
Abstract
Introduction:
A spot sign on computed tomography angiography (CTA) scan is a widely recognized radiographic indicator of primary intracerebral hemorrhage (ICH) used to predict early hematoma expansion. Nonetheless, recent multicenter studies have indicated that its predictive value for hematoma expansion is not as significant as previously stated. Therefore, identifying the reasons for the poor performance of these studies is imperative.
Case presentation:
A 48-year-old man presented with a 9-hour history of alalia and right limb hemiplegia. Noncontrast computed tomography (CT) revealed a hematoma in the left frontal lobe, while CTA showed a spot sign within the hematoma, leading to a diagnosis of frontal lobe hemorrhage. During the surgical procedure, a blood clot was removed, revealing the presence of 3 mm of saccular tissue resembling an aneurysm. The process of exposing its complete form resulted in its rupture and bleeding. The location of this tissue at the top of the hematoma cavity corresponded to the CTA spot sign. Pathological examination confirmed that the characteristics of the tissue wall were consistent with those of a pseudoaneurysm.
Conclusion:
This case suggests that more stringent identification criteria should be established in studies predicting ICH expansion using the spot sign on CTA to differentiate and exclude pseudoaneurysms, thereby improving the accuracy of predicting early hematoma expansion using the CTA spot sign.
Introduction
Hematoma expansion following intracerebral hemorrhage (ICH) is a commonly observed phenomenon, even in patients with normal coagulation function, and hematoma expansion is a risk factor for poor outcomes following ICH. 1 The computed tomography angiography (CTA) spot sign refers one or more foci of contrast enhancement within an acute primary parenchymal hematoma visible on the source images of CTA. 2 This sign has been used to screen for patients at risk of hematoma expansion. 2 However, in recent multicenter studies, its performance in predicting hematoma expansion was worse than that reported in earlier studies. 3 Furthermore, there was no evidence that intensive blood pressure reduction or tranexamic acid treatment could prevent ICH growth and thereby improve clinical outcome in patients with spot signs.3,4 The poor performance of these studies may be due to falsely identified spot signs. The development of more advanced recognition criteria may improve identification and thus performance in similar future studies. Here, we report novel intraoperative and pathological findings related to CTA spot signs in a patient with ICH.
Case Presentation
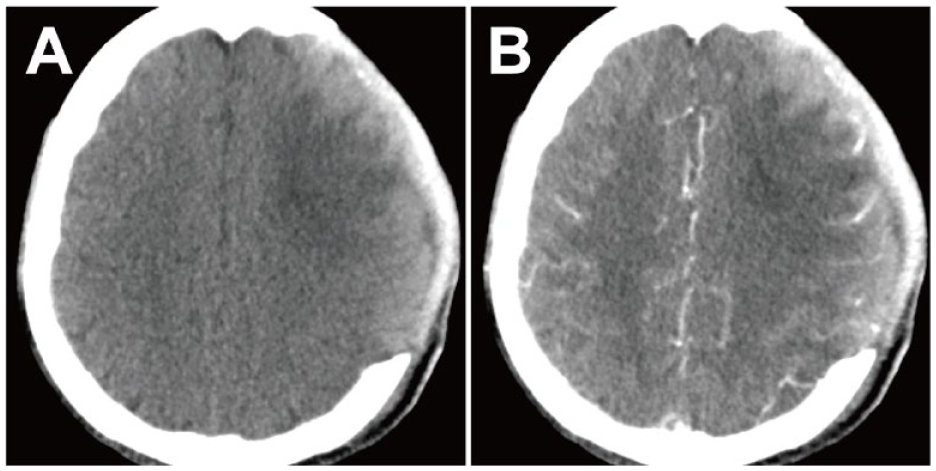
A 48-year-old man presented with a 9-hour history of alalia and right limb hemiplegia. The patient denied a history of hypertension, denied any use of anticoagulant or antiplatelet medications, and denied a history of trauma. Noncontrast computed tomography (CT) showed a 50 mL hematoma in the left frontal lobe, temporal lobe, and basal ganglia without hyperdensity (except for calcium analogs) (Figure 1A and B), while CTA axial source images and coronal and sagittal multi-planar reconstruction images showed a spot suspended in the frontal lobe hematoma without vascular connection to the surrounding structures or with a density greater than 120 Hounsfield units (Figure 1C-E). No aneurysms affecting the left cerebral arteries or their branches were observed on CTA 3-dimensional reconstruction (Figure 1F). The spot sign was ascertained according to the definition cited above 2 in the introduction. Emergency evacuation of the left cerebral hematoma and hemicraniectomy were performed. CTA multiplanar reconstruction was used to determine the optimal access point where the cortex was closest to the spot sign. The hematoma was found 15 mm beneath the subcortex. After evacuation of the hematoma, under an intraoperative microscope, a piece of 3 mm saccular tissue resembling an aneurysm arose from a microvessel (Figure 2A). The process of exposing its complete form resulted in its rupture and bleeding (Figure 2B). It was located at the top of the hematoma cavity, consistent with the location of the CTA spot sign. The microvessels were coagulated using bipolar forceps. The aneurysm-like tissue was removed from the arteriolar defect and sent for further pathological diagnosis. Hematoxylin-eosin (HE) staining demonstrated that the wall of the aneurysm-like tissue was composed of organized thrombi and fibrosis, as well as chronic inflammatory cell infiltration, but lacked the intima, internal elastic laminae, and adventitia (Figure 2C and D). Therefore, we concluded that the spot sign identified via preoperative CTA should indicate a pseudoaneurysm. At the 19-day follow-up examination, postoperative CTA confirmed that the hematoma had been thoroughly evacuated, and there was no sign of a CTA spot sign (Figure 3A and B).

(A, B) Noncontrast head computed tomography(CT) shows hematoma in the left frontal lobe, temporal lobe, and basal ganglia. (C-E) CTA axial source images and coronal and sagittal MPR images show spot sign (yellow arrow) in hematoma before surgery. (F) No intracranial vascular aneurysm were observed on the CTA.
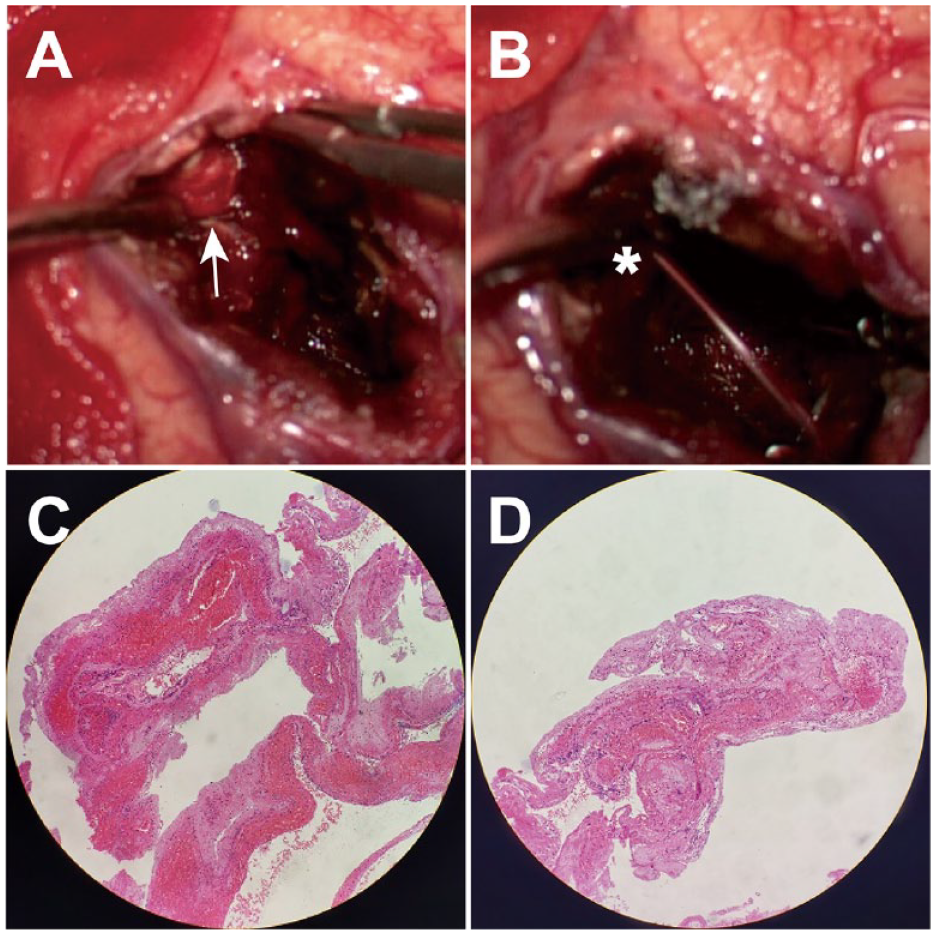
(A, B) Intraoperative microscopic images revealed the presence of a 3 mm-sized saccular tissue (white arrow) resembling an aneurysm at the superior aspect of the hematoma cavity; its complete exposure led to the rupture and active hemorrhage (white asterisk). (C, D) The HE stain demonstrated that the wall of the aneurysm-like tissue was composed of organized thrombosis and fibrosis, as well as chronic inflammatory cell infiltration, but without intima, internal elastic laminae, or adventitia.
(A, B) The NCCT and CTA axial source images revealed a successful and thorough evacuation of the hematoma, with no evidence of the CTA spot sign.
Discussion
In 1997, Brott et al. defined hematoma expansion as “an increase in hematoma volume of more than 33% as observed on head CT scans,” a definition that has been widely adopted as the universal standard for assessing hematoma expansion. 5 In recent years, researchers have reported that hematoma expansion affects 1 of 5 patients within 24 hours of the onset of acute ICH and is associated with increased risks of mortality and disability, making it an attractive therapeutic target.6,7 The CTA spot sign is considered a promising radiological marker for the prediction of hematoma expansion, but its pathology and exact relationship with hematomas remain unclear. 8 Through autopsy, Fisher discovered fibrin globes up to 5 mm in diameter adjacent to an arteriolar defect, which were composed of external fibrin strands and internal platelet mass filling. 9 According to the description, some scholars have postulated that the fibrin globe might be the pathological feature of the CTA spot sign. 9 However, in our patient, the spot sign identified via preoperative CTA was actually a pseudoaneurysm arising from an unrecognizable vessel. Just as Fisher believed that the appearance of the fibrin globe indicated the cessation of bleeding, 9 the pseudoaneurysm might also mark the temporary cessation of bleeding. It is therefore reasonable to recognize that a pseudoaneurysm might be an early stage or intravital manifestation of the fibrin globe, and hence an early manifestation of bleeding cessation. Although this hypothesis has yet to be proven, our case study explored the possible underlying pathology of the spot sign, which could contribute to its novel recognition.
The CTA spot sign is recommended as an inclusion criterion for patient selection in clinical trials of acute hemostatic therapy or surgical intervention to minimize hematoma expansion. However, in recent multicenter clinical studies, the spot sign performed poorly in predicting hematoma expansion, and interventions did not achieve the desired clinical prognosis.3,4 The CTA features of pseudoaneurysms include punctate enhancement connected to the vessel. However, the pseudoaneurysm in this patient, which was mistakenly identified as a spot sign, may have been undiagnosed on preoperative CTA due to reasons such as the supplying artery being relatively small, vascular spasm, or compression by hematoma (Figure 1C-F). This provides a reasonable explanation for the lower accuracy of CTA spot sign in predicting hematoma expansion. The true CTA spot sign is generally believed to represent the site of vessel rupture and thus active hemorrhage. Since the development of a pseudoaneurysm most likely represents hemostasis, this could interfere with the judgment and lead to misidentification of the spot sign. Novel radiological criteria must be established for accurate identification of active contrast extravasation. The true characteristic of CTA spot sign is the slow and persistent extravasation of contrast agent, which is not observed in pseudoaneurysms following hemostasis after ICH. Therefore, true CTA spot sign will demonstrate volume changes on delayed scans, whereas pseudoaneurysms formed due to hemostasis will not. The utilization of dynamic contrast-enhanced CTA facilitates the differentiation between spot sign and pseudoaneurysms. 10 Our report of this case acknowledges certain limitations. For instance, the results of these studies must be interpreted with caution as they present a scenario in which the spot sign is indicative of an earlier stage of hemorrhage cessation.
Conclusion
The CTA spot sign is considered a promising radiological marker for predicting hematoma expansion, but its exact pathological significance and relationship with the hematoma are still unclear. This is the first case of ICH presenting as a spot sign, confirmed by intraoperative and pathological examination as a pseudoaneurysm. This provides a reasonable explanation for the suboptimal results of clinical trials in which the spot sign was used to predict hematoma expansion, as the formation of pseudoaneurysms may represent hemostasis while the true spot sign may indicate active bleeding. This case suggests that more stringent identification criteria should be established in studies predicting ICH expansion using the spot sign on CTA to differentiate and exclude pseudoaneurysms, thereby improving the accuracy of predicting early hematoma expansion using the CTA spot sign.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Chongqing Science-health joint medical research project (Grant No. 2023MSXM102 to YN), Heilongjiang Provincial Health Commission scientific research project (Grant No. 20230404040027 to QZ), and the 961st Hospital medical scientific research project (Grant No. ZZKY2023-012 to QZ).
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
YN conceived and designed the present study. QZ, ZC, YC, ZJ, WL, ZY, WF, YF, ML and YN acquired and analyzed the data. QZ and YN drafted the manuscript. All authors read and approved the present version of the manuscript to be published.
Consent to Participate
Written informed consent was obtained from the patient for his participation in this case report. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Consent for Publication
Consents were obtained for publication from the patients upon stabilization of their psychotic illnesses.