
Abstract
Background:
Spontaneous Retropharyngeal Hematoma and cervical hematoma are rare conditions characterized by the accumulation of blood in the retropharyngeal and cervical region and poses a potential life-threatening risk. This complication can occur unexpectedly and without apparent trauma, particularly in patients on vitamin K antagonists.
Case Presentation:
A 60-year-old man presented to the emergency with acute dysphagia, dysphonia and a right-sided neck ecchymosis. The patient had been on vitamin K antagonists for 7 years following a left intraventricular thrombus. Blood tests revealed an International Normalized Ratio of 7. The diagnosis of Spontaneous Retropharyngeal Hematoma was suspected given the absence of an identified cause and was confirmed by contrast-enhanced computed tomography. The hematoma was attributed to the patient’s long-term use of vitamin K antagonists, which predisposed him to spontaneous bleeding. Treatment involved the administration of vitamin K but the patient ultimately passed as a result of respiratory arrest.
Conclusion:
Spontaneous Retropharyngeal Hematoma due to VKA-related incidents is a rare but significant complication to consider in patients undergoing anticoagulant therapy. Awareness among healthcare professionals is crucial to ensure early recognition and appropriate management.
Introduction
Vitamin K antagonist (VKA) is by far the most widespread oral anticoagulant used in underdeveloped and emerging countries. Its efficacy in prevention of thrombotic and embolic events has been demonstrated in numerous studies. 1 The occurrence of bleeding on VKAs, whether in the therapeutic zone or in overdose, is an event with far-reaching consequences, and its frequency is not negligible. 2
In the neck, the organization of fascial planes, bordering potentially expansive and interconnected spaces, facilitates the emergence of significant space-occupying lesions. 3 Retropharyngeal hematoma (RH) is a rare and potentially fatal condition due to its rapid compressive impact on the upper respiratory airways. 4
We describe a rare case of spontaneous retropharyngeal hematoma (SRH) and cervical hematoma (CH), an unusual localization of a hemorrhagic event with antivitamins K. We discuss the pathology, diagnostic challenges, and therapeutic issues associated with this unusual case.
Case Presentation
A 60-year-old man was referred to our emergency department with acute difficulty of swallowing and dysphonia. The symptoms began a week before presentation along with sore throat, for which his family physician prescribed Augmentin, 1 g twice daily, and analgesics. The patient had a history of hypertension treated by amlodipine, diabetes treated by oral antidiabetic drugs, ischemia of the left lower limb stented in 2012 and a left intraventricular thrombus managed with a daily dose of 1/4 tablet of Sintrom for the past 7 years. No history of alcohol or tobacco intoxication was recorded.
Physical examination revealed an alert, oriented patient with a Glasgow Coma Scale of 15/15. On the hemodynamic aspect, the patient had a blood pressure of 136/70 mm Hg and a pulse of 92 beats/min. On the respiratory side, the patient was tachypneic with a respiratory frequency of 25 breaths/min; and an oxygen saturation of 97% on room air. The chest auscultation was normal. Examination of the oral cavity revealed a large, soft, violaceous mass involving the soft palate, uvula and right lateral and posterior wall of the pharynx (Figure 1A). Neck examination showed a right-sided ecchymosis with a pain at flexion and extension (Figure 1B). Anterior rhinoscopy was normal. The remainder of the general examination showed no abnormalities.
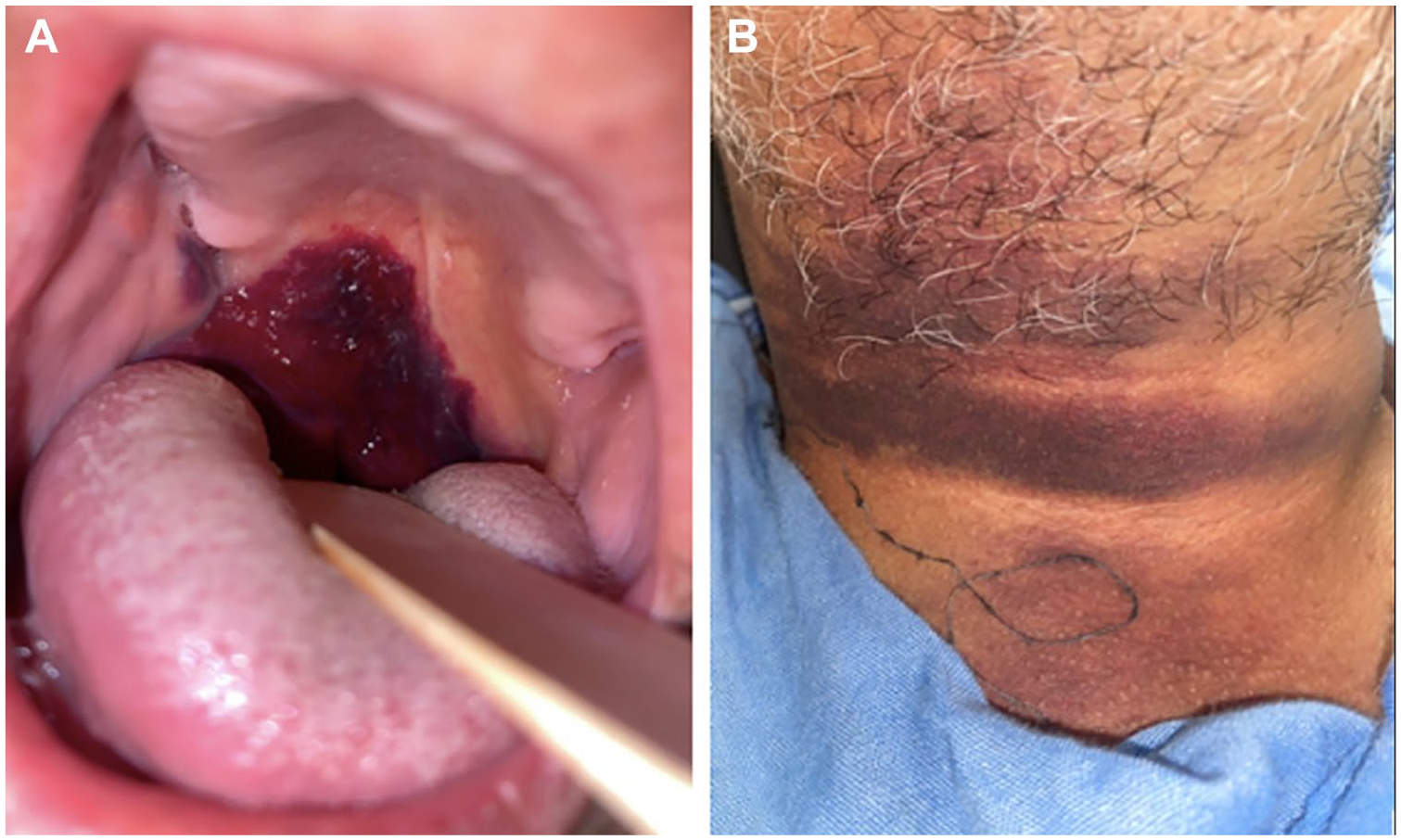
(A) Hematoma of the uvula, soft palate and the postero-lateral wall of the oropharynx. (B) Rightsided cervical ecchymosis.
The admission blood tests revealed a prothrombin time inferior to 10% with an International Normalized Ratio (INR) superior to 7 (normal range 0.8-1.2, therapeutic range 2.0-3.0). The electrolyte panel revealed no abnormalities, and the complete blood count demonstrated a hemoglobin of 16,2 g/dl, a hematocrit of 32%, a platelet count of 290 000/mm3 and a white blood cell count of 9960/mm3.
The contrast-enhanced (CT) scan of the neck revealed a well-defined hematoma, appearing as a non-enhancing mass located in the right posterolateral wall of the oropharynx, with extension into the hypopharynx and supraglottic region, measuring 37 mm in height (Figure 2). In addition, a linear area of contrast extravasation was noted (Figure 2B), consistent with active arterial bleeding at the time of imaging.

Contrast-enhanced CT of the neck in coronal (A) and axial (B) planes revealing huge hematoma of the right postero-lateral wall of the oropharynx extending to the hypopharynx, the supraglottic region and the homolateral vocal cord (white arrows). In addition, a linear area of contrast extravasation was noted, consistent with active arterial bleeding ((B) yellow arrows).
Other potential causes of retropharyngeal hematoma, such as trauma, infection, foreign body ingestion, or vascular anomalies, were systematically excluded based on the patient’s history, physical examination, and imaging findings. Given the absence of these factors and the patient’s elevated INR of 7 due to long-term use of vitamin K antagonists, the hematoma was classified as spontaneous, directly related to anticoagulation therapy.
The initial treatment involved admission to the intensive care unit and the intravenous administration of 10 mg of vitamin K, with the discontinuation of Sintrom as part of the management of VKA-related incidents. The progression was characterized by the normalization of biological markers, with a control INR at 30 minutes of 1.33 and a PT of 60%. However, the patient progressed to complete airway obstruction and respiratory arrest. An emergency tracheotomy was performed and the patient was put on mechanical ventilation. Unfortunately, the evolution was marked by abolition of brain stem reflexes and bilateral mydriasis. The electroencephalogram (EEG) confirmed brain death, and the patient succumbed on the third day of hospitalization.
Discussion
The retropharyngeal space is a median anatomical region situated between the posterior wall of the pharynx and the vertebral column, covered by the prevertebral muscles and the prevertebral fascia. It spans from the basilar part of the occipital bone to the sternal notch in the mediastinum. The alar fascia divides the retropharyngeal space into 2 components; the “true” retropharyngeal space and the “danger space.” 5 The continuity of the danger space with the mediastinum facilitates the dissemination of collections from the oral cavity to the thoracic cavity, posing potential life-threatening complications given the risk of developing mediastinitis and airway obstruction.
RH is a rare condition with the potential for a fatal outcome due to progressive internal bleeding and airway obstruction. Diagnosis can be challenging, as patients may initially present only with a sore throat, leading to potential misdiagnosis as viral pharyngitis. Many potential causes of RH were documented. 6 Neck trauma is undoubtedly the primary contributor, 7 followed by hemorrhagic diathesis6,8 and anticoagulation related incidents.6,9 Other possible causes include neck infections, foreign body, parathyroid adenoma or cyst, aneurysm rupture, jugular vein canulation, and after vomiting, sneezing or coughing. In cases where no evident cause can be identified, the diagnosis of SRH is established. 6 In this case, the RH was classified as spontaneous due to its association with anticoagulation therapy and the absence of trauma or other identifiable causes. Spontaneous hematomas in patients on VKAs occur without any external precipitating factors, as the altered coagulation status predisposes them to bleeding. This underscores the importance of considering spontaneous bleeding as a potential complication in patients undergoing anticoagulant therapy, even in the absence of obvious triggers.
While plain X-ray evaluation remains the most easy and accessible method for exploring the RPS, 10 CT stands out as a superior tool due to its ability to provide the anatomical variations and the extension of the RH in short time. 6 However, the CT image is not always specific of RH and may not significantly contribute to the differential diagnosis. Magnetic resonance imaging (MRI) offers several advantages over CT in terms of multiplanar anatomic display and superior soft-tissue contrast. 11 It is sensitive to blood products in different stages of evolution, allowing an early diagnosis of hematoma, with hyperintensity seen on both T1- and T2-weighted sequences within a few hours of the acute event.11,12 Nevertheless, MRI may not be suitable for agitated patients and may be unavailable in certain structures, especially in emerging countries.
The management of RH remains on 3 essential aspects; (1) correction of the abnormal hemostatic mechanism if present; (2) ensuring airway patency by tracheotomy, if necessary; and (3) evacuation of the hematoma when spontaneous resolution does not occur. 13 In our case, a VKA-related incident was the responsible mechanism of the RH. Given the potentially life-threatening nature of this incident, discontinuation of VKA with urgent INR measurement must be carried out, combined with the administration of both prothrombin complex concentrates (PPC) and 10 mg vitamin K. 14 INR levels should be checked at 30 minutes and at 6 hours. In this patient’s case, only vitamin K was administered, as PCC were not available. The management of airway compromise in RH remains controversial; primary conservative care should be favored with close observation. However, if dyspnea occurs, either tracheotomy or endotracheal intubation must be performed. 15 In our case, the onset of dyspnea was abrupt, requiring urgent tracheotomy. Endotracheal intubation as a secondary option proved challenging due to the localization of the hematoma.
Finally, waiting for the resorption of the hematoma is possible within 3 to 4 weeks.16,17 Surgical removal becomes a viable option after 3 or 4 days, offering a shorter recovery period and improved prognosis. 17 The transoral pharyngeal aspiration represents the simplest approach, but some authors prefer a lateral cervical approach to quickly evacuate the hematoma and insert 2 drains into the retropharyngeal space. 18 The latter approach is associated with a lower risk of contaminating the mediastinum. Unfortunately, the patient succumbed on the third day of hospitalization secondary to respiratory arrest. Prophylactic tracheotomy must be considered even in the absence of respiratory distress signs. Ultimately, the prognosis for SRH remains favorable when the diagnosis is made early and promptly followed by appropriate treatment.
Conclusion
Although relatively rare, SRH should be considered as a differential diagnosis in the presence of acute dysphagia. Its potential for fatal progression justifies abandoning primary conservative cares and adopting invasive measures, even in the absence of dyspnea. Tracheotomy and surgical evacuation of the RH are recommended to ensure a favorable prognosis and swift recovery.
Footnotes
Abbreviations
RH : Retropharyngeal hematoma
CH : Cervical hematoma
SRH: Spontaneous Retropharyngeal Hematoma
VKA: Vitamin K antagonists
INR : International Normalized Ratio
CT : Computed tomography
MRI : Magnetic resonance imaging
PPC : prothrombin complex concentrates
Consent to Participate
Written informed consent was obtained the legally authorized representative of the subject for his participation in this case report. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Consent for Publication
Written informed consent was obtained from the legally authorized representative of the subject for his participation in this case report. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Author Contributions
Hatim Bensouda Korachi and Safa Darouich took part in gathering patient data, researching the bibliography and writing the article.
Said Anajar, Mustapha Essaadi and Khalid Snoussi took part in editing the article and approved the final manuscript.
Amal Hajjij approved and validated the final manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.