
Abstract
The respiratory impact of e-cigarette usage, also known as vaping, emerged as a significant healthcare issue in 2019. This concern arose due to the sharp rise in cases of e-cigarette or vaping-associated lung injury (EVALI) among adolescents and young adults. Now, systemic manifestations have been described. We present the case of a 39-year-old male patient who had been vaping for 5 years and developed EVALI associated with multiple severe complications, including acute myocardial infarction, metabolic acidosis, acute kidney injury and sepsis-like syndrome, requiring hospitalization in the critical care unit. Every day, reports of patients with systemic complications due to the use of e-cigarettes are becoming more frequent. Therefore, it is crucial for clinicians to be aware of this condition and to consider whether vaping truly constitutes a safe alternative to combat smoking.
Keywords
Introduction
Electronic cigarettes, or e-cigarettes (ECIGs), were developed in the early 2000s in China by pharmacist Hon Lik. 1 ECIGs are devices equipped with a heating element that generates nicotine vapor mixed with other solutions, stored in a reservoir for inhalation, vaping, devoid of smoke. 1 The solution, named as e-liquid, encompasses flavoring agents, propylene glycol, vegetable glycerin and nicotine, but it can also contain other substances as tetrahydrocannabinol, vitamins. 2
In recent times, vape pens have been endorsed as potential devices for smoking cessation, thus they are considered a healthier alternative to tobacco smoking. 3 Adult smokers are shifting towards using vape pens and ECIGs, leading to a reversal in nicotine use trends, with a noticeable increase in vaping among young individuals who have never smoked before. 4
According to the National Survey of the Consumption of Psychoactive Substances among middle school students for the year 2022 ECIGs are the second most consumed psychoactive substance by this population after alcohol, 22.7% of the students had vaped at some point in their lives.
According to the 2022 National Survey on the Consumption of Psychoactive Substances among School Population, 5 ECIGs or vapes are the second most consumed psychoactive substance by schoolchildren in Colombia after alcohol, with a lifetime prevalence of 22.7%, a past-year prevalence of 17.61%, and a past-month prevalence of 11.21%. The average age of initiation is 14.1 years. 5 This data is higher compared to the 2017 National Youth Smoking Survey, which found that 15.4% of Colombian schoolchildren aged 12 to 15 had used ECIGs at least once in their lifetime, and 9% had done so in the past 30 days. 6 On the other hand, the latest survey on Psychoactive Substance Consumption provided by National Administrative Department of Statistics (DANE for its acronym in Spanish) reports that 5% of the Colombian population between the ages of 12 and 65 has used ECIGs at some point, with the average age of initiation being 23 years old. 7 These patterns are mirrored globally, with the prevalence of vape products increasing in US, China, and the UK. 8
Despite being initially praised as a safer substitute for cigarette smoking, the presence of toxic substances in vape aerosols has brought forth concerns regarding the long-term safety of vaping.
Herein, we present the case of a 39-year-old male patient who had been vaping for 5 years and developed of e-cigarette or vaping-associated lung injury (EVALI) accompanied by multiple severe complications, highlighting the importance of knowing the potential harms of vaping as a challenge posed by a new generation of nicotine users in order to intervene on this new public health crisis.
This case report was approved for publication by the Research Ethics Committee of Fundación Santa Fe de Bogotá. Written informed consent for treatment and publication was provided by the patient. The reporting of this study conforms to the CARE guidelines.
Case Report
A 39-year-old male presented with a 10-day history of fever spikes, ranging from 38.6°C to 39°C, accompanied by a dry cough and a sensation of shortness of breath, particularly evident during short walks with perioral cyanosis. In the last 24 hours, he experienced oxygen desaturation to 85%, abdominal pain, and passed three liquid stools without mucus or blood. He reported a history of vaping product use over the past 5 years. During the physical examination, his temperature was 38.7°C, heart rate 115 beats/min, blood pressure normal, and respiratory rate 25 breaths/min. The patient exhibited hypoxia while breathing room air, along with signs of tachypnea without utilizing respiratory accessory muscles.
Laboratory tests revealed leukopenia and elevated serum creatinine at 1.49 mg/dL, with concurrent hyperkalemia (6.19 mEq/L), arterial blood gas analysis (ABG) with metabolic acidosis (pH 7.23, HCO3 11.1, pCO2 35, lactic acid 2.15 mEq/L), and an elevated anion gap (15, normal range 8-12). Respiratory viral panel and influenza testing were negative. Due to hyperkalemia, an electrocardiogram (EKG) was performed, showing sinus rhythm, left ventricular hypertrophy, and widespread T wave inversions (Figure 1).

EKG with sinus rhythm, left ventricular hypertrophy and widespread T wave inversions.
Chest imaging (X-ray and CT scan) revealed ground glass and alveolar opacities, predominantly towards the lung periphery, with no enlargement of cardiac cavities (Figure 2). The patient was subsequently transferred to the ICU, where he received intravenous ampicillin/sulbactam for treatment of a suspected infection, intravenous normal saline for volume depletion, and high-dose steroids, in addition to inhalers for symptom management. Despite treatment, his condition persisted, prompting consideration of worsening community-acquired pneumonia, possibly due to an antibiotic-resistant organism or an opportunistic infection caused by an undiagnosed immune deficiency.

(a) X-ray. Ground glass and alveolar areas can be seen, being more profuse towards the periphery of both lung fields. No growth of cardiac chambers is observed and there is respect for the cardio and costophrenic angles bilaterally. (b-d) Chest CT. Large bilateral symmetrical ground-glass and reticular opacities in a broncho vascular distribution with subpleural sparing affecting all lobes accompanied by bronchiectasis.
Further investigations included urine legionella and streptococcus antigen tests, as well as serum antinuclear antibody, antineutrophil cytoplasmic antibodies, and HIV antibodies, all of which returned negative. A fiberoptic bronchoscopy with bronchoalveolar lavage (BAL) and biopsy revealed an increase in lymphoplasmacytic infiltrate with interstitial and alveolar eosinophils, along with reactive changes in pneumocytes and a pattern of occupation of the alveolar spaces by fibrous tufts. Cultures from the BAL fluid were negative, while the biopsy indicated a pattern of subacute lung injury consistent with organizing pneumonia with eosinophils.
The patient received antibiotics and corticosteroids for 10 days, resulting in improved renal function and resolution of metabolic acidosis. There was no recurrence of fever or diarrhea, and the patient tolerated weaning off oxygen. However, he reported chest pain, prompting a new EKG, which revealed sinus rhythm with T wave inversions in leads V1-3 (Figure 3). Considering this result, a cardiology consultation was sought.

EKG showing sinus rhythm with T wave inversions in leads V1-3.
Transthoracic echocardiography showed a moderately reduced global systolic function (ejection fraction: 40%) with segmental wall motion abnormalities, including akinesia of the mid and apical thirds of the inferior septum and inferior wall, as well as the anterior septum with remodeling of the mid and apical thirds of the septum. Hypokinesia of the medial and apical inferior wall was also noted. Cardiac catheterization confirmed significant coronary artery disease involving one main vessel and one secondary vessel. Primary angioplasty with the implantation of a drug-eluting stent in the mid-segment of the left anterior descending artery and balloon angioplasty at the ostium of the diagonal branch was performed.
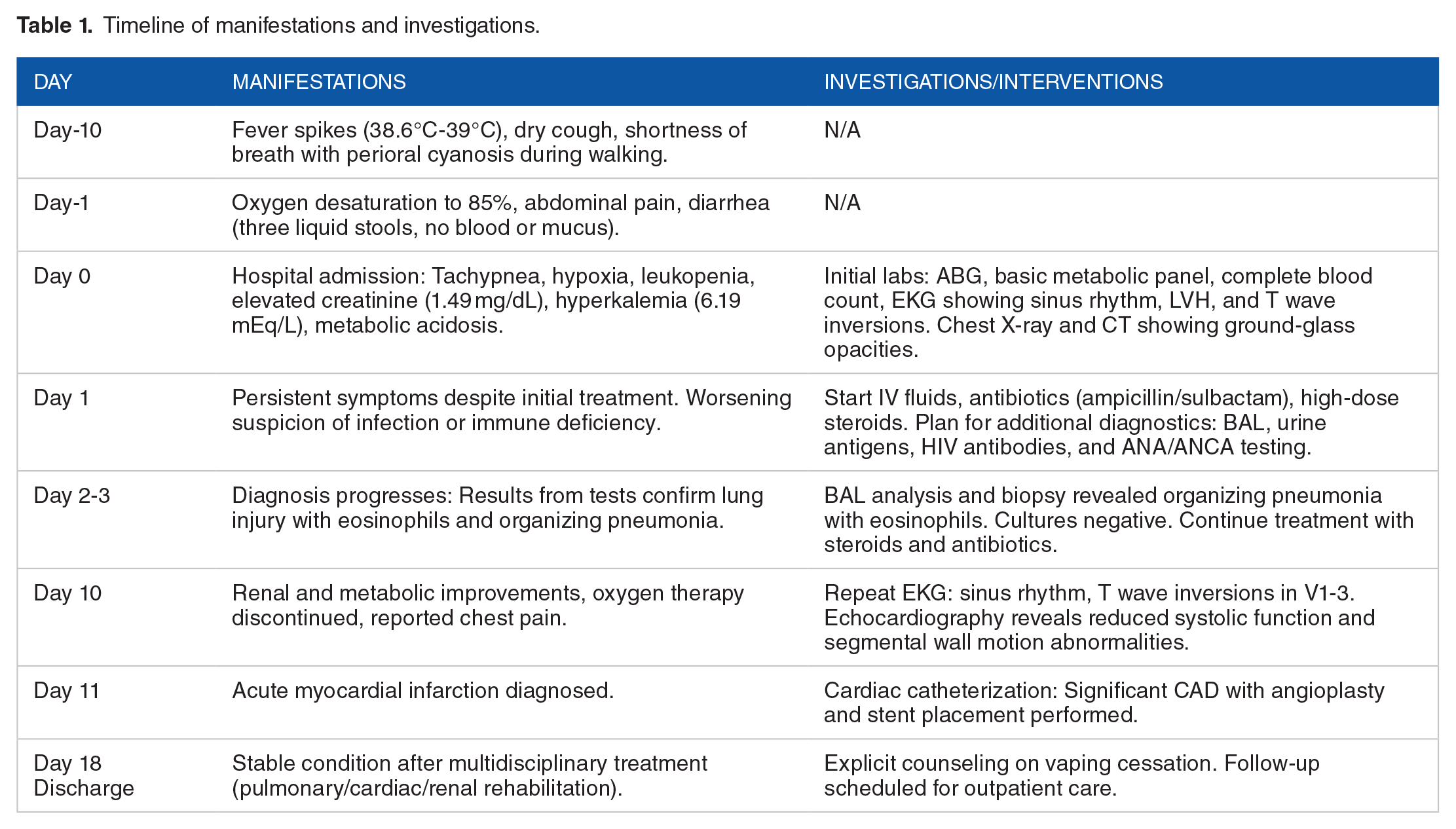
Upon discharge, the patient continued with physical therapy, pulmonary rehabilitation, and cardiac rehabilitation, with follow-up appointments scheduled in the outpatient clinic. Explicit counseling was provided to cease vaping, as it was likely the cause of his current hospital visit. Table 1 provides a chronological overview of the patient’s symptoms, diagnostic processes, and treatments
Timeline of manifestations and investigations.
Discussion
The possible health impact of using vape pens encompass a range of issues primarily focused on harm to the air passages and lung tissue.2,3 Prior to the 2019 EVALI crisis, medical studies documented instances of occasional acute lung injuries linked to vaping. 9 The earliest recorded case dates to 2012, when a patient exhibited symptoms, such as coughing, widespread ground glass opacities, and the presence of lipid-laden macrophages in BAL following vape pen usage. 10
In subsequent years, a diverse range of serious negative health outcomes has been reported, encompassing issues such as nicotine overdose, injuries from battery explosions in vaping devices, and harm to various bodily systems including the gastrointestinal, renal, cardiovascular, and neurological systems.2,3
This case presents a complex medical scenario involving a previously healthy 39-year-old male with a history of vaping. He presented with a constellation of symptoms, including fever, respiratory distress, gastrointestinal symptoms, renal abnormalities, and electrolyte imbalances being a multisystemic disease. The initial assessment revealed hypoxia and metabolic acidosis, prompting further investigation. Ultimately, a diagnosis of organizing pneumonia type with eosinophils was made. Surprisingly, despite his young age and absence of known cardiovascular risk factors, he also experienced a myocardial infarction and acute kidney injury associated with this condition.
One notable aspect of this case is the connection between vaping and the patient’s presentation. Following the criteria proposed in 2020 after the Wisconsin crisis to determine if a patient has EVALI, several factors are required: a history of ECIG use within the last 90 days, lung opacities on chest radiograph or computed tomography, exclusion of lung infection based on negative results from tests such as influenza PCR or rapid test (unless out of season), respiratory viral panel, negative testing for clinically respiratory infections (urine antigen test for Legionella and Streptococcus pneumoniae, blood cultures, sputum cultures if producing sputum, and BAL if performed), negative testing for HIV-related opportunistic respiratory infections, along with the absence of a plausible alternative diagnosis (cardiac, neoplastic, rheumatologic). 9 In this case, the patient’s history of vaping raises suspicion for vaping-associated lung injury as a potential underlying cause of his symptoms, particularly given that all the before mentioned criteria were met, confirming the diagnosis of EVALI.
Regarding the clinical presentation of EVALI, respiratory symptoms arise due to direct chemical injury from ECIG aerosols containing substances like propylene glycol, glycerin, nicotine, or THC, leading to necrosis of epithelial and endothelial cells. 11 Additionally, flavorings can disrupt the integrity of the alveolar squamous epithelium, alter microbial clearance in the respiratory tract, reduce mucus clearance, and impair the phagocytic activity of alveolar macrophages and polymorphonuclear cells, thereby triggering an inflammatory response that eventually culminates in lung injury. 2 Clinically, this presents as chronic cough, bronchitis, decreased forced expiratory volume in one second (FEV-1), and wheezing with oral breathing. In acute episodes, dyspnea and desaturation may also occur, depending on the severity of involvement. 12 Comparing what is described in the literature, our patient presented all the manifestations, including hypoxemia and oxygenation disorder in ABG.
Gastrointestinal manifestations such as abdominal pain, nausea, and vomiting are present in 73% of cases, regardless of the severity of the condition. 2 Depending on the severity of EVALI, along with gastrointestinal symptoms, renal injury and electrolyte disturbances may occur,3,13 as was the case with the patient who presented acute kidney injury, metabolic acidosis, and hyperkalemia. In terms of evidence, nicotine solvents propylene glycol and glycerol used to create theatrical fog and smoke are metabolized through the methylglyoxal pathway which ends up in the production of D-lactate; however, after high-dose (8 g/kg), long-term (22 days) inhalation, they can result in D-lactic acidosis and nephrotoxicity.3,13 The patient in this case had been vaping daily for 5 years, thus explaining the presence of these manifestations.
A remarkable detail in this case was the involvement of the cardiovascular system. Despite being a young patient without known cardiovascular risk factors, he revealed a complex cardiovascular condition during hospitalization, necessitating prompt and targeted management strategies. Emerging evidence suggests that ECIGs have also cardiovascular risks and effects.3,14 Cardiovascular effects linked with nicotine arise from its sympathomimetic properties. Nicotine triggers the release of catecholamines by the sympathetic nervous system, activating β-adrenergic receptors in the heart. This activation leads to elevated heart rate, increased cardiac contractility (inotropy), and heightened workload. Prolonged stimulation of the sympathetic nervous system induces cardiac remodeling, which fosters heart failure development, heightens arrhythmia occurrence, potentially causing vasospasm, resulting in ischemia, and sudden death.3,14 Besides nicotine, other constituents in vape products can also induce cardiovascular effects. 15 These components contribute to increased oxidative stress and inflammation, causing endothelial damage, platelet activation, and lipid oxidation. This cascade raises the risk of inflammatory atherosclerosis and ischemia. Additionally, non-nicotine constituents may disrupt ventricular repolarization, further elevating the risk of arrhythmias. 15 This patient developed an acute myocardial infarction due to non-nicotine products that triggered the condition.
Concerning treatment, managing this patient involved a multidisciplinary approach, encompassing ICU care, supplementary oxygen, intravenous fluid administration, antibiotic therapy, corticosteroids, and cardiac intervention. According to CDC recommendations, admission criteria include patients with potential lung injury, particularly those experiencing respiratory distress, those with comorbidities compromising pulmonary reserve, or those with decreased (<95%) oxygen saturation. 16 The need for ICU admission in our patient was determined by renal disturbances and hyperkalemia, in addition to respiratory issues.
Based on a prospective observational cohort study, antibiotic and/or antiviral treatment should also be considered in EVALI patients, as EVALI can be associated with bacterial or viral pneumonia. Initial antibiotic treatment should align with local or national antibiotic guidelines. 17 Considering steroids, this study supports a short course, starting with the equivalent of methylprednisolone 0.5 to 1 mg/kg per day and tapering over 5 to 10 days, guided by the clinical course. 17 Following these recommendations, the administered treatment led to favorable progress. The comprehensive evaluation and treatment highlight the importance of thorough assessment and collaboration among different medical specialties in managing complex cases.
Conclusion
In conclusion, this case states the critical role of patient education and counseling in addressing the risks associated with vaping. Explicit advice to discontinue vaping upon discharge emphasizes the need for healthcare providers to actively inquire about vaping history and offer appropriate guidance to patients, especially given the rising prevalence of vaping and its associated health hazards. Further research is imperative to deepen our understanding of EVALI’s pathophysiology, diagnosis, and treatment. To effectively tackle this life-threatening issue, implementing a comprehensive approach that includes product regulation, public awareness campaigns, socioeconomic interventions, and policy reforms is essential. Ultimately, recognizing that vaping carries risks and is not a safe alternative for smoking cessation is crucial in safeguarding public health.
Supplemental Material
sj-jpg-1-icr-10.1177_11795476251313766 – Supplemental material for Vaping: A Safe Alternative to Counteract Smoking? Case Report
Supplemental material, sj-jpg-1-icr-10.1177_11795476251313766 for Vaping: A Safe Alternative to Counteract Smoking? Case Report by María Cristina Martínez-Ávila, Eugenio Matijasevic Ardila, Alieth Lucía Acosta Cardozo, Cristian Camilo Alvarado Castro and Carlos Eduardo Matiz-Bueno in Clinical Medicine Insights: Case Reports
Footnotes
Acknowledgements
The authors would like to acknowledge the support of the Fundación Santa Fe de Bogotá.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
MCMA and ALAC collected the data, creation of the report and writing the manuscript. CCAC contributed to image selection. EMA clinical expertise, final approval of the version to be published. CEMB supervision, project administration, and ensuring integrity of the work throughout. All authors read and approved the final manuscript. The authors have read and confirmed the agreement with the ICMJE authorship and conflict of interest criteria.
Consent for Publication
Written informed consent for treatment and publication was provided by the patient.
Data Availability Statement
The data analyzed in this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.