has been shown that the average age of such Japanese patients is high and the most frequent cause of death is infectious complications. 9 Thus, the Japanese clinical practice guideline for the disease has emphasized the need for reduced immunosuppressive treatment, such as a reduced dose of PSL with or without an immunosuppressant, and the concurrent application of cyclophosphamide has not necessarily been recommended.8,9 Consequently, the monotherapeutic protocol with corticosteroids applied in the current patient may not be surprising.
Despite the clinical benefit of corticosteroids on the overall management of ANCA-associated vasculitis,5–8 numerous adverse effects, including opportunistic infections and metabolic disturbances, have been attributed to the agents. 10 This was also the case in the current patient, since the treatment with PSL seemed to result in the improvement of renal function, but led to the concurrent development of CMV infection, herpes zoster infection, and impaired glycemic control, characterized by postprandial hyperglycemia. One may argue that the clinical and therapeutic manifestations of our patient are too common to describe in the literature. However, the clinical significance of the present report should be evaluated carefully in terms of the fact that he was subsequently complicated with cervical subcutaneous emphysema, pneumomediastinum, and air accumulation in the bowel wall, leading to a diagnosis of pneumatosis intestinalis.
Pneumomediastinum and cervical subcutaneous emphysema have been associated with a wide range of structural lung diseases, including asthma, emphysema, bronchiectasis, and interstitial lung disease, 11 while the simultaneous occurrence of pneumomediastinum and pneumatosis intestinalis with or without subcutaneous emphysema is not exceptional.12–15 Such a combination may result from alveolar rupture based on the pressure gradient between the alveoli and the lung interstitium, which leads air to pass along the vascular channels in the mediastinum, tracking caudally through the retroperitoneum and then to the mesentery of the bowel.2,3 However, our patient did not manifest any pulmonary symptoms such as cough, chest pain, or discomfort during the observation period, and thus, descending gas that originated from the lungs was considered to be a less likely cause in the current case. Rather, it appears that retroperitoneal air that had arisen from gas accumulated within the bowel wall escaped upward into the mediastinum and cervical subcutaneous area in the present patient, as has been described anecdotally.14,15
Numerous clinical conditions (Table 2) have been regarded to be underlying diseases associated with pneumatosis intestinalis.1–3 A vasculitis-based pathogenesis within the intestinal territory has been proposed as an etiological background for the development of the disease among select subjects with systemic lupus erythematosus. 12 A gastrointestinal tract involvement resulting from a vascular injury can be observed in patients with ANCA-associated vasculitis as well 16 ; however, the lack of systemic disease manifestations in our patient led us to attribute the patient's renal abnormalities to the renal-limited phenotype and to conclude that the clinical impact of a MPO-ANCA–mediated mechanism on the development of pneumatosis intestinalis might be marginal. Otherwise, the paucity of data regarding the occurrence of pneumatosis intestinalis in patients with ANCA-associated vasculitis may imply that such a vascular injury does not play a role as a predisposing factor equivalent to that of lupus, although the case of systemic vasculitis associated with PR3-ANCA, but not with MPO-ANCA, in a patient accompanied by the disease has been shown anecdotally. 17
Diseases and conditions associated with pneumatosis intestinalis.

We feel it is reasonable to consider that certain medications and comorbidities may have played a role in the development of pneumatosis intestinalis in our patient. The common candidates are corticosteroids, which have been suggested to deplete the lymphoid tissue within Payer's patches, leading to disturbances in the mucosal integrity which permits the dispersion of gas into the noninflamed bowel wall.2,18 Alternatively, or in addition, alpha-glucosidase inhibitors (AGIs) such as acarbose, voglibose, and miglitol, which delay the absorption of carbohydrates from the gastrointestinal tract by inhibiting AGI, thereby limiting postprandial plasma glucose excursions, 19 have also been reported to be associated with pneumatosis intestinalis.3,20 An increase in intraluminal pressure due to excessive gas production based on the bacterial fermentation of undigested carbohydrates in the bowel might result in the development of pneumatosis intestinalis. 20 Otherwise, concurrent opportunistic infections with CMV may have also predisposed our patient to the disease. Indeed, a presumable causal relationship between pneumatosis intestinalis and CMV infection has been mentioned anecdotally,21–23 and the primary cytopathogenic effect of CMV on the bowel mucosa or vasculitic reaction mediated by CMV infection may be implicated in the disease process. 23 Finally, we are of the opinion that the development of the disease in our patient could be attributed to the additive or synergistic effects of multiple factors, including the use of corticosteroids and voglibose, as well as CMV infection. The rapid radiological improvement, along with the disappearance of CMV antigenemia in the current patient after the cessation of voglibose and the dose reduction of PSL supports this assumption, although it is difficult to determine the precise contributions of each factor.
Despite the accumulation of anecdotal or systemic studies disclosing the nature of pneumatosis intestinalis,2,3,24 we feel that an early and accurate diagnosis, as well as awareness of the disease, remains a challenge for physicians. The current report apparently emphasizes the pitfalls of managing patients with ANCA-associated glomerulonephritis who are treated with corticosteroids. The validity of the treatment with AGIs for the steroid-induced diabetes, which is occasionally reported in subjects with ANCA-associated vasculitis, 10 may also need to be evaluated carefully, even if there are only few subjects who may benefit from such agents. 25 No specific surgical approach may be required in asymptomatic cases, while there are some subsets of patients who require urgent surgical intervention due to concurrent abdominal sepsis, perforation, or peritonitis.2,3,18,26 The establishment of an optimal diagnostic and therapeutic policy for the disease is clearly mandatory since the origin of the gas is occasionally unclear, and the patient's symptoms can be volatile, presenting a diagnostic dilemma for the surgeon in charge. 3
Author Contributions
Drafted the manuscript: SN, TA. Made contributions to the acquisition of the clinical data: ST, MO, AM, HY. Provided a detailed review of the contents and structure of the manuscript, resulting in significant changes to the original document: SM, EK, DN. All authors have read and approved the final manuscript.