
Abstract
A case of massive muscular bleeding of iliopsoas resulting in lethal exsanguination is presented. The intramuscular bleeding occurred spontaneously in an old man with heart failure, presented to the emergency department after the acute onset of shortness of breath, and treated with therapeutic doses of antiplatelets and heparin to prevent thrombosis. On the sixth day of recovery, pain in the left lumbar region develops while there was a decrease in hemoglobin level. Computed tomography (CT) scan revealed a 10 × 3 cm hematoma of the left iliac muscle. The treatment was immediately stopped, but within 6 hours, the death was confirmed. The autopsy revealed that the hematoma, and its increased size since the latest imaging assessment, was the leading cause of death. Particularly in older patients with comorbidity, even in those with clotting parameters in the therapeutic range, the potential for fatal result of iliopsoas muscle bleeding should be considered. Identifying potential patience with increased risk of this complication could be important, especially in pandemic time of COVID-19, when the use of anticoagulant therapy—both for treatment and for prevention of severe disease—has become massive and addressed also to people without previous and specific pathologies.
Keywords
Introduction
Iliopsoas hematoma (IPH) is a rare complication associated with hemorrhagic diathesis, trauma, and anticoagulant therapy. The symptoms and natural history range from mild pain to femoral neuropathy, up to abrupt shock and cardiovascular collapse. 1 Diagnosis is challenging depending on clinical features and imaging studies. Contrast-enhanced computed tomography (CT) scan is the most sensitive way to confirm hematoma. 2 Conservative management (bed rest, medication cessation, volume replacement, and blood transfusion) is usually sufficient when a small hematoma is not associated with active bleeding. 3 In patients with severe hemorrhage, surgical decompression or transcatheter arterial embolization may be considered.4-6 The most serious consequences usually involve elderly patients in whom symptoms are often non-specific or easily overlooked if cognitive impairment is present. 7 Rarely, in the literature, IPH is described as a potentially lethal disease. We report such an event.
Case Report
An 82-year-old Caucasian presented to the emergency department due to acute-onset shortness of breath. His medical history included hypertension, ischemic cardiopathy treated with PTA (percutaneous transluminal angioplasty) and coronary stent, chronic obstructive pulmonary disease (COPD), and previous hip fracture treated with arthroprosthesis.
Home oral therapy was angiotensin-converting enzyme (ACE) inhibitors (ramipril 5 mg), beta blockers (bisoprolol 2.5 mg), and antiaggregant (clopidogrel 75 mg).
Based on the clinical assessment reported in Table 1, after performing an echocardiogram showing an enlarged hypokinetic heart with reduced ejection function (35%), the patient was diagnosed with heart failure.
Day 1 Clinical Assessment.
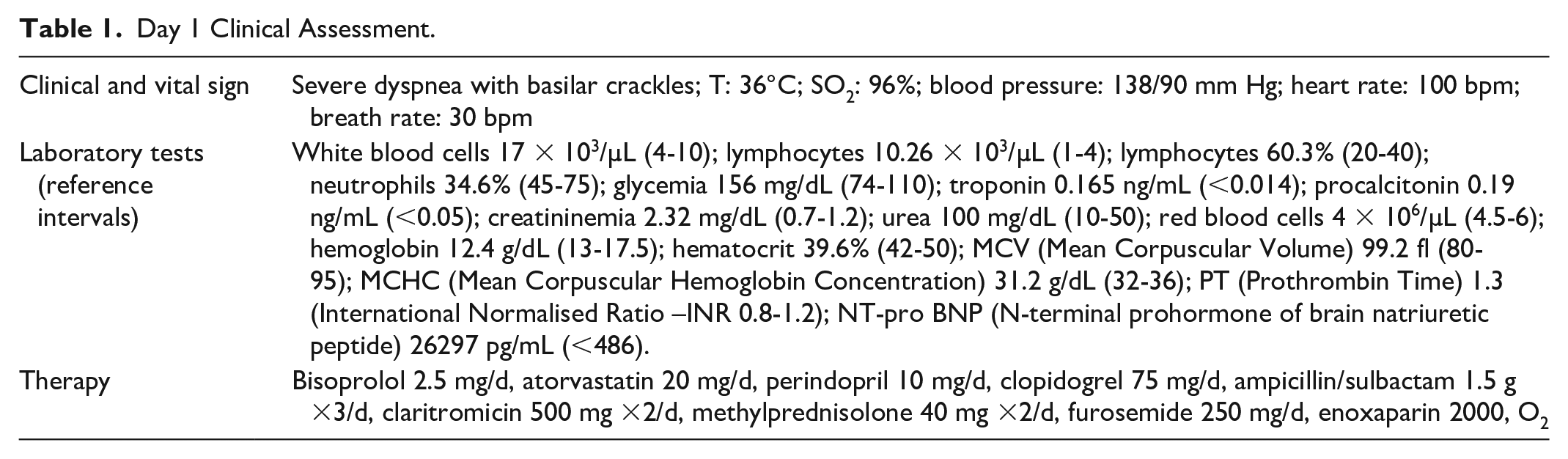
As shown in Table 2, clinical conditions, vital signs, and laboratory tests remain substantially unchanged until the sixth day of recovery when the patient experienced a sudden pain in the left lumbar, cold sweat with hypotension, and dropped into a state of unconsciousness. Laboratory test showed that hemoglobin levels had decreased to 5.3 g/dL within 24 hours, platelets to 65 × 103/µL, and activated partial thromboplastin time (aPTT) was delayed at 64.3 seconds.
Clinical Evolution.

Contrast-enhanced abdominal CT revealed a hematoma of the left iliac muscle with perilesional fluid collection as shown in Figures 1 and 2.
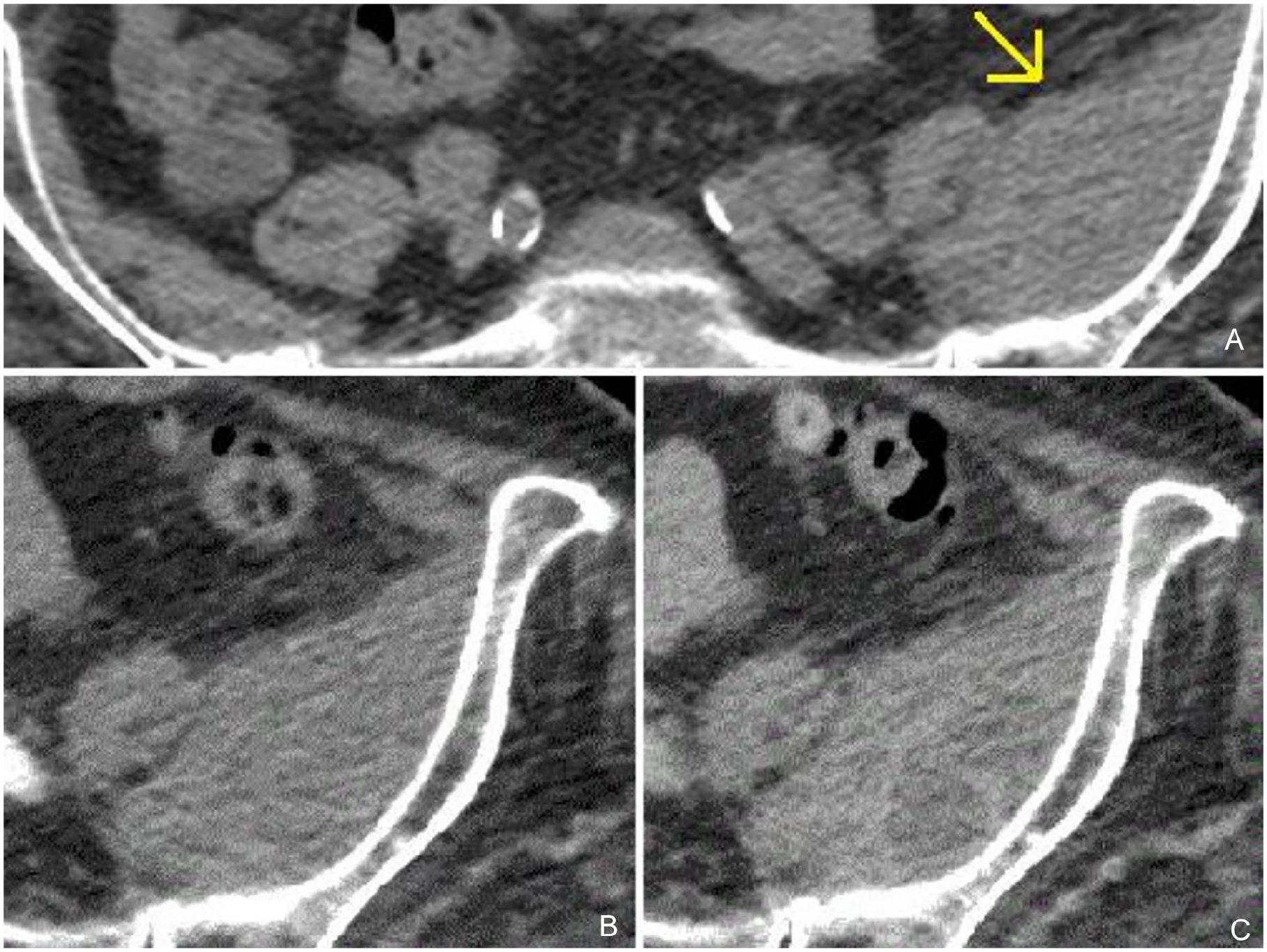
Computed tomography (CT) scans revealing the hematoma (yellow arrow). (A) scan for comparison with contralateral normal side and (B, C) zoomed scans of the hematoma

Computed tomography scans of the hematoma with size measurement. (A, B) scans revealing minum (A) and maximum (B) sizes of the hematoma.
Heparin and clopidogrel were stopped immediately, and a conservative approach was followed with rapid volume replacement and the transfusion of 4 units of packed red blood cells. Nevertheless, after 6 hours, he went into cardiac arrest. Cardiopulmonary resuscitation (CPR) failed and his death was confirmed.
At necroscopy, external examination revealed a significant ecchymosis emerging on the skin of the left lumbar region. Inner organs appeared widely pale. The heart was markedly dilated and hypertrophic. In the left ventricle, an acute sub-endocardial infarction was detected and confirmed by microscopy. Lungs were macroscopically and microscopically congested, as result of a severe acute cardiogenic pulmonary edema. After removal of abdominal internal organs, a large retroperitoneal hematoma (20 × 6 × 5 cm) infiltrating perirenal adipose tissue was observed, originating in the left iliopsoas muscle, and containing about 2350 to 2500 cm3 of blood (Figure 3).
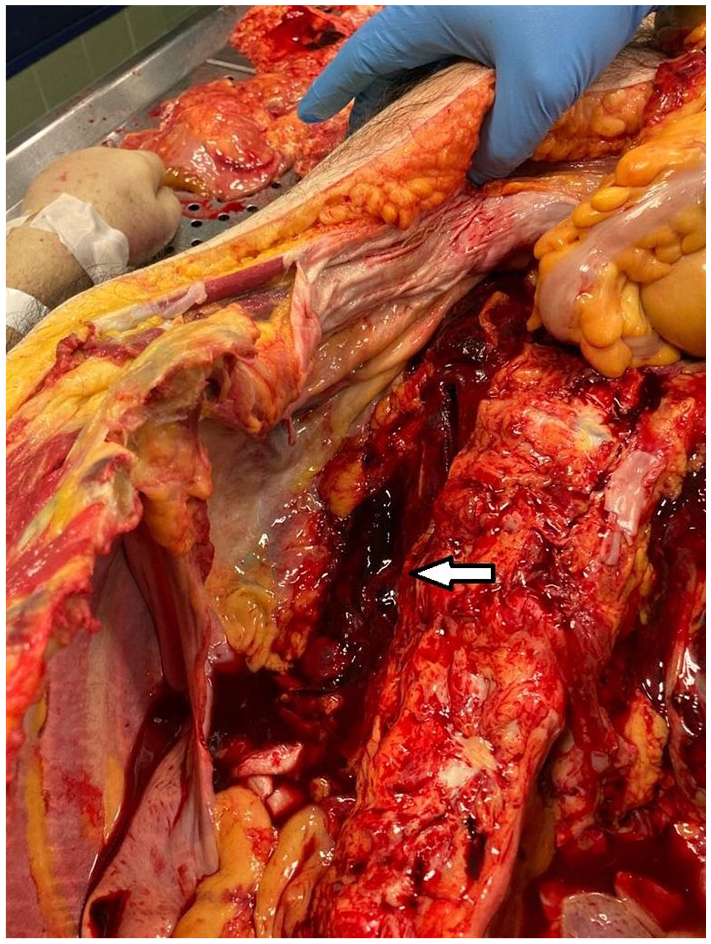
Hematoma revealed at the autopsy (white arrow).
Discussion
Severe or even life-threatening IPH is such a rare condition.
Some case of IPH has been observed following muscle injuries due to a direct trauma or strain,8,9 and even due to an indirect minor trauma as a coughing attack, but in a patient with hemophilia A. 10 However, serious consequences are usually related to a spontaneous hemorrhage.
Almost all patients with severe IPH were described in therapy with antiplatelets agents, oral anticoagulants, or heparin within the therapeutic range. Also, congenital or acquired coagulopathy (like hemophilia or liver failure) represent major risk factors.11-16 It is usually unilateral but may occur bilaterally.10,17,18
The incidence of spontaneous IPH in intensive care unit hospitalizations ranges from 0.3% to 0.4% with this kind of patients having an estimated mortality rate between 30% and 50%.19,20
The symptoms are often non-specific or atypical, as the characteristic Lenk’s triad (severe flank pain, hemodynamic shock, and palpable mass) only presents in one-third of the cases. 21 Therefore, the diagnosis is often causal performing wide spectrum diagnostics like a full body CT, as in the case presented.
The lack of level I evidence for the best management plans due to the rarity of reports makes necessary an individual clinical approach by properly assessing the risks and benefits before proceeding with any plan of action.
Two are the major issues that need to be discussed in our case.
The first one concerns the confirmation of IPH as the leading cause of death. The observed pronounced pallor of the inner organs (in Figure 1 it is possible to easily notice the pallor of the diaphragm and of the intercostal muscles) is a sure suggestion of severe hemorrhage. Also, severe and rapid anemia can induce a coronary hypoperfusion and sub-endocardial infarction due to an acute imbalance in myocardial oxygen supply and demand in the absence of atherothrombosis (Type 2 myocardial infarction), with worsening of left ventricle contractility, which led to an acute pulmonary edema, 22 as observed during the autopsy.
The second one is about the correlation between IPH development and anticoagulant therapy.
This can be easily established by the quick and the subsequent beginning of the therapy, rise of aPPT value, and symptoms onset.
Rarely, in the literature, cases characterized by a fatal outcome of spontaneous iliopsoas muscle bleeding are described.1,23
However, those have great differences with our case. The one reported by Maruyama et al 1 is characterized by an 80-day hospitalization with 64 days between the diagnosis of the IPH and the death. Moreover, death seems to be linked to an Escherichia coli-related pneumonia and subsequent sepsis, worsened by the compression of the hematoma on the diaphragm, which led to respiratory and hemodynamic instability.
On the contrary, the 2 cases reported by Türk et al 23 concern 2 people—one died before any diagnostic or therapeutic was possible and one found death at home—in which IPH represent only a postmortem diagnosis, such that no data about clinical presentation are available.
As IPH is related to the administration of anticoagulants, particular attention should be paid to COVID-19 patients, who are frequently administered a standard prophylactic anticoagulant therapy.
A recent report suggests that hospitalized COVID-19 patients treated with anticoagulant, often with low-molecular-weight heparin at therapeutic doses, are at risk of IPH. 24 According to the authors, up to January 2021, 12 cases of IPH in COVID-19 patients have been reported, and 3 of them were fatal with the hematoma playing a role in the determinism of death. 24 Al-Samkari et al 25 suggest that thrombocytopenia (platelet count <150 × 103 cells/μL, also observed in our case) and elevated D-dimer levels (>2.5 μg/mL) at initial presentation are predictive of hemorrhage-related complications during hospitalization and so may be monitored for a better and early management of potential life-threatening IPH.
Conclusions
Rarely, in the literature, similar cases characterized by such a rapid fatal outcome of spontaneous iliopsoas muscle bleeding are described.
Especially in older patients with comorbidity, in therapy with anticoagulants, a potentially fatal outcome of IPH should be considered.
The case presented is intended to contribute to the discussion on psoas hematoma, helping to identify and prevent sensitive cases that could result in death.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the patient’s relatives for their anonymized information to be published in this article.