
Abstract
Objectives
Hematoma in the retropharyngeal space (RPS) is a life-threatening condition that leads to rapid airway obstruction. However, the indication for airway management remains unclear. Additionally, the requirement for surgical hematoma evacuation remains undetermined. Therefore, we attempt to suggest some criteria for the management of hematoma in such cases.
Methods
We report three cases of hematoma in the RPS wherein one patient was treated without surgery and the other two underwent tracheotomy followed by hematoma evacuation.
Results
We found that airway management should be based on whether the glottis could be visible on laryngoscopy and dyspnea severity. The degree of hematoma, swelling, subcutaneous bleeding in the anterior neck, and emotional stability should also be considered. Proper management during the acute phase may allow for conservative treatments. Hematomas extending below the tracheal bifurcation may help ease upper airway obstruction due to pressure distribution, allowing for conservative treatment. When hematomas are surgically evacuated, tracheotomy should be performed simultaneously. Our report suggests that mediastinal hematoma evacuation could be avoided.
Conclusion
We should determine a therapeutic strategy for hematoma in RPS based on glottis visualization, patient’s condition, and extent of hematoma growth under careful observation.
Introduction
Hematoma in the retropharyngeal space (RPS) arising from various events such as blunt trauma, orthopedic surgery, and stellate ganglion block (SGB) is rare. However, it extends rapidly to the mediastinum and leads to upper airway compromise, resulting in a life-threatening condition, reportedly causing death. Therefore, airway management must be a key priority. 1 In some cases, tracheal intubation would be difficult owing to laryngeal edema, requiring urgent cricothyrotomy or tracheotomy. However, some patients could survive without airway management. 2 Since conservative treatment is particularly recommended for managing hematomas, the indications for airway management and transcervical hematoma evacuation remain unclear. 3 -5 Furthermore, whether hematomas in the mediastinum should be evacuated remains undetermined; accordingly, treatment decisions are controversial. In 2017, Song et al 6 reported a provisional guideline for postoperative retropharyngeal hematoma caused by anterior cervical fusion. However, in this therapeutic guideline, the initial evaluation event was cyanosis that resulted from oxygen desaturation, suggesting that early assessment was necessary for favorable management. Laryngoscopy is the most efficient tool for evaluating the upper airway. Most cases of RPS hematomas have been reported by emergency physicians and orthopedists. Therefore, to establish a new treatment algorithm for managing RPS hematoma, it is vital to educate otolaryngologists. 7 Moreover, since few studies have focused on the criteria for selecting proper treatment, further studies are necessary to identify the indications for airway management and hematoma evacuation. In this report, we reviewed three cases of hematoma in the RPS and discussed the determinants of surgical decision-making.
Case series
Case 1
A 53-year-old male patient who underwent SGB for pain caused by herpes zoster experienced dyspnea several hours after the procedure and was immediately hospitalized at another hospital. Although the anterior neck swelling was small and subcutaneous bleeding was unclear, plain computed tomography (CT) showed hematoma in the RPS extending from the cranial base to the mediastinum (Figure 1). Therefore, the patient was referred to our hospital the following day. Although laryngoscopy findings revealed a severely swollen retropharyngeal wall, glottic movement was confirmed (Figure 1). Considering the low level of progression of the hematoma on CT and the fact that the patient had mild dyspnea without a comorbidity, conservative treatment under careful observation was performed. Sulbactam sodium (4.5 g/day) was administered to prevent infections, and a feeding tube was used for nutrition management. Consecutive CT images taken for three days showed minor changes in the hematoma. Therefore, CT was performed at longer intervals. Laryngoscopy demonstrated pooling saliva occurring in the hypopharynx, resulting in silent aspiration pneumonia 10 days after hospitalization (Figure 1). The antibiotics were switched to tazobactam (13.5 g/day), by which the pneumonia improved. Thereafter, the patient had no signs of infection and could start oral intake at 27 days and was discharged at 37 days after hospitalization. The hematoma in the RPS completely resolved 68 days after hospitalization (Figure 1). Retropharyngeal hematoma extending from the cranial base inferior to the tracheal bifurcation is shown as (A) and yellow arrowheads in (B). The laryngoscope shows a severely swollen retropharyngeal wall (C). By contrast, on day 10, remarkable saliva pooling has emerged (D), leading to silent aspiration pneumonia.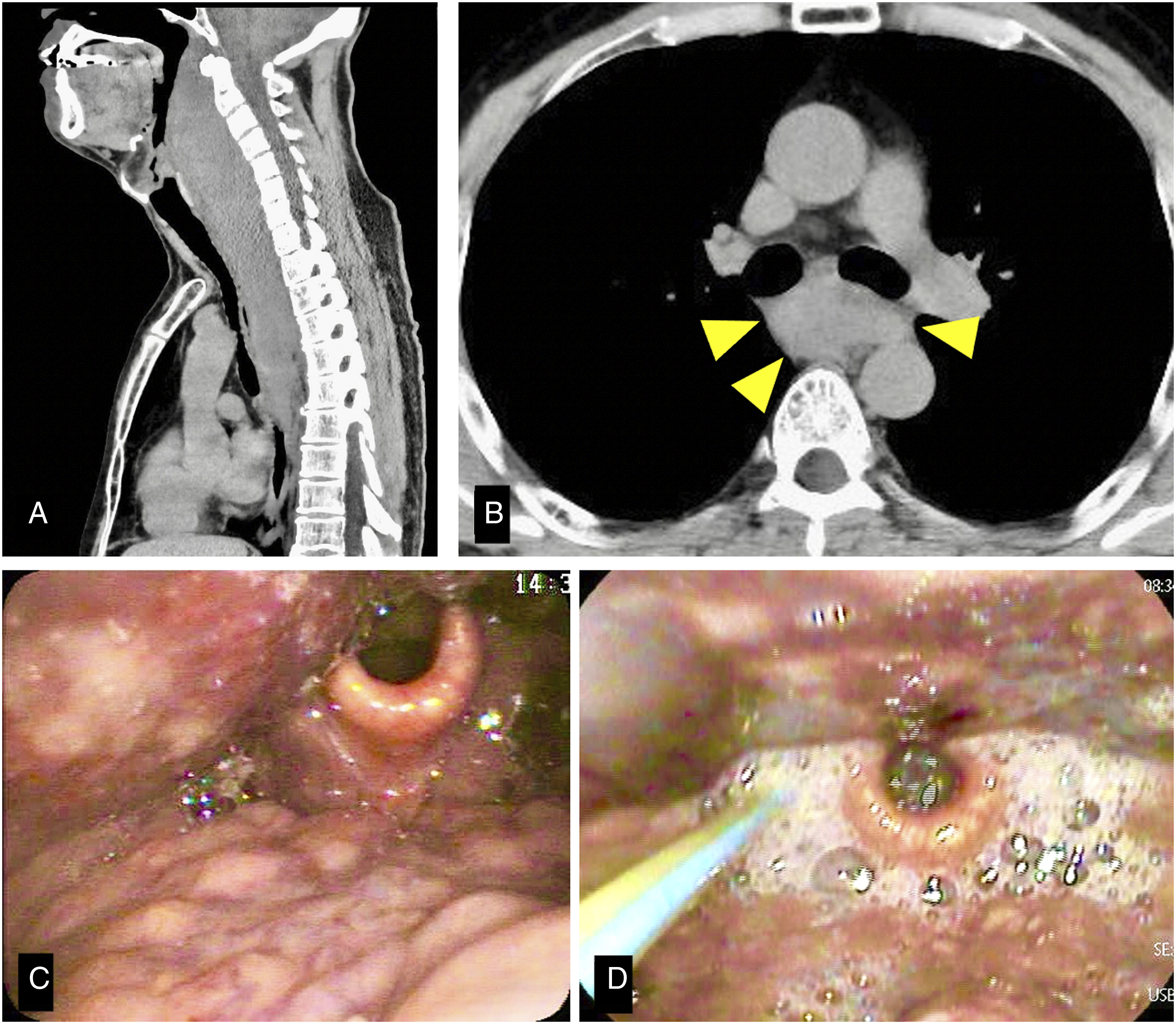
Case 2
A 44-year-old male patient presented with dyspnea 2 h after undergoing SGB and was urgently admitted to our hospital. In addition to exhibiting the anterior neck swelling and reddish coloration, laryngoscopy showed that the retropharyngeal wall and tongue root were severely swollen and the glottis was not visible, necessitating an emergency surgery. Although the breathing deteriorated during surgery, tracheotomy was completed without oxygen desaturation. Since the extent of the hematoma expansion had been preoperatively unconfirmed, the hematoma from the level of the cricoid to the lower neck was evacuated. Postoperative contrast-enhanced CT showed that the mediastinal hematoma persisted (Figure 2). Subsequent laryngoscopy findings and CT images showed no signs of hematoma deterioration. Therefore, oral intake was started three days after surgery. The hematoma completely resolved at 14 days after admission. At 19 days, the patient was discharged with the tracheal stoma closed. Postoperative computed tomography indicates a drain placed posterior to the trachea at the level of the thyroid (A). Retropharyngeal hematoma has remained in the mediastinum (B).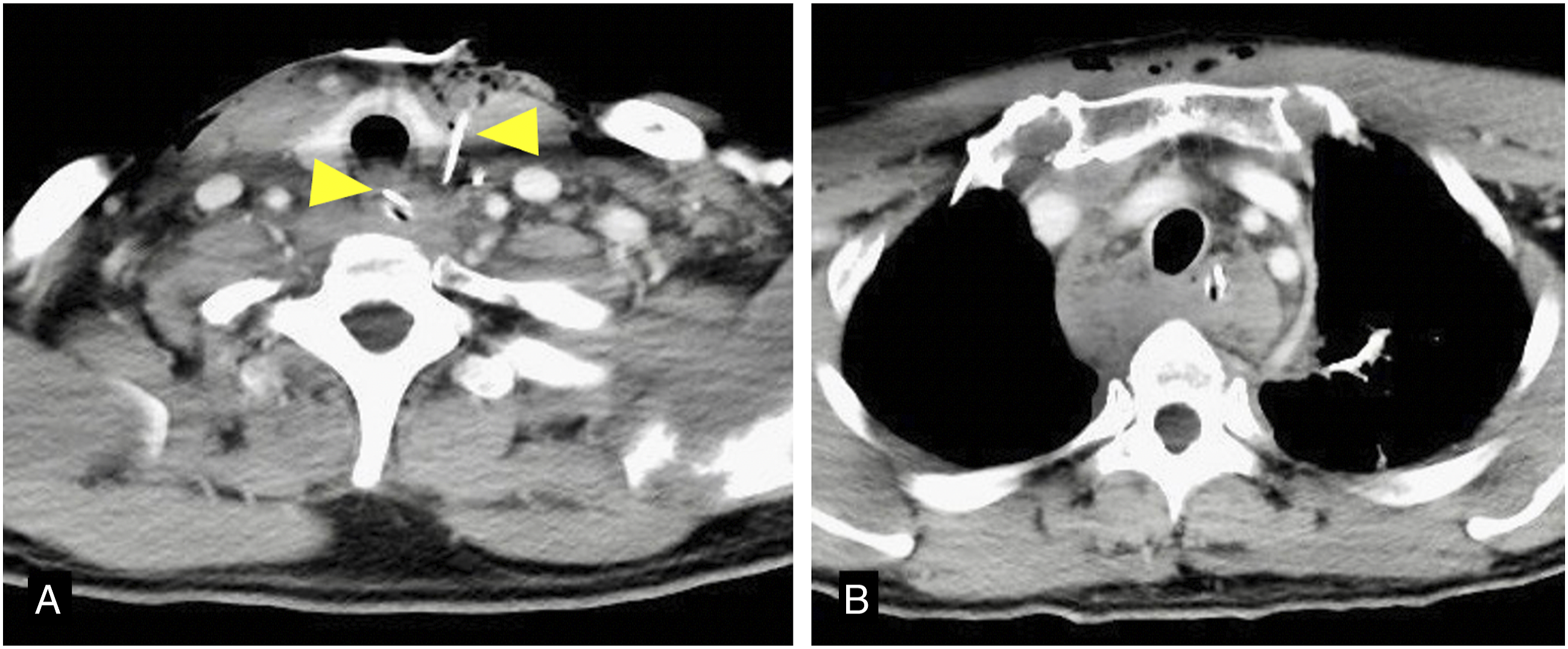
Case 3
A 74-year-old female patient, who experienced stridor and severe dyspnea two days after a blunt trauma to the anterior neck, falling off a bed, was referred to our hospital. In addition to extensive swelling and reddish coloration on the anterior neck, laryngoscopy findings revealed a severely swollen retropharyngeal wall, particularly around the upper airway; hence, the glottis was not visible. Contrast-enhanced CT images showed a non-enhanced mass in the RPS of the oropharynx close to the mediastinum. Based on the clinical course, hematoma in the RPS was suspected (Figure 3). Therefore, tracheostomy and hematoma evacuation were immediately performed. The hematoma extending from the cranial base to the mediastinum was confirmed and evacuated. The causative vessel was undetected on three-dimensional CT angiography the following day. Oral intake was started five days after surgery. The hematoma resolved 13 days after surgery. At 17 days, the patient was discharged with natural closure of the tracheal stoma. Retropharyngeal hematoma has predominantly arisen in the upper airway, leading to airway compromise as shown in (A) and (B).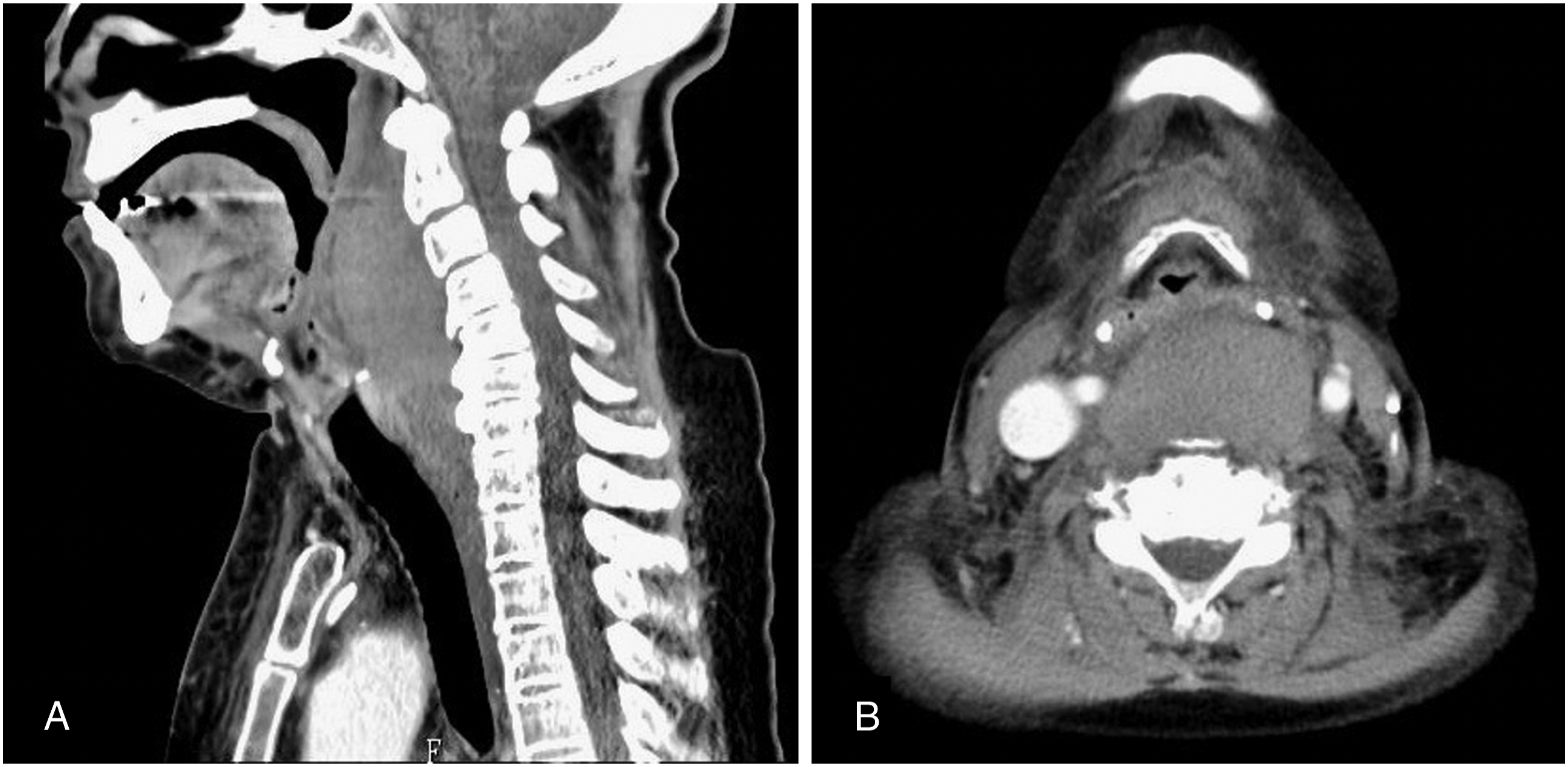
Characteristics of three cases of retropharyngeal hematoma.

SGB: stellate ganglion block.
Treatment and postoperative condition of the cases of retropharyngeal hematoma.

Discussion
We report the cases of three patients with RPS hematoma: one underwent conservative treatment, while the other two underwent tracheotomy and hematoma evacuation. Two of the three cases were induced by SGB treatment, the incidence rates of which are reported to be one in 90 000–100 000. 8 The RPS extends from the cranial base to the superior mediastinum and contains loose connective tissue, and bleeding in this region can rapidly deteriorate. Therefore, hematoma in the RPS can cause life-threatening upper airway obstruction. According to previous reports, conservative treatment is recommended; most patients undergo airway management, such as tracheal intubation or tracheotomy. 3 However, few studies have focused on the determinants for choosing between surgical and non-surgical treatment. In addition, otolaryngologists are rarely involved in decision-making for airway management. The primary requirement for conservative treatment is to ensure that the glottis is visible on laryngoscopy. Furthermore, a comprehensive evaluation is necessary considering the following aspects: the degree of dyspnea; range of the hematoma expansion; swelling and subcutaneous bleeding of the anterior neck; patient’s age and mental state; and medical history of immunosuppression and anticoagulants administration.
As shown in Tables 1 and 2, patient 1 was a healthy middle-aged man with mild dyspnea whose glottic movement was visible and had a stable RPS hematoma, in which conservative treatment was provided under careful observation. A hematoma in the RPS is likely to be treated conservatively if airway compromise in the acute phase is properly managed. Owing to the extensive hematoma in Case 1, the start of oral intake took much longer than that in the other patients who underwent hematoma evacuation. Since this patient also had a hospitalization length that was twice as long as that of the others, the socioeconomic background should be considered when selecting conservative treatment. Furthermore, the period of hematoma resolution was five times longer than that in the other cases, requiring a longer time for preventive antibiotics.
Taken together, conservative treatment appears to require longer healing time than surgical treatment, as noted in previous case reports. Moreover, silent aspiration pneumonia occurred during conservative treatment in our patient, suggesting that patients must be in a good general condition to undergo such treatment. If the patient is in a generally good condition, even extensive hematomas could be cured without any surgery. Hematoma in the RPS extending below the tracheal bifurcation, such as in case 1, might unexpectedly help ease the swelling in the peri-laryngeal airway, ranging from C3 to C4, and thus alleviate airway obstruction. Hemostasis treatment was not performed because CT images did not show further deterioration after onset. In cases of suspected active bleeding, CT angiography is recommended to detect the causative vessel, and embolization would be beneficial. However, angiography has been reported to carry a 1% risk of stroke when used to evaluate head and neck vessels. 9
Regarding airway management, transoral intubation is occasionally difficult due to laryngeal edema. Some studies reported that transoral intubation itself could possibly induce rupture of hematoma and may be contraindicated. 10 Although endoscopy-assisted intubation or intubation with McGRATHTM MAC (Medtronic, Dublin, Ireland) is possible, 11 tracheotomy should be performed in parallel in emergency cases.
Hematoma evacuation is recommended for cases in which tracheotomy is required and early extubation is desirable. Case 2 suggests that mediastinal hematoma evacuation may be avoided in an RPS hematoma. In fact, the mediastinal hematoma was intact during surgery in case 2. However, the result was similar to that in case 3, where the RPS hematoma was completely evacuated. To prevent complications and infection like mediastinitis, a hematoma below the mediastinum should be monitored rather than surgically evacuated. Although a hematoma infection causing an abscess rarely occurs, this infection is likely to cause mediastinitis, suggesting that antibiotics should be administered prophylactically.
Since hematomas in the RPS can result in rapid upper airway compromise, otolaryngologists should be involved in treatment decision-making. In addition to educating otolaryngologists, further studies are necessary for establishing appropriate treatment algorithms for hematomas in the RPS.
Footnotes
Author contributions
MS was responsible for conceptualization, data curation, drafting, and review of the manuscript for technical contents. NO assisted with data curation, writing the original draft, and reviewing the manuscript. SK assisted with drafting the manuscript. RY assisted with writing and reviewing the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability
Data available on request due to privacy/ethical restrictions.
Ethics approval
All study participants, except for one patient who died, provided informed consent.