
Abstract
Kawasaki disease (KD), a febrile vasculitis primarily affecting young children under 5, is commonly associated with coronary artery complications. This report describes the case of a 2.5-month-old infant presenting with a persistent 15-day fever, initially misidentified as pharyngitis and otitis media. Laboratory tests indicated significant leukocytosis, thrombocytosis, and increased C-reactive protein (CRP) levels. Echocardiography revealed coronary artery dilation and pericardial effusion, confirming a KD diagnosis. The infant received intravenous immunoglobulin (IVIG) and high-dose aspirin, which resolved the fever. Symptom recurrence necessitated additional IVIG and corticosteroid treatment. Subsequent imaging showed ongoing coronary dilation, emphasizing the risk of lasting vascular complications. This case underscores the diagnostic challenges of KD in infants, especially those with atypical presentations. Prompt diagnosis and treatment are critical to prevent serious complications such as coronary aneurysms. Healthcare providers should consider KD in infants with prolonged unexplained fevers to improve prognosis and minimize heart-related risks.
Introduction
Kawasaki disease (KD) was first recognized by Nagasaki Fuzuo in 1967. 1 This acute systemic vasculitis predominantly affects children aged 6 months to 5 years, with coronary artery abnormalities representing its most critical complication.1,2 Epidemiological studies indicate a male predominance, with diagnosis rates 1.5 to 2 times higher in males compared to females. 3 While KD incidence is highest in east Asian populations—especially Japan and South Korea—cases are increasingly reported in non-Asian regions.4,5
Classic clinical features include prolonged fever, cervical lymphadenopathy, bilateral conjunctival injection, erythema of the lips and oral mucosa, a “strawberry” tongue, and erythema/edema of the extremities. Atypical presentations often complicate diagnosis and management, particularly in infants under 6 months who exhibit incomplete symptoms and face elevated cardiac risks. 6 Untreated cases progress to severe cardiovascular sequelae in 20% to 25% of patients, positioning KD as the foremost cause of acquired pediatric heart disease in developed nations.
Diagnosis relies on clinical criteria, inflammatory markers (eg, leukocytosis, thrombocytosis), and echocardiographic evidence of coronary artery changes. Standard therapy combines intravenous immunoglobulin (IVIG; 2 g/kg) and high-dose aspirin, initiated promptly to reduce inflammation and prevent coronary aneurysms. 6
This report describes a rare instance of KD in an exceptionally young patient, underscoring the diagnostic complexities in atypical age groups. Early intervention remains vital to minimizing cardiac morbidity.
Case Presentation
A 2.5-month-old baby experienced persistent fever for 15 days, peaking at 39°C and responding to oral antipyretics, but without other symptoms. Initially diagnosed with pharyngitis and otitis media, the fever continued, accompanied by vomiting and cracked lips. The baby was then referred to a hospital for further evaluation and lab tests shown in (Table 1).
Laboratory Results at Admission (Day 20 of Illness).
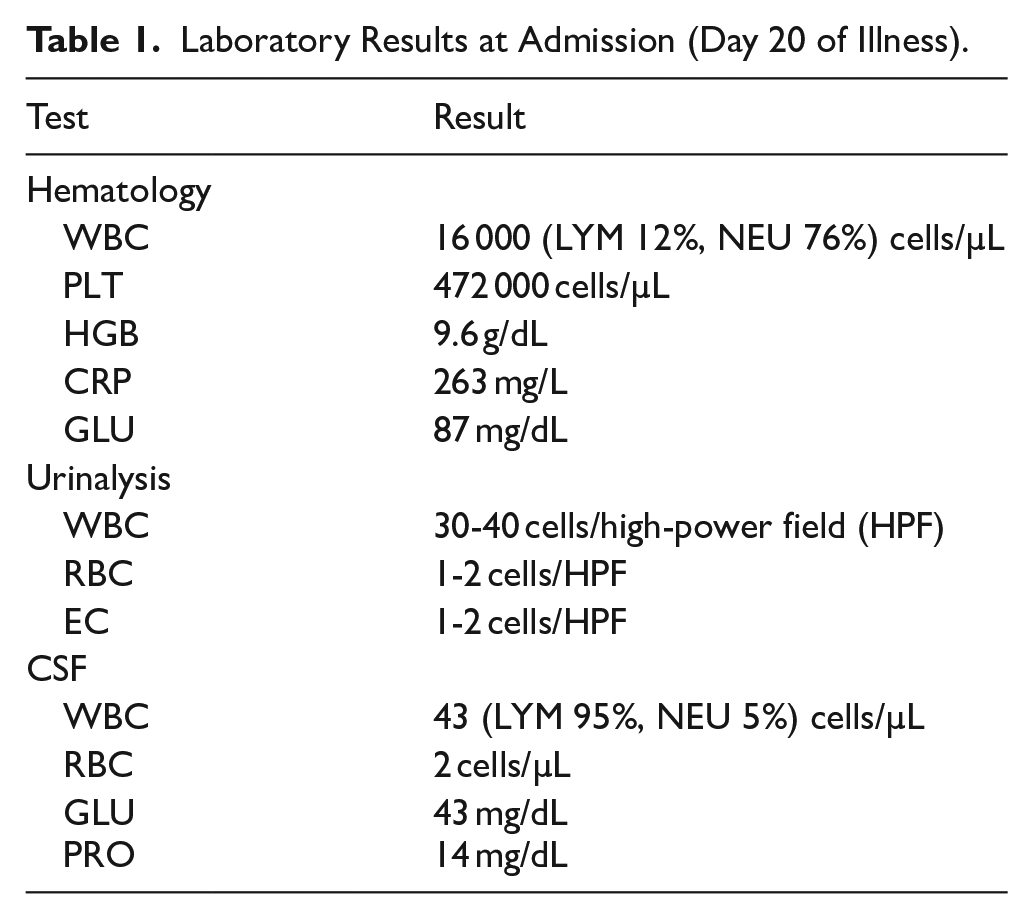
Based on the clinical findings and the presence of white blood cells in the urinalysis, the case was initially handled as meningitis paired with urinary tract infection (UTI), but treatment for the UTI was insufficient. The patient was given a 14-day antibiotic regimen that included ceftriaxone, vancomycin, and amikacin. However, the fever continued, peaking every 6 hours at a maximum of 38.5°C. Laboratory results were subsequently reexamined and shown in Table 2.
Laboratory Results After 48 Hours of IVIG Treatment (Day 22 of Illness).

The patient was transferred to pediatric hospital for further evaluation. Upon admission, the patient presented with a temperature of 38.2°C, respiratory rate of 44 breaths/min, heart rate of 160 bpm, blood pressure of 75/55 mmHg, and oxygen saturation of 98% without supplemental oxygen. He was fully conscious, with a Pediatric Glasgow Coma Scale score of 15/15. Peripheral pulses were palpable and well-filled, with a capillary refill time of 3 seconds. Notable findings included skin peeling on the fingers and toes, accompanied by nail peeling. Oral and pharyngeal examination was normal, with no enlarged lymph nodes or visceral enlargements. Chest examination was also normal. Heart examination revealed a rapid heart rate with intensified heart sounds. Neurological examination showed cervical lordosis and intensified tendon reflexes in all limbs. He was then admitted to the infectious disease department. Several differential diagnoses were considered, including meningitis, urinary tract infections, brucellosis, and KD. Additional lab tests were conducted after admission, and the results are presented in Table 3.
Laboratory Results at Hospital Discharge (Day 25 of Illness).

Radiological scanning revealed normal abdominal echography results. The chest X-ray (CXR) showed enlargement of the heart shadow. A head CT scan indicated signs of slight frontal cerebral atrophy, with subarachnoid space expansion and sylvian fissure expansion. The echocardiogram demonstrated moderately pericardial effusion and right coronary expansion measuring 2.6 mm at the origin. Additionally, it identified cystic conformations with clear content at the expense of the right atrium in the auriculo-ventricular groove, which may represent aneurysms (Figure 1).

Echocardiogram showing the aneurysm in the right coronary artery, 2 different sections.
A comprehensive clinical assessment uncovered ongoing hyperthermia that persisted for over 15 days, along with significant skin peeling on the fingers and toes. Laboratory analyses showed increased WBC and PLT counts. Furthermore, an echocardiogram revealed moderate pericardial effusion and a dilation of the right coronary artery measuring 2.6 mm at its origin. These results lead to a diagnosis of KD.
Consequently, treatment for KD was promptly initiated, which included an infusion of IVIG at a dose of 2 g/kg and aspirin at a dose of 100 mg/kg. The patient also received enoxaparin sodium at a dose of 100 units/kg every 12 hours.
After treatment we observed the patient and noticed that for 2 days the fever was absent. A subsequent echocardiogram revealed enlargement of the atriums and slight pericardial effusion, especially at the heart’s apex. Three cystic formations, possibly megaloaneurysms, were found in the right auriculo-ventricular groove, with densities suggesting thrombosis. The MB-CK test showed 17.8 U/L, and an MSCT with contrast was ordered. The fever returned 48 hours after the IVIG infusion. MSCT results indicated a tortuous vascular structure up to 10 mm in diameter, likely an aneurysm in the right coronary artery (Figures 2 and 3).

Sections of MSCT showing the aneurysms of the right coronary artery.

Digital recreation of the aneurysm of the right coronary artery.
A second IVIG dose, methylprednisolone 30 mg/kg/24 h, and aspirin 50 mg/kg/24 h were administered. After a few days, the fever subsided, and lab evaluations were repeated. The echocardiogram showed persistent right coronary dilatation with a zigzag mass, left coronary dilatation, and mild mitral insufficiency. Oral prednisolone, aspirin, and warfarin were prescribed. Lab tests were re-evaluated before discharge, with recommendations for cardiac follow-up and neurological consultation. Brain MRI indicated meningoencephalitis, atrophic changes, and cervical The MRI revealed fused vertebrae along with other normal results.
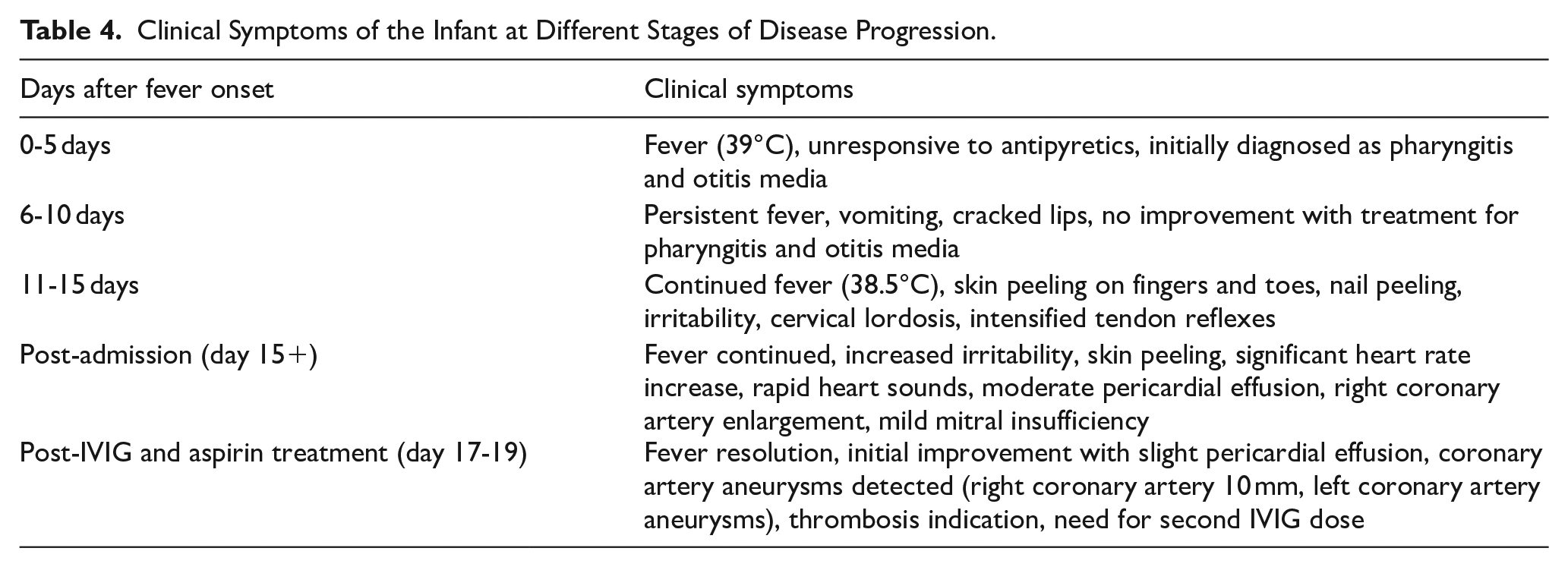
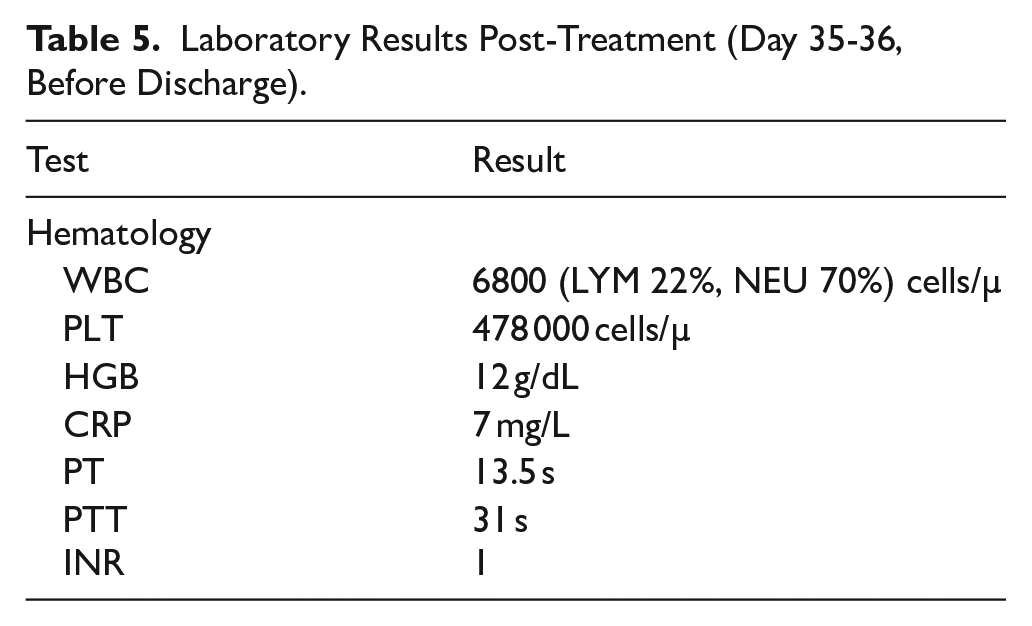
Neurological recommendations included physical therapy. A follow-up echocardiogram a week after discharge showed a large right coronary artery aneurysm, with the same measurements as before, without thrombosis, and a left coronary artery aneurysm without thrombosis. Table 4 shows the clinical symptoms of the infant at different stages of disease progression (Table 5).
Clinical Symptoms of the Infant at Different Stages of Disease Progression.
Laboratory Results Post-Treatment (Day 35-36, Before Discharge).
Discussion
Kawasaki disease (KD) was first recognized as a condition that predominantly affects children under the age of 5. It poses considerable risks to the coronary arteries and is more common in males.
It is notably higher in Asian nations like Japan and South Korea, though it occurs globally.
A comprehensive review conducted between 1978 and 2023 across 16 countries in the Arab world identified a total of 1264 reported cases of Kawasaki disease (KD). Of these, 256 cases involved coronary artery aneurysms (CAA), including 25 classified as giant coronary aneurysms. 7 Notably, there have been no officially recorded cases of Kawasaki disease in Syria to date, indicating a significant gap in national epidemiological reporting.
The cause of KD remains unclear, but some studies indicate it may be linked to infections due to its clustering patterns and low recurrence rates, while others propose a connection to neonatal sepsis and pneumonia. Commonly suspected pathogens include Staphylococcus aureus, Streptococcus pyogenes, and certain respiratory viruses like adenovirus and coronavirus, though no single pathogen has been definitively proven as the cause. 8 Other theories propose a connection to neonatal sepsis and pneumonia. 8
KD is a feverish condition in children characterized by symptoms such as conjunctival injection, oral changes, rash, alterations in extremities, and cervical lymphadenopathy, with recent guidelines indicating that fever is not essential for diagnosis; newborns are more likely to show incomplete symptoms compared to older children. 8 The primary symptoms of incomplete Kawasaki disease (IKD) include fever, redness, and swelling in the limbs.4,8 In our case the infant did not present with sepsis or pneumonia, but he experienced persistent fever for 15 days, peaking at 39°C and responding to oral antipyretics. After a doctor’s visit for pharyngitis and otitis media, vomiting and cracked lips emerged while the fever continued.
A prior investigation analyzed neonatal Kawasaki Disease (KD) cases that conformed to diagnostic criteria from the 6th revised edition of clinical guidelines. Researchers excluded duplicate cases or those with insufficient clinical, laboratory, or outcome data. After screening 15 published studies, 19 cases were included in the review. Of these, Incomplete Kawasaki Disease (IKD) constituted 68% (13/19). The most frequently reported clinical manifestations were rash (94.7%, 18/19), extremity changes (78.9%, 15/19), fever (78.9%, 15/19), and erythema of the lips/oral mucosa (68.4%, 13/19). Less common findings included bilateral non-purulent conjunctivitis (42.1%, 8/19) and cervical lymphadenitis (10.5%, 2/19). Notably, coronary artery lesions were identified in 89.5% (17/19) of patients. Laboratory analyses revealed elevated C-reactive protein (CRP) levels in 63.2% (12/19) of cases and platelet counts above 300 × 10⁹/L in 57.9% (11/19). 9
In contrast, the present case lacked hallmark features such as rash, lip/oral mucosa erythema, conjunctivitis, or cervical lymphadenopathy.
A significant proportion of KD cases affect infants younger than 6 months, representing approximately 10% of all cases. These infants are less likely to display typical symptoms and show a higher incidence of incomplete or atypical KD presentations, affecting 40% of infants versus 10% to 12% in older children. In this age group, persistent fever and extreme irritability may be the sole indicators of the disease. Fever accompanied by pyuria in infants is frequently mistaken for a urinary tract infection (UTI). Due to the nonspecific nature of these symptoms, diagnosis and treatment are often delayed, resulting in delayed recognition and elevated risks of coronary artery abnormalities, aneurysms, and life-threatening complications such as giant coronary aneurysms, shock, or fatal outcomes. Infants in this age group face the highest rates of severe complications and mortality among KD patients. 10
In our case, the infant presented with fever and considerable irritability, along with indications of large coronary artery aneurysms and shock; however, we successfully managed the situation.
A giant coronary aneurysm is characterized by a Z-score of 10 or greater, or a diameter exceeding 8 mm in the pediatric population, or a diameter that surpasses the reference vessel diameter by more than 4 times in adults. The development of coronary artery aneurysms is thought to involve mechanisms such as breakdown of the medial arterial layer, weakening of the vessel wall, heightened mechanical stress, and progressive coronary segment dilation linked to elevated matrix metalloproteinase activity. Contributing factors range from Kawasaki disease (KD) and atherosclerosis to vasculitis, infections, congenital coronary anomalies, and connective tissue disorders. Among KD patients, coronary aneurysms occur in roughly 0.3% to 0.8% of cases, with aneurysm size strongly predicting clinical outcomes. Smaller aneurysms (<8 mm or Z-score < 10) may resolve naturally without complications like persistent vascular remodeling. In contrast, giant aneurysms (>8 mm or Z-score ⩾ 10) seldom regress and are associated with higher risks of thrombosis, stenosis, or myocardial infarction.11 -13
The MSCT findings of the patient revealed a twisted vascular formation with a diameter of up to 10 mm, which is probably an aneurysm in the right coronary artery.
Numerous treatment strategies exist for managing IKD, but a unified approach has not been reached. The backbone treatment consists of IVIG and aspirin. Additional therapies may involve corticosteroids and biologic medications. 6
And that’s what we used for treatment in our patient.
Compared to typical cases of KD described in medical literature, this case is notable for the patient’s exceptionally young age (2.5 months), the remarkably large coronary aneurysms (10 mm), atypical clinical presentation, and an initial misdiagnosis as pharyngitis and otitis media. Furthermore, the early onset, absence of coronary ostium involvement, lack of aortic calcification, and absence of infection markers strongly suggested KD as the most probable diagnosis.
Conclusion
This case highlights the challenges of diagnosing KD in very young infants, particularly when classic symptoms are absent. The patient initially presented with prolonged fever and irritability, leading to a misdiagnosis. However, the detection of large coronary aneurysms (10 mm) confirmed KD.
Given the increased risk of severe cardiac complications in infants, early recognition is crucial. This case emphasizes the need for heightened clinical suspicion and timely treatment to improve outcomes in atypical KD presentations.
Footnotes
Acknowledgements
We would like to thank Dr. Yahia Ranjous for his help in checking our academic writing and reviewing some points.
Ethical Considerations
Ethical approval is not required for case reports at our institution.
Consent to Participate
Written informed consent was obtained from the parents for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author Contributions
Suzan Mahfoud: Supervised the clinical and research components of the study, provided direct patient care, conducted critical revisions of the manuscript, and approved the final version. Aous Arous: Participated in data acquisition, performed data analysis and interpretation, curated resources, validated findings, designed visualizations, drafted the manuscript, contributed to revisions, and approved the final submission. Danial Antonios: Engaged in data collection, analyzed and interpreted results, provided resources, verified data accuracy, developed visual materials, authored sections of the manuscript, revised content critically, and endorsed the final draft. Hussein Jasser: Led project coordination and study design, facilitated data collection, conducted analytical interpretation, managed resources, ensured data validation, created visual representations, wrote portions of the manuscript, performed critical editing, and approved the final version. Abdulrahman Shbani: Contributed to data analysis and interpretation, supported resource acquisition, validated outcomes, assisted in visualization, drafted manuscript content, participated in revisions, and approved the finalized document.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.