
Abstract
Vitamin D deficiency is a significant public health concern that affects bone health and muscle function in children, especially in developing countries. The COVID-19 pandemic has intensified this issue because lockdowns have reduced sunlight exposure. We report a rare case of a 13-year-old Indian boy who developed severe proximal myopathy induced by vitamin D deficiency during the pandemic. The patient presented with generalized body aches, progressive lower limb weakness, difficulty walking, waddling gait, and a positive Gower’s sign. Laboratory tests revealed severe hypovitaminosis D (25[OH]D level, 3.8 ng/ml), hypocalcemia, hypophosphatemia, elevated parathyroid hormone, and elevated alkaline phosphatase levels. Electromyography and nerve conduction study results were normal. The patient was diagnosed with vitamin D deficiency-induced proximal myopathy and osteomalacia, likely due to reduced sunlight exposure, inadequate dietary intake, and obesity. The treatment involved high-dose vitamin D supplementation, oral calcium, lifestyle modifications, and a structured physiotherapy program focusing on resistance training and functional mobility exercises. Despite biochemical normalization after 2 months, significant symptomatic improvement was achieved only after intensifying physiotherapy. By 7 months, the patient had fully recovered muscle strength, achieved normal gait, and maintained normal follow-up laboratory values. This case emphasizes the importance of considering vitamin D deficiency in children with muscle weakness during periods of limited sunlight exposure, and highlights the need for a multidisciplinary approach for effective management and full functional recovery.
Introduction
Vitamin D deficiency is a widespread public health issue affecting bone mineralization and neuromuscular function, particularly among children in developing countries. 1 Despite abundant sunlight, studies indicate that 80% to 85% of Indian children suffer from hypovitaminosis D.2,3 Vitamin D is synthesized in the skin upon exposure to ultraviolet B (UV-B) radiation and minimally obtained through dietary sources. Common causes of deficiency include limited sunlight exposure, inadequate dietary intake, malabsorption syndromes, increased catabolism, and obesity. 4 The clinical manifestations of vitamin D deficiency range from asymptomatic biochemical abnormalities to rickets and osteomalacia. Proximal myopathy associated with vitamin D deficiency in the pediatric population is under-recognized and often misdiagnosed due to nonspecific symptoms. 5 Most documented cases of vitamin D deficiency-related myopathy involve adults, making pediatric presentations particularly rare. 6
The COVID-19 pandemic has exacerbated vitamin D deficiency due to lockdown measures restricting outdoor activities, thereby reducing sunlight exposure. 7 Although cases of pediatric vitamin D deficiency-induced myopathy have been documented pre- and post-pandemic, severe presentations remain uncommon.8,9 A recent Indian study identified 31 cases of proximal myopathy due to vitamin D deficiency (VDD) in children between November 2021 and May 2022. 10 However, our patient’s case, occurring during the 2021 lockdown, is notable for its profound severity of deficiency, the added impact of overweight status on vitamin D metabolism, and the extended recovery period required for full functional restoration, even after achieving biochemical normalization. This case highlights the challenges in diagnosing and managing severe VDD-induced proximal myopathy in pediatric patients during pandemic restrictions, and emphasizes the importance of holistic treatment approaches for achieving complete recovery.
Case Report
A 13-year-old Indian boy presented with a 3-month history of generalized body aches, progressive lower limb weakness, and gait difficulties. His symptoms began as lethargy and fatigue, escalating to difficulty climbing stairs and rising from a seated position, respectively. The patient eventually developed a waddling gait and required assistance for mobility. The sole significant medical event was laparoscopic appendectomy 9 months earlier. There was no history of trauma, chronic illness, neurological disorders, or familial muscle disease, and he had no long-term medications or known allergies.
Dietary assessment showed a predominantly meat-based diet with limited dairy, fruits, and vegetables. He consumed meat approximately 5 times per week, but rarely consumed fish or vitamin D–fortified foods. During the strict 2021 lockdown, he had less than 1 hour of weekly sunlight exposure for 6 months, staying mostly indoors with significant screen time and minimal physical activity.
On examination, he weighed 54 kg and was 143 cm tall, yielding a BMI of 26.4 kg/m², classified as overweight according to World Health Organisation (WHO) standards for children. 11 Vital signs were normal. Musculoskeletal assessment revealed proximal lower limb weakness (Medical Research Council grade 3/5), while upper limb strength remained intact (5/5). He had a waddling gait and a positive Gower’s sign. No fasciculations, atrophy, or hypertrophy was observed. Deep tendon reflexes were normal and symmetrical, and the sensory examination was intact. The neurological findings were unremarkable. Neuromuscular irritability tests showed negative Chvostek’s and Trousseau’s signs despite hypocalcemia.
Laboratory evaluations (Table 1) showed hypocalcemia (7.6 mg/dl), hypophosphatemia (2.5 mg/dl), and a markedly low serum 25-hydroxyvitamin D [25(OH)D] level (3.8 ng/ml). The parathyroid hormone (PTH) level was elevated (85 pg/ml), indicating secondary hyperparathyroidism, and alkaline phosphatase level (280 U/l) suggested increased bone turnover. Muscle enzymes (including creatine kinase), inflammatory markers (ESR and CRP), and thyroid function test results were normal. Serum vitamin B1 (thiamine) levels were checked to exclude deficiency-induced myopathy. 12 Electromyography (EMG) and nerve conduction studies (NCS) ruled out neuromuscular disorders. X-rays of the pelvis and lower limbs were unremarkable, but a Dual-Energy X-ray Absorptiometry (DEXA) scan of the lumbar spine and proximal femur showed a Z-score of −2.5, confirming osteomalacia. Magnetic Resonance Imaging (MRI) of the lower limbs was also normal.
Laboratory investigations demonstrating biochemical abnormalities consistent with vitamin D deficiency.

Potential differential diagnoses included muscular dystrophies, inflammatory myopathies, endocrine myopathies, and electrolyte imbalance. Muscular dystrophies were deemed unlikely because of normal CK levels, no muscle atrophy, and normal EMG findings. Inflammatory myopathies were ruled out by normal inflammatory markers and MRI, whereas normal thyroid function tests excluded hypothyroidism. No significant electrolyte abnormalities (beyond hypocalcemia and hypophosphatemia) were detected.
Based on the clinical picture and investigations, a diagnosis of vitamin D deficiency-induced proximal myopathy and osteomalacia was made, which was likely triggered by reduced sunlight exposure, poor dietary intake, and obesity during the COVID-19 lockdown. Treatment began with cholecalciferol 60 000 IU weekly for 8 weeks (total 480 000 IU), followed by 800 IU daily and 1000 mg/day of oral elemental calcium. Lifestyle modifications included daily sunlight exposure of at least 30 minutes (10 a.m.-3 p.m.) and dietary counseling to incorporate vitamin D-rich foods (eg, fortified dairy, eggs, fatty fish). Physical activity was encouraged to address the patient’s overweight status. A structured physiotherapy program was instituted 5 times per week, with each 45-minute session focusing on progressive resistance exercises for proximal muscles, functional mobility drills (sit-to-stand, step-ups), gait training to correct the waddling pattern, and balance exercises to reduce fall risk.
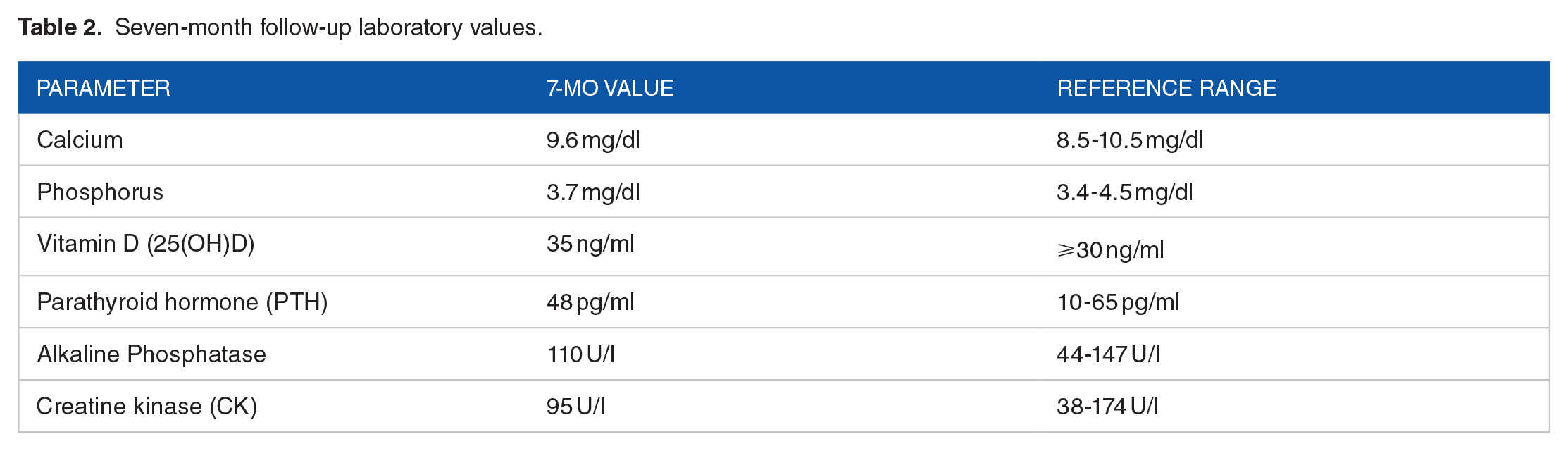
After 2 months, laboratory tests showed a vitamin D level of 38 ng/ml, normalization of calcium (9.8 mg/dl) and phosphorus (3.7 mg/dl), and a reduction in PTH to 50 pg/ml. Despite these biochemical improvements, the patient experienced minimal symptomatic relief. Recognizing that muscle recovery often lags behind biochemical normalization, the physiotherapy regimen was intensified to include greater resistance and more challenging functional exercises. By the 7-month follow-up, he had fully regained muscle strength (5/5), achieved a normal gait, resolved the Gower’s sign, and returned to daily activities without assistance. Laboratory results at 7 months (Table 2) indicated sustained normalization of vitamin D (35 ng/ml), calcium, phosphorus, PTH, and alkaline phosphatase levels, confirming stable musculoskeletal health.
Seven-month follow-up laboratory values.
Discussion
This case highlights a rare occurrence of vitamin D deficiency-induced proximal myopathy in a pediatric patient during the COVID-19 pandemic. Unlike previously reported cases, our patient’s course was complicated by profound hypovitaminosis D, overweight status potentially affecting vitamin D storage and bioavailability, and a protracted interval between biochemical normalization and functional recovery. The lockdown measures led to reduced sunlight exposure, which, along with inadequate dietary intake and obesity, contributed to severe hypovitaminosis D. Vitamin D plays a crucial role in muscle function through several mechanisms. It promotes protein synthesis, muscle cell proliferation, and differentiation by binding to vitamin D receptors (VDRs) in muscle tissue. 13 Deficiency leads to muscle fiber atrophy, particularly of type II fast-twitch fibers, resulting in proximal muscle weakness. 14 Additionally, hypocalcemia can impair excitation-contraction coupling in muscle cells. 15
Excess adiposity in overweight children can sequester vitamin D within adipose tissue, reducing its circulating bioavailability and exacerbating deficiency. 16 This may have contributed to the severity of deficiency in our patient. Delayed symptomatic improvement despite biochemical normalization highlights the time required for muscle repair and regeneration. Vitamin D supplementation corrects serum levels but may not immediately reverse muscle atrophy. 17 Physiotherapy enhances muscle strength and function by stimulating muscle protein synthesis and promoting neuromuscular adaptations. 18 High-dose vitamin D therapy was justified and safe in this case. Guidelines recommend doses ranging from 2000 to 6000 IU daily (or equivalent weekly doses) for children with severe deficiencies. The total cumulative dose administered was within the recommended limits and did not result in adverse effects.
Some investigators have posited that certain genetic polymorphisms, specifically rs731236 and rs2228570, within vitamin VDR genes, can modify the clinical severity of deficiency by altering receptor sensitivity. 19 These polymorphisms may lead to differential binding affinities or variations in signal transduction pathways, thereby affecting muscle fiber function and response to supplementation. Emerging epigenetic research also indicates that environmental factors—such as nutritional deficits and sedentary lifestyles—can induce stable changes in gene expression without altering DNA sequences. 20 Future studies could explore whether targeted genetic or epigenetic profiling of pediatric patients might refine dosing regimens and provide more individualized treatment plans for vitamin D deficiency-induced myopathy.
While vitamin D and calcium therapy form the cornerstone of treatment, optimal recovery may also depend on adequate levels of other micronutrients including magnesium, phosphate, and vitamin K2. Recent studies have suggested that magnesium repletion can boost the effectiveness of vitamin D supplementation by aiding its metabolic activation and improving neuromuscular function.21,22 Incorporating micronutrient assessments into the diagnostic workup may be beneficial, particularly in children with diets lacking green vegetables, whole grains, or dairy products. Such a comprehensive approach could potentially accelerate muscle strength gains and reduce the lag often observed between biochemical correction and return of normal motor function.
Although clinical examinations and basic laboratory assessments are standard for diagnosing vitamin D deficiency myopathy, newer diagnostic tools offer additional insights. Quantitative muscle ultrasound and magnetic resonance spectroscopy have been explored in various pediatric myopathies to evaluate muscle architecture and metabolic activity. 23 When combined with DEXA scans for assessing bone density, these modalities could help clinicians objectively monitor disease progression and therapeutic response. Incorporating advanced imaging into research settings might also clarify whether prolonged muscle weakness stems primarily from metabolic derangements, structural muscle damage, or a combination of both.
Beyond the acute phase of treatment, ongoing monitoring of vitamin D status is advisable to prevent relapse, especially in children with risk factors, such as obesity or limited outdoor exposure. Some clinicians advocate periodic serum 25-hydroxyvitamin D measurements, repeat dietary evaluations, and sustained exercise regimens. 24 Public health measuresranging from fortified school lunches to community-based physical activity programscould further reduce the incidence of clinically significant deficiencies. As societies adapt to future lockdowns or other circumstances that limit outdoor activities, preventive strategies that integrate nutrition, supplementation, and telehealth-based physiotherapy may play a crucial role in safeguarding pediatric musculoskeletal health.
The limitations of this case include its nature as a single case report, which may limit the generalizability of the findings to all pediatric patients. Clinicians should maintain a high index of suspicion for hypovitaminosis D in children presenting with muscle weakness, particularly during periods of reduced sunlight exposure. Early recognition and comprehensive management, including vitamin D supplementation, dietary modification, and physiotherapy, are essential for full functional recovery.
Conclusion
Vitamin D deficiency should be considered in pediatric patients presenting with proximal muscle weakness, particularly in the context of limited sunlight exposure, such as pandemic lockdowns. This case highlights the need for a multidisciplinary approach including vitamin D supplementation, calcium support, dietary counseling, lifestyle modifications to increase sun exposure, and structured physiotherapy to achieve complete recovery. Public health strategies include routine vitamin D supplementation during prolonged indoor confinement, encouraging brief safe sun exposure through windows or balconies, promoting fortified foods, and offering telehealth-based dietary and exercise guidance. By implementing these measures, clinicians and policymakers can mitigate the risk of severe vitamin D deficiency-induced myopathy and ensure prompt and complete functional restoration in affected children.
Footnotes
Acknowledgements
The authors would like to sincerely thank Medicos In Research, Nautanwa, UP 273164, India, for their unwavering support and guidance throughout every step of the development of this manuscript. Their invaluable contributions were instrumental in shaping this work, and we deeply appreciate their efforts. We also extend our gratitude to the medical staff of the Department of Pediatrics for their exceptional care during the patient’s treatment. Lastly, we thank the patient’s family for their cooperation and consent, which made this case report possible.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Dr. Arihant Surana was responsible for the clinical assessment and management of the patient in India. Dr. Amit Varma conducted the literature review and drafted the initial manuscript. Dr. Mahendra Pratap Singh and Dr. Sanjit Sah provided critical revisions and supervised the overall project. Dr. Mohammad Hazique, Dr. Aashna Mehta, Dr. Helen Huang, Dr. Surour Alneyadi, Kavita Shah, and Dr. Ajeet Singh contributed to data interpretation and manuscript editing. Dr. Amogh Verma coordinated and validated the project and finalized the manuscript. All authors have read and approved the final manuscript.
Data Availability
Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
Ethical Considerations
Ethical approval was not required for this case report as per the policies of our institution. The Institutional Review Board waived the need for approval in accordance with institutional guidelines for case studies.
Consent to Participate
Written informed consent to participate in this study was obtained from the patient’s parents.
Consent for Publication
Written informed consent for publication of this case report was obtained from the patient’s parents.