
Abstract
Kawasaki disease is an acute multisystemic vasculitis occurring predominantly in children and rarely in adults, with sequelae of potentially life-threatening coronary artery aneurysms. “Incomplete” Kawasaki disease is a novel concept and considered a diagnosis of exclusion as it alludes to patients with fever lasting ⩾5 days and 2 or 3 clinical criteria without another reasonable explanation for the illness. The multidisciplinary team should be vigilant for this oligosymptomatic clinical presentation, specifically within this subgroup despite age and ethnicity, and the syndrome should be considered as a differential diagnosis in challenging cases presenting as infectious or autoimmune disease.
Introduction
Kawasaki disease (KD) is an acute multisystemic vasculitis occurring predominantly in children and rarely in adults with sequelae of potentially life-threatening coronary artery aneurysms (CAAs).1,2 The precise etiology is yet to be ascertained; however, epidemiologic studies have implicated infectious agents with both autoimmune and genetic mechanisms being postulated as well. 3 The pathophysiology involves a complex inflammatory milieu with a predilection for small- to medium-sized arteries, especially the coronary vessels.4,5
It is estimated that there are approximately 10 000 incident cases per year in Japan alone and 4000 in the United States.6,7 The epidemiology and characteristics of this enigmatic syndrome are virtually unknown in the largely heterogeneous Caribbean population; however, it remains the leading cause of acquired heart disease in the developed world. The most devastating complication is that of CAA, but also include other organ systems. 8
The diagnosis is usually clinched via guidelines as there is no specific, confirmatory test available. “Incomplete” KD is a novel concept and considered a diagnosis of exclusion as it alludes to patients with fever lasting ⩾5 days and 2 or 3 clinical criteria without another reasonable explanation for the illness. 2 The term “atypical” KD should be reserved for patients who display symptoms that are not common in classical KD, such as renal impairment, acute surgical abdomen, and pleural effusion. 8
We describe a first case report of an adult South Asian patient with incomplete features of KD, which can masquerade as a clinical distractor.
Case Report
A 29-year-old South Asian male with no significant medical history presented to the emergency department with a 14-day symptom complex of persistent, high-grade fever refractory to antibiotics and antipyretics, malaise, and anorexia with a 10-pound weight loss. There were no recent medications, ill contacts, or travel history. His vital signs affirmed normotensive blood pressures, a resting sinus tachycardia of 110 beats per minute, and pulse oximetry of 98% on room air with a mild pyrexia of 38.8°C. Physical examination revealed bilateral conjunctivitis with chemosis, a strawberry tongue glossitis, palmar desquamation, and ichthyosis (see Figure 1a-c, respectively). There was no evidence of lymphadenopathy or dermatologic manifestations, such as rash.
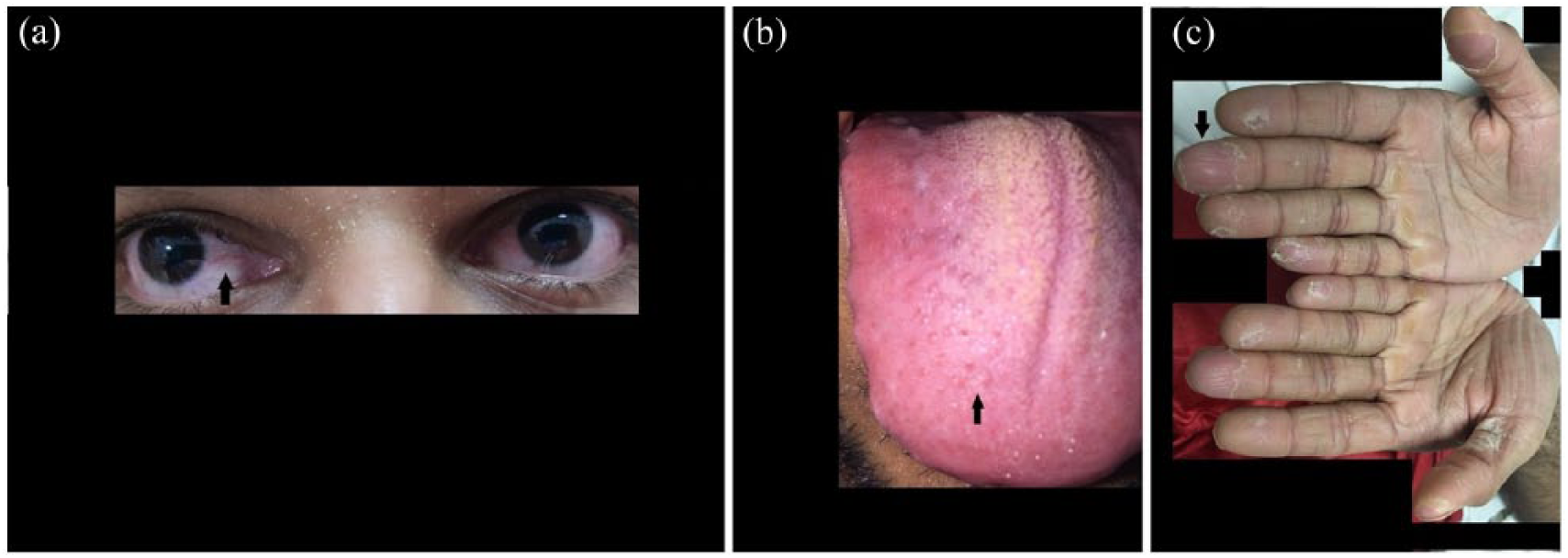
(a) The patient’s bilateral keratoconjunctivitis with chemosis, indicated by the black arrow. (b) The patient’s strawberry tongue glossitis with hyperplastic fungiform papillae, indicated by the black arrow. (c) The patient’s palmar desquamation with incomplete dehiscence of the epidermis and associated ichthyosis, indicated by the black arrow.
Recent pertinent laboratory investigations (see Table 1) included a leukocytosis and notable thrombocytosis, normal comprehensive metabolic panel, markedly elevated inflammatory markers of erythrocyte sedimentation rate, and C-reactive protein. An extensive infectious disease diagnostic workup indicated negative blood, urine, and stool cultures and normal tests for human immunodeficiency virus, mycobacterium tuberculosis, hepatitis B and C, influenza A and B, adenovirus, echovirus, coxsackie virus, dengue, malaria, leptospirosis, mycoplasma, legionella, Epstein-Barr virus, cytomegalovirus, and Clostridium difficile toxin. An in-depth immunological panel revealed no evidence of vasculitides or rheumatological disease, such as systemic lupus erythematosus, rheumatoid arthritis, Sjogren’s syndrome, polyarteritis nodosa, the polyangiitis spectrum, and cryoglobulinemia. A potential adverse drug reaction was not entertained as the patient was not administered any recent therapeutic or complementary alternative agents. Cardiovascular testing with both an electrocardiogram and echocardiogram were normal and advanced imaging with a pan-body computed tomography scan was also unremarkable. He was deemed to have an incomplete presentation of KD and was initiated on high-dose enteric-coated aspirin (Bayer HealthCare Pharmaceuticals LLC, Berlin, Germany) 325 mg every 8 hours, as well as single infusion of intravenous immunoglobulin (GammaGard, Baxter International Inc, Glenview, IL) at a dose of 2 g/kg over a 12-hour period. Subsequently, his clinical syndrome gradually resolved over the ensuring hospitalization as his pyrexia de-effervesced along with steady improvement of his inflammatory markers. He did not receive any glucocorticoids or immunomodulating therapies. He was safely discharged after 1 week of inpatient care on low-dose aspirin monotherapy with gastroprotective proton-pump inhibitors and subsequently scheduled for a dedicated cardiac computed tomography angiogram that did not reveal any CAAs at a later outpatient clinic appointment (2 weeks from index hospitalization).
Comprehensive Laboratory Testing Including the Infectious and Immunologic Panels.

Discussion
The diagnosis of classic KD is usually verified via guidelines as there is no specific, confirmatory test available (Table 2).8-10 Adult incomplete KD was clinically diagnosed based on the absence of overt infection, persistence, and recrudescence of high-grade fever despite empirical antibiotics and antipyretics, and the presence of conjunctivitis, glossitis, and palmar desquamation.9,11 A recent French study evaluated 9 patients who fulfilled criteria for incomplete disease. The median time to diagnosis was 13 days, which coincided with our patient’s time to presentation and the main symptoms were fever (100%), exanthema (98%), changes in the extremities (91%), conjunctivitis (77%), oral cavity changes (89%), cervical adenitis (55%), and cardiac abnormalities (45%) of which fever, changes in the extremities, conjunctivitis, and oral cavity changes featured as clinical signs in our patient. Overall, 35% of the patients showed large-vessel vasculitis: coronary vasculitis (26%) and coronary aneurysm (19%), neither of which were replicated in our patient.11,12 Another large, international-based registry of non–East Asian incomplete KD patients reported statistically significant increases in the occurrence of conjunctivitis, mucosal changes, and extremity alteration, which paralleled our observations. 12

To our knowledge, this is the first reported case of an adult South Asian male in the Caribbean presenting with incomplete KD. Apart from his age, our patient was also of South Asian ethnicity; and currently, there exists a paucity of literature with regard to this subgroup. In many developing countries, including India, the majority of patients with KD continue to remain undiagnosed likely attributed to lack of awareness among clinicians. 13 Adult-onset KD should be considered as a differential diagnosis in challenging cases presenting as infectious or autoimmune disease even if the patient is not of East Asian lineage.13-15
The key therapeutic strategy for KD is to prevent the formation of CAAs and symptom alleviation. Inpatient supportive management and administration of intravenous immunoglobulin (IVIG) is considered to be the mainstay of treatment.16-18 Currently, there are several risk scores for IVIG resistance that could identify patients at high-risk for nonresponse to IVIG treatment, which in turn is highly associated with the development of CAAs.19-21
American Heart Association (AHA) guidelines recommend a second dose of IVIG, methylprednisolone, a longer tapering course of prednisolone or prednisone plus IVIG, cyclosporine, immunomodulatory monoclonal antibody therapy, cytotoxic agents, or plasma exchange for patients resistant to IVIG.10,18,22
Aspirin has been the conventional, standard therapy for its antiplatelet effects, initially a high-dose regimen for a variable period, followed by a lower dose for a protracted period in patients with small CAAs, whereas dipyridamole is indicated in patients with larger CAAs. 23 It is recommended by the AHA guidelines that these patients should be treated with low-dose aspirin until aneurysms are documented to have regressed. Clopidogrel has also been used in cases of aspirin hypersensitivity. 4
As of 2017, the AHA and the Japanese Circulation Society guidelines specify that KD patients require vigilant follow-up with noninvasive imaging and cardiac stress testing and to detect progressive stenosis, thrombosis, and luminal occlusion that may lead to myocardial ischemia and infarction.10,24,25
The literature is not replete with describing this subpopulation of incomplete KD with regard to age and ethnicity and this case emphasizes its rarity, but also underscores the absolute necessity for specific guidelines in this patient panel. 2
Conclusion
In summary, we describe the first case report of incomplete KD in an adult South Asian patient based in the Caribbean. The multidisciplinary team should be vigilant for this oligosymptomatic clinical presentation, specifically within this subpopulation despite age and ethnicity, and the syndrome should be considered as a differential diagnosis in challenging cases presenting as infectious or autoimmune disease.
Footnotes
Author Contributions
NB, RS, SV, NM, VM, SG, and NAS all contributed equally in writing the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
The patient provided written informed consent to have the details of his case published.