
Abstract
Introduction:
Hepatic portal venous gas is a rare and life-threatening condition characterised by the presence of gas in the portal vein. Hepatic portal venous gas is frequently associated with intestinal ischaemia and necrosis. We present the case of a paediatric patient with acute appendicitis with hepatic portal venous gas detected using ultrasonography.
Case report:
A 5-year-old boy was admitted to our hospital with a respiratory tract infection. The boy started vomiting on day 2 of hospitalisation. He did not complain of any symptoms due to developmental retardation. We performed bedside point-of-care ultrasound, which detected hepatic portal venous gas, although the appendix could not be detected due to an acoustic shadow associated with bowel gas. Contrast-enhanced computed tomography revealed perforated appendicitis and pneumatosis intestinalis associated with paralytic ileus. An emergency laparoscopic appendectomy was performed. He was discharged on day 25 of hospitalisation after antibiotic therapy.
Discussion:
The present case suggests that the mechanism of hepatic portal venous gas was paralytic ileus, which caused gas-forming bacterial proliferation. The gas produced by bacteria and/or the gas-forming bacteria entered the bowel wall, which caused pneumatosis intestinalis. The bubbles in the intestinal wall floated in the portal system and were detected as hepatic portal venous gas. Perforated appendicitis and paralytic ileus seemed to be caused by a delayed diagnosis of appendicitis. The point-of-care ultrasound examination was useful for detecting hepatic portal venous gas and for helping establish the diagnosis of appendicitis.
Conclusion:
Hepatic portal venous gas is a rare finding associated with appendicitis in children. In addition, point-of-care ultrasound is useful for detecting hepatic portal venous gas in paediatric patients.
Keywords
Introduction
Hepatic portal venous gas (HPVG) is a rare condition characterised by the presence of gas in the portal vein and its branches, and it is associated with necrotising enterocolitis, bowel ischaemia, diverticulitis, gastric pathologies, inflammatory bowel disease and other conditions. 1 In children, it can be associated with other intestinal diseases, such as intestinal necrosis, volvulus, enteritis and food allergies.1,2 In adult patients, the presence of HPVG is associated with a high mortality rate of 56%–90%. 1 Although there are few data on children with HPVG, a single-centre retrospective study reported a mortality rate of 23% in children. 2
HPVG is diagnosed using abdominal radiography, computed tomography (CT), or ultrasound. Ultrasound detection of HPVG is favourable because it can be performed repeatedly and does not expose patients to radiation. Ultrasound findings indicative of HPVG include highly echogenic particles flowing within the portal vein or highly echogenic patches in the hepatic parenchyma due to accumulation of gas bubbles. We present herein our experience with a rare case of HPVG associated with appendicitis that was diagnosed using ultrasound.
Case report
A 5-year-old boy was admitted to our hospital with a fever, which persisted for 4 days, and decreased oral intake of food. He did not complain of any symptoms due to developmental retardation. Physical examination revealed the following: body temperature of 39.6°C, heart rate of 146 beats per minute, respiratory rate of 32 breaths per minute, systemic oxygen saturation of 92% and blood pressure of 104/63 mm Hg. No heart murmur was observed. Auscultation of respiratory sounds revealed wheezing in the right chest. Abdominal distention and guarding were not detected as signs of peritoneal irritation. Chest radiography showed a cardiothoracic ratio of 0.45 and bronchial wall thickening. Laboratory tests revealed white blood cell count of 13.2 × 109/L, haemoglobin concentration of 12.9 g/dL with haematocrit of 37.2%, platelet count of 241 × 109/L and C-reactive protein of 5.59 mg/dL. Nasopharyngeal swab reverse transcription polymerase chain reaction revealed parainfluenza virus type 3. He was diagnosed with bronchitis and asthma and treated with inhalational beta stimulants and intravenous administration of steroids.
On the second day of hospitalisation, the patient had bilious vomiting. Physical examination revealed abdominal distention and absent bowel sounds. Bedside ultrasonography was immediately performed by a paediatrician. Hyperechoic HPVG particles flowing in the portal vein and hyperechoic patches in the hepatic parenchyma were detected (Figure 1, shown in the video (Supplementary Online Resource)). We also found dilated loops in the bowel and ascites with deposits. The appendix was not detected because of an acoustic shadow caused by intestinal gas. The patient was diagnosed with ileus, which required an emergency surgery. He was transferred to a paediatric surgical centre. Contrast-enhanced abdominal CT revealed enlargement of the appendix with appendicolith, dilated bowel loop, pneumatosis intestinalis and ascites (Figure 2(a) and (b)). The patient was diagnosed with perforated appendicitis and paralytic ileus. An emergency laparoscopic appendectomy was performed. The wall of the appendix was thickened and its tip perforated (Supplementary Figure 1). There were no necrotic changes in the intestinal tract or volvulus. Escherichia coli, Streptococcus constellatus, Bacteroides fragilis, Prevotella nigrescens and Slackia exigua were detected in ascitic fluid cultures. Antibiotic therapy was administered postoperatively, and the patient was discharged after 25 days of hospitalisation.
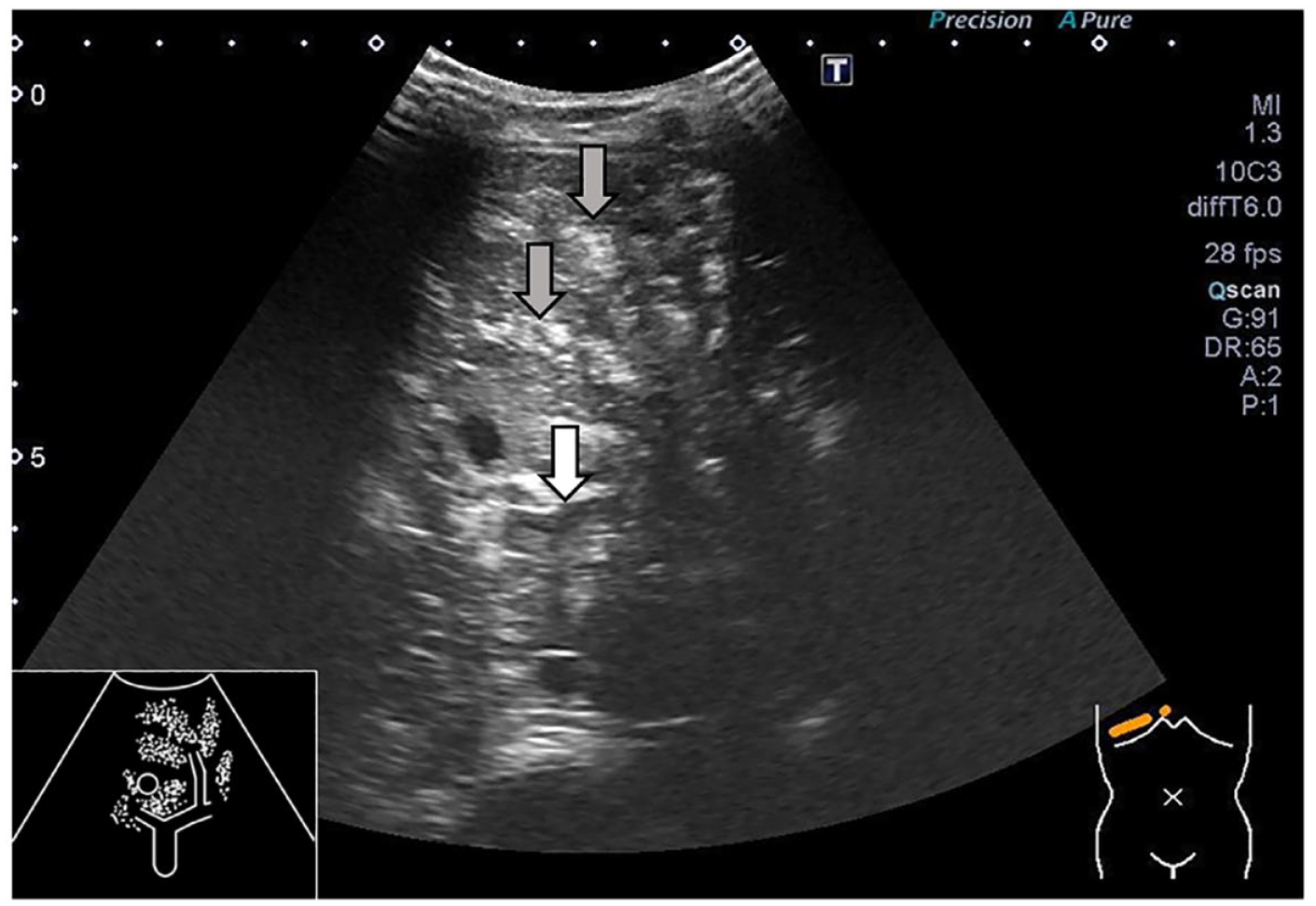
Ultrasound showing hyperechoic particles flowing in the portal vein (white arrow) and hyperechoic patches in the hepatic parenchyma (grey arrows).
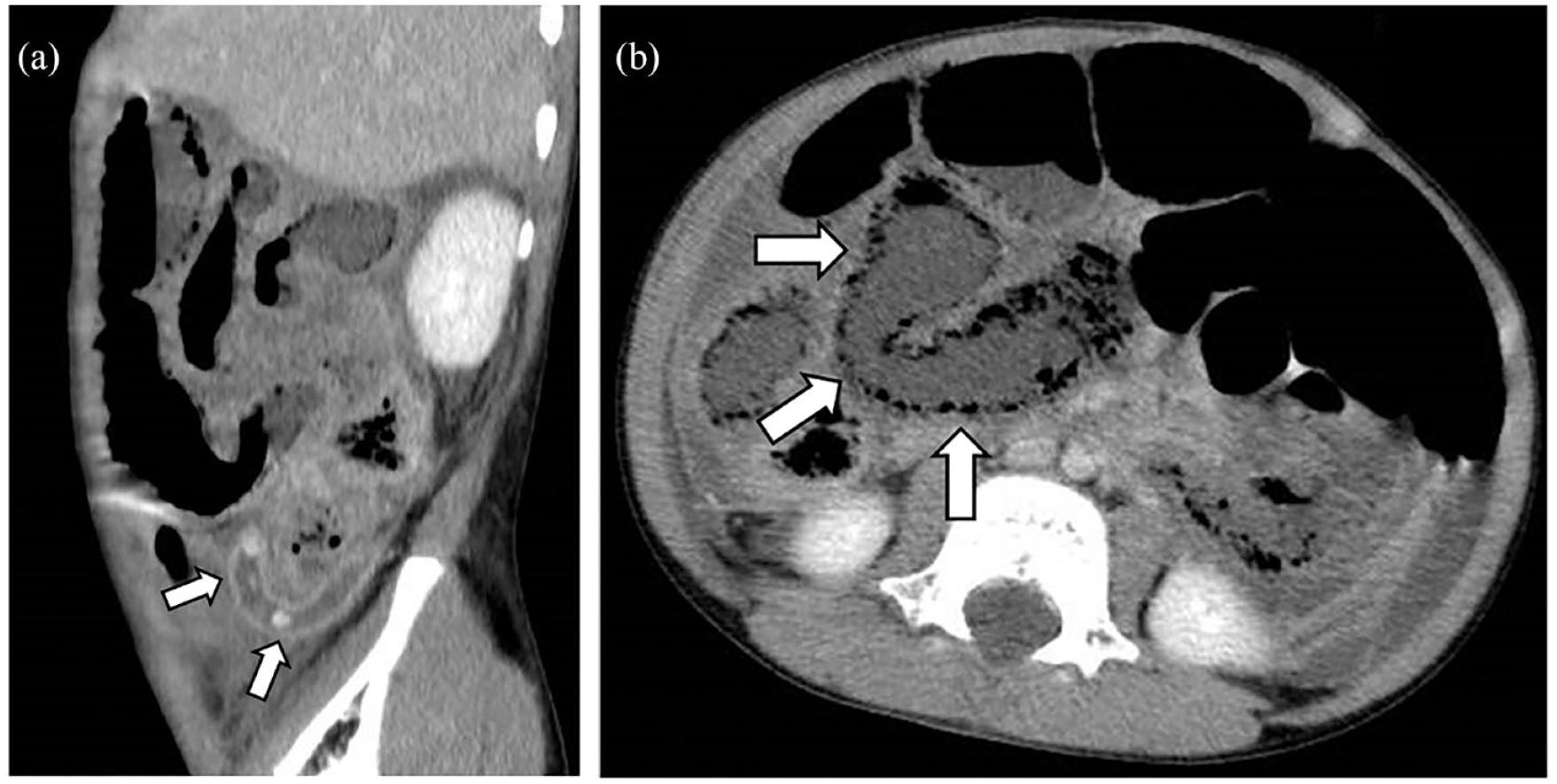
(a) Contrast-enhanced abdominal computed tomography (CT) showing enlargement of the appendix with appendicolith (white arrow). (b) Contrast-enhanced abdominal CT revealing pneumatosis intestinalis (white arrow).
Discussion
HPVG is an imaging finding suspected to be a severe intestinal disorder with poor prognosis. 1 The mechanism of HPVG is unclear; but gas-forming organisms are suspected to be involved. In this case, the pneumatosis intestinalis was also detected by contrast-enhanced abdominal CT. The mechanisms of HPVG and pneumatosis intestinalis overlap, in which mucosal disruption or increased mucosal permeability allows for the invasion of gas and bacteria into tissues. 3 Some hypotheses regarding the causes of pneumatosis intestinalis have suggested that (1) gas embolises into the bowel wall from either the intestinal lumen or the lungs and (2) gas-forming bacteria enter the submucosa and produces gas within the bowel wall. 4 The bubbles enter the venous system and float into the portal vein; these bubbles are detected as HPVG. In the present case, acute appendicitis with perforation caused paralytic ileus, which caused gas-forming bacterial proliferation. The gas produced in the intestinal tract entered into intestinal wall due to increasing intraluminal pressure; it was also possible that bacteria entered the intestinal wall and produced gas in the wall. The bubbles that entered or were produced in the bowel wall were detected as pneumatosis intestinalis by CT. Gas embolised into the bowel wall entered the mesenteric veins and floated into the portal vein, which was detected as HPVG using ultrasound.
Previously, four adult cases of HPVG associated with appendicitis have been reported (Table 1);5–8 approximately three-quarters of which were diagnosed as perforated appendicitis. In cases with intestinal necrosis or abscess, it tended to take more time to diagnose. Although most cases with HPVG were detected by CT, only one reported case was diagnosed by ultrasound. There is no report concerning a paediatric case of HPVG associated with appendicitis. In the present case, perforated appendicitis and bubbles floating in the portal vein seemed to be caused by a delayed diagnosis of appendicitis. The delayed diagnosis caused the paralytic ileus and pneumatosis intestinalis, which led to HPVG as a rare finding associated with appendicitis. The complex chronic conditions such as developmental retardation, which prevented the patient from complaining of any abdominal symptoms, are factors in the delayed diagnosis of acute appendicitis. 9 There were no findings suggestive of inflammatory bowel disease, immunoglobulin A vasculitis, or other immune system disorders. It was unclear at first that the patient’s airway symptoms were complicated by HPVG.
Cases of HPVG associated with appendicitis.
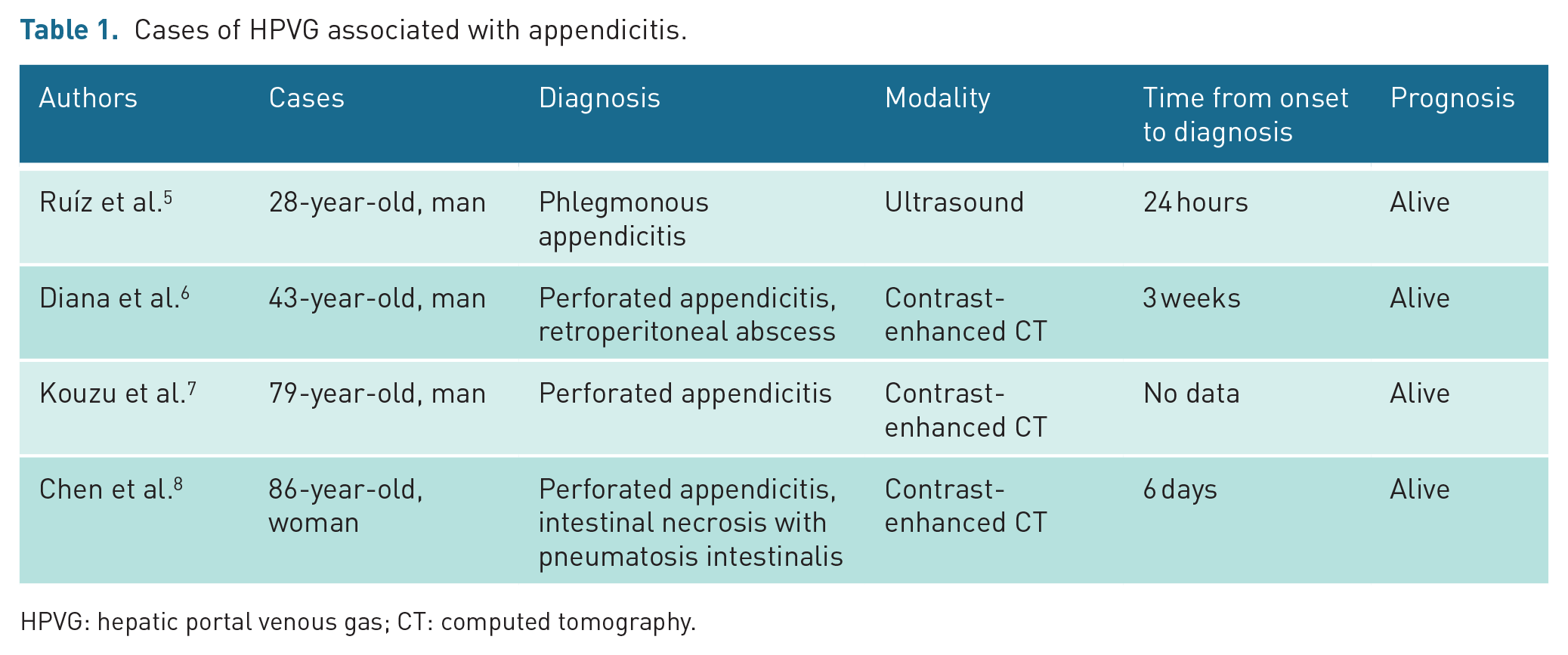
HPVG: hepatic portal venous gas; CT: computed tomography.
In addition, bedside point-of-care ultrasound (POCUS) was useful for detecting HPVG in this case. Ultrasound was performed immediately after the patient vomited, and HPVG was detected, which suggested a severe intestinal disorder. POCUS is defined as an ultrasound examination performed by a clinician in real-time. 10 Abdominal POCUS serves as an important diagnostic tool for various diseases, including abdominal trauma, appendicitis, ileus and pyloric stenosis. 10 Although ultrasound could not visualise the appendix due to an acoustic shadow associated with bowel gas in this case, the detection of HPVG using POCUS provided important information for managing this patient. Therefore, POCUS is beneficial for providing clinicians with real-time images of patients’ presenting signs, especially in children who cannot express their symptoms.
In conclusion, we present a rare case of HPVG associated with perforated appendicitis that could be caused by the delayed diagnosis of acute appendicitis and pneumatosis intestinalis. Furthermore, POCUS has been proven to be an effective diagnostic tool for detecting HPVG in paediatric patients.
Supplemental Material
sj-tif-1-ult-10.1177_1742271X231195752 – Supplemental material for Ultrasound and computed tomography findings of hepatic portal venous gas associated with acute appendicitis in a paediatric patient: A case report
Supplemental material, sj-tif-1-ult-10.1177_1742271X231195752 for Ultrasound and computed tomography findings of hepatic portal venous gas associated with acute appendicitis in a paediatric patient: A case report by Takashi Furuta, Mayu Fujiwara, Takahiro Motonaga, Hironori Matsufuji, Hiroshi Tateishi, Soichi Nakada, Tsutomu Kanagawa and Masashi Uchida in Ultrasound
Footnotes
Contributors
T.F. and H.T. were the principal investigators responsible for the manuscript. M.F., T.M. and H.M. helped with the clinical management. S.N. and T.K. performed laparoscopic appendectomy and postoperative management. The first draft of the manuscript was written by T.F. M.U. critically reviewed the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethics approval
This work does not involve any human/animal experimentation. The ethics approval was not required by the ethics committee of JCHO Tokuyama Central Hospital on 4 March 2022.
Guarantor
M.U. is the guarantor of this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.