
Abstract
Condyloma acuminata (CA) is a common manifestation of human papillomavirus (HPV) infection affecting the urogenital tract. While external genital lesions are frequently encountered, urethral involvement presents a therapeutic challenge due to the risk of recurrence and long-term complications such as urethral stricture. We present a case of urethral condyloma acuminata in a 43-year-old male patient who demonstrated favorable progression following electrocoagulation therapy. The patient presented with urethrorrhagia and lower urinary tract symptoms, with subsequent diagnosis confirmed via urological examination. Negative results from extensive microbiological testing supported the diagnosis. Treatment involved biopsy excision combined with electrocoagulation, resulting in complete resolution of symptoms without recurrence at 2-month follow-up. This case underscores the importance of individualized treatment strategies for intraurethral condyloma acuminata and highlights electrocoagulation therapy as a viable option with favorable outcomes.
Introduction
Condyloma acuminata (CA) are superficial epithelial papillomatous growths that mainly affect the external genitalia and the perianal area. These lesions result from a sexually transmitted infection (STI) with human papillomaviruses (HPV). 1 Urethral involvement, although more common in men, represents a major therapeutic challenge due to the prolonged healing process, the high rate of recurrence, and the risk of long-term complications, such as urethral stricture.
We present a case of condyloma acuminata of the urethra in a 43-year-old patient who demonstrated favorable progression following electrocoagulation therapy.
Case Presentation
A 43-year-old married father of two presented to the clinic with urethrorrhagia. The patient reported no risky sexual behavior or specific toxic habits. However, he was suffering from recurrent episodes of urethritis.
On general examination, the patient was afebrile, hemodynamically stable, and had normal respiratory parameters. Urological examination revealed condyloma acuminata in the urinary meatus and distal urethra (Figure 1).

Clinical examination appearance of condyloma acuminata upon admission. (A) Condyloma appearance upon visual inspection. (B) Condyloma appearance after physical examination.
Symptoms began 1 month prior to admission, with progressive urethrorrhagia after intercourse, associated with moderate lower urinary tract symptoms (LUTS) such as urinary frequency and urgency. In addition, the patient presented with flat papillary lesions on the anterior perineum.
A urethral swab to exclude potential HPV infection was not performed. Due to technical limitations, no PCR genotyping was conducted to analyze either high-risk or low-risk HPV genotypes. A full microbiological evaluation of various STI was carried out. For this evaluation, we performed a urine culture using the first-catch urine sample to diagnose Ureaplasma sp., Mycoplasma hominis, Trichomonas vaginalis, and Neisseria gonorrhoeae. Additionally, serological testing was conducted for Chlamydia trachomatis. All results from these tests were negative. Rapid tests for HIV, HBsAg, anti-HBV antibodies, anti-HCV antibodies and the hemagglutination test for Treponema pallidum were also negative. No inflammatory cells were found in the urine sediment, leading to the diagnosis of intra-urethral condyloma acuminata.
Following a thorough intraoperative examination of the lesions (Figure 2), the patient underwent biopsy excision combined with electrocoagulation using an electric loop under locoregional anesthesia (Figure 3). Subsequent cystoscopy revealed no other associated lesions.
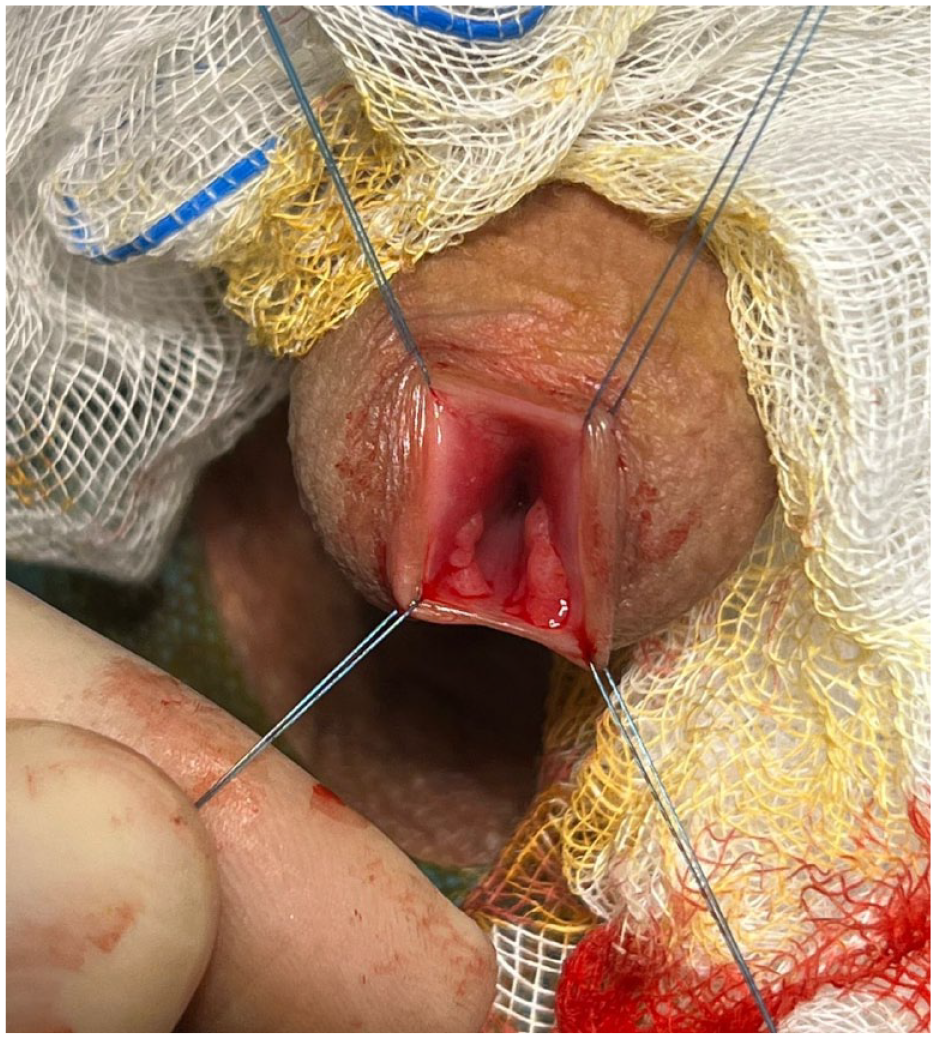
Preoperative appearance of lesions in the distal urethra.

Urethral mucosa after electrocoagulation.
The patient’s clinical course was favorable in the days following the operation, with the disappearance of the urethral lesions as well as urethrorrhagia and LUTS. Examination of the urethra 2 months after the operation showed no recurrence or narrowing. In addition, a gynecological assessment of the partner was recommended.
Discussion
Condyloma acuminata represent one of the most common STI, with a higher incidence among individuals aged 18 to 26.2,3 Among the various human papillomaviruses, subtypes HPV 6 and 11 are the primary causes of condyloma in the urogenital tract. 4 Urethral involvement occurs retrogradely, explaining the prevalence of distal locations, situated about 2 cm from the urethral meatus, as common sites for wart development. However, in rare cases, the proximal urethra and bladder may also be affected; this manifestation is consistently associated with immunodeficiency, 5 as demonstrated by the case reported by Sarier et al., 6 describing a 30-year-old patient who developed condyloma acuminata 12 months after a living-donor renal transplantation, with lesions identified in the proximal urethra and bladder. In contrast, our patient exhibited no clinical signs of immunodeficiency, was in good overall health, and tested negative for HIV, and hepatitis, which likely accounts for the exclusively distal location of the condyloma within the urethra in this case.
Transmission occurs primarily through sexual contact, with a transmission risk of approximately 6%, which increases with a higher number of sexual partners and an early onset of sexual activity. 7 Although we do not have detailed information about the patient’s sexual behavior beyond his report, the infection could be related to the sexual behavior of his partner (his wife), who was not assessed. Therefore, a gynecological assessment of the partner should always be recommended. Although HPV has carcinogenic potential and is classified based on its risk as low, intermediate, and high, subtypes 16 and 18, which are most associated with dysplasia and cancers of the cervix or penis, represent only 3% of cases of condyloma acuminata.7,8
Condyloma acuminata are generally minimally symptomatic or asymptomatic. Clinical manifestations appear in only 1% of virus carriers. The primary manifestations are visible growths, which can be papillary or pedunculated, reddish-brown in color and vary significantly in number and size.1,9 Depending on their size and anatomical location, they can be painful or pruritic, cause burning sensations, irritation from clothing and occasionally bleeding. 9 In men, they frequently occur on the scrotum, under the foreskin of the uncircumcised penis, on the corona, and on the frenulum of the glans, accounting for 52% of cases. The urethra is affected in 20% of cases, with the meatus alone involved in over 80% of these cases. Papillary lesions in the proximal part of the navicular fossa are present in approximately 5% of cases.3,10 -12 Additionally, urinary symptoms may be observed, such as increased frequency of urination, dysuria, spontaneous or irritation-induced urethrorrhagia, deviation of the urinary stream, and acute urinary retention. 13
During the physical examination, CA can be observed with the naked eye or using tools such as a speculum adapted to visualize the urethral meatus and navicular fossa. 3 For a complete exploration of the urethra, urethro-cystoscopy is recommended, as it allows not only a detailed diagnosis of lesions, including their number and location, but also the performance of biopsies and therapeutic procedures. 3 Local application of 5-aminolevulinic acid (ALA) can improve the detection of subclinical lesions. 14 It is generally advisable to treat external and distal lesions first, before proceeding with endoscopic exploration. However, if there are features suspicious of malignancy—such as irregular pigmentation, ulceration, or bleeding—or if the lesions affect more internal areas such as the proximal urethra or bladder, a thorough pathological examination becomes crucial.15,16 This is particularly important in cases where there is urethral bleeding or other concerning symptoms, as they may warrant further investigation to rule out malignancies such as urethral carcinoma, which, although rare, can present with symptoms like hematuria or urethrorrhagia. Despite the association of low-risk HPV types (eg, HPV 6 and 11) with benign lesions, high-risk HPV types (eg, HPV 16 and 18) are more commonly linked to cancers in these areas. Therefore, a pathological examination is essential to guide a specific approach and ensure appropriate management.
In terms of treatment, current guidelines do not define a specific approach. The aim is to heal the lesions while reducing the risk of recurrence and urethral stricture. A number of treatment options are available: topical medication, photodynamic therapy with delta aminolevulinic acid (ALA-PDT), 1 simple excision using scissors or sharp curettes, electric loop ablation and endoscopic ablation (laser or cryotherapy). 17 Each doctor must develop a treatment plan based on their expertise and the available modalities. While initial assessments after 4 to 8 weeks are advisable, 15 HPV’s ability to persist in basal keratinocytes and reactivate later necessitates long-term follow-up. Although there is no consensus on specific follow-up protocols for urethral condyloma, regular monitoring is essential due to the chronic nature of the infection and the ongoing risk of recurrence.
Prevention is based on widespread vaccination against subtypes 6, 11, 16 and 18, targeting mainly young individuals aged between 12 and 17, and ideally administered before the start of any sexual activity. The vaccination is recommended for both sexes. 18 It is crucial to note that the best protection is obtained by reducing the number of sexual partners and combining vaccination with the use of condoms. 19
Our case presents some limitations, Due to technical limitations, we were unable to perform PCR genotyping to assess the risk associated with HPV serotypes in the presented case. PCR testing would have allowed for a more precise analysis of HPV genotypes, particularly to identify high-risk serotypes that could influence patient management and disease prognosis. This restriction limits our ability to fully assess associated risks and tailor treatment accordingly. We acknowledge that the absence of this test is a significant limitation and note that it may impact the interpretation of results and the management of condyloma acuminata.
Conclusion
Intraurethral condyloma acuminata represent a clinical and therapeutic challenge due to their rarity and high potential for recurrence. Treatment options require an individualized approach, taking into account the location and extent of the lesions as well as the patient’s preferences. Regular monitoring and adjustments are essential to optimize healing and reduce the risk of recurrence.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Abbreviations
CA: Condyloma Acuminata
LUTS: Lower Urinary Tract Symptoms
STI: Sexually Transmitted Infections
ALA-PDT: Delta Aminolevulinic Acid
HPV: Human Papillomaviruses
Author Contributions
Ghassane El Omri and Hamza Rais contributed to the patient’s care, conducted the bibliographic research, and wrote the paper. Anas Taghouan and Moussaab Rachid contributed to the development of the study design. Younes Houry and Abdeljalil Heddat reviewed and approved the final manuscript and participated in its validation process.
Availability of Data and Material
On request, email the corresponding author.
Ethical Approval
Not applicable.
Code Availability
Not applicable.
Consent to Participate
Written and informed consent taken.
Consent for Publication
Written and informed consent taken.