
Abstract
Dopamine agonists are the first-line treatment of prolactinomas. The risk of developing de novo psychiatric symptoms during dopamine agonist therapy is low. Herein, we report the case of a 42-year-old woman with a giant prolactinoma who developed a psychiatric disorder after 1 day of cabergoline therapy initiation. She presented with amenorrhea, galactorrhea, headaches, and disturbed vision. Biological investigations revealed hyperprolactinemia (2975 ng/ml) with gonadotropin deficiency. Pituitary MRI showed a giant pituitary adenoma. The patient was treated with cabergoline at the dose of 1 mg twice weekly. One day after the treatment initiation, she developed acute delirium with temporospatial disorientation and compulsive medication use. These symptoms disappeared 1 week after the reduction of the dose of cabergoline. Patients with hyperprolactinemia receiving an initial high dose of cabergoline may develop changes in mood and behavior regardless of prior psychiatric history.
Introduction
Prolactinoma represents the most common tumor of the pituitary gland, accounting for 40% of pituitary adenomas. It’s classified according to the tumor size as microprolactinoma (<10 mm) and macroprolactinoma (⩾10 mm). Although microprolactinoma is more frequent in women, macroprolactinoma occurs more frequently in men. Giant prolactinoma, defined as an adenoma with a maximum diameter of more than 4 cm that is associated with serum prolactin above 1000 ng/mL, is rare, representing 0.5% of all pituitary tumors and 4% of all prolactinomas.1-3 It’s more frequent in men with a median age at diagnosis of 42 years. 4 Only 10% of giant prolactinomas occur in women with a median age at diagnosis of 44 years. 5
The first-line treatment of prolactinoma is dopamine agonists that lower prolactin levels, decrease tumor size, and restore gonadal function. 6 Bromocriptine and cabergoline are the most frequently prescribed drugs. 7
Psychological disorders may be expected in patients with prolactinoma. 8 Indeed, these patients may have a poor quality of life, anxiety, depression, and certain personality traits. Recently, an increasing number of reports emphasized dopamine agonists’ psychological side effects. Some patients developed de novo psychiatric symptoms; others had an exacerbation of preexisting conditions during dopamine agonist therapy. 6
Herein, we report the case of a woman with a giant prolactinoma who developed psychiatric disorders after 1 day of cabergoline therapy initiation.
Case Presentation
A 42-year-old woman was referred to our department for pituitary apoplexy. Her past medical history included type 2 diabetes mellitus treated with metformin. No personnel or family history of psychiatric disorders was reported. She was not taking any other drugs. The patient was unmarried and unemployed.
The patient presented with a headache associated with visual blurring, secondary amenorrhea, and galactorrhea.
On physical examination, she had a body weight of 75 kg, a body height of 1.65 m corresponding to a body mass index of 27.5 kg/m2, a blood pressure of 120/70 mmHg without orthostatic hypotension, a heart rate of 66 beats/min, and a normal sized thyroid gland. Hydration, cardiovascular, pulmonary, abdominal, and neurological examinations were normal. There was no dysmorphic syndrome or other features of acromegaly.
Biological investigations showed hyperprolactinemia and hypogonadotropic hypogonadism (Table 1).
Serum biological and hormonal parameters.

Two-day, 2 mg test.
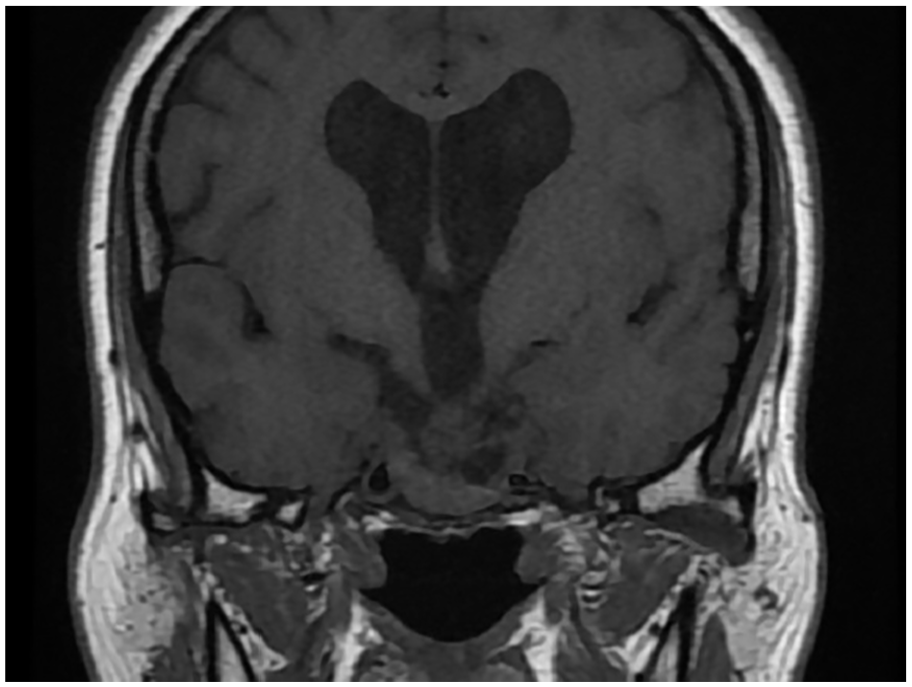
The pituitary magnetic resonance imaging (MRI) showed a giant pituitary adenoma measuring 57 × 41 × 42 mm extending to the cavernous and sphenoid sinuses, compressing the optic chiasma, and complicated by apoplexy and hydrocephalus (Figure 1). The ophthalmologic examination revealed a right papilledema stage 2 with absolute scotoma and left optic atrophy.

Pituitary MRI showing a giant macroadenoma before treatment.
The patient was treated with cabergoline 1 mg twice weekly. One day after treatment initiation, the patient developed acute delirium with temporospatial disorientation and compulsive medication use. Physical examination, blood glucose, calcium and sodium levels, and electrocardiogram were normal. The patient was immediately examined by a psychiatrist. After ruling out organic causes, acute confusion and impulsive control disorder due to the use of cabergoline were assessed. No psychiatric treatment was needed. The patient had only a close follow-up. The dose of cabergoline was reduced to 0.5 mg twice weekly. The patient’s psychiatric symptoms disappeared after 1 week. Three months later, her prolactin level was normal and tumor size was reduced to 40 × 20 × 29 mm (Figure 2) with visual field improvement.
Pituitary MRI showing tumor shrinkage 3 months after treatment.
Discussion
We report the case of a woman with a giant prolactinoma complicated by apoplexy and hydrocephalus and who developed de novo psychiatric disorders immediately after cabergoline initiation.
Dopamine is an essential nervous system transmitter for many cerebral functions such as the control of motor function, motivation, and learning. 9 In the central nervous system, dopaminergic pathways include the nigrostriatal pathway involved in the regulation of locomotion and movement, the mesocorticolimbic pathway involved in the regulation of emotional states (behavior, pleasure, and addiction), and the tubero-infundibular pathway involved in the control of pituitary activities. 10 Dopamine represents the major prolactin inhibiting factor. Dopamine agonists are used in the treatment of prolactinomas. In patients with giant prolactinoma, medical treatment with dopamine agonists represents the first-line therapeutic option even in case of visual defects. 11 It is associated with a rapid and remarkable reduction of tumor size, with a possible significant visual improvement within a short period. 11 Cabergoline was reported to have excellent efficacy and tolerability in the management of giant prolactinoma. According to Espinosa et al, 12 cabergoline treatment resulted in the normalization of prolactin levels in 68% and in a reduction of >50% in tumor volume in 87% of patients with giant prolactinoma. A rapid dose escalation may be associated with the risk of apoplexy or cerebrospinal fluid leak. The recommended initial dose of cabergoline is 0.5 to 1 mg per week. 13 In the study of Verhelst et al, 14 including 455 patients with hyperprolactinemia, the median starting dose of cabergoline was 1 mg/week in 2 gifts (Q1-Q3: 0.5-1.5 mg/week). In the case of giant prolactinoma reported by Casulari et al, 15 the starting dose of cabergoline was 1.5 mg/week. In our patient, a high starting dose was prescribed in order to obtain a rapid relief of compression of adjacent structures, particularly the optic chiasm.
Our patient had no history of psychiatric disorders before the initiation of cabergoline. She developed acute psychiatric symptoms immediately after drug intake with no other evident cause. Thus, her psychiatric symptoms can be attributed to the use of cabergoline.
The association of hyperprolactinemia and psychiatric disorders was described in the literature. In fact, elevated prolactin levels were observed in patients with a first episode of psychosis, who did not receive any antipsychotic drugs. 16 Oliveira et al, 17 in a study including 32 patients with hyperprolactinemia and 15 subjects with normal prolactin levels, demonstrated that hyperprolactinemia was associated with an increased risk of 3.52 for depression, 3.32 for anxiety, and 3.84 for other psychiatric symptoms. In a study conducted in a non-psychiatric population, Henry and Sherwin 18 suggested that increased serum prolactin levels may have negative effects on cognition. Inversely, psychiatric disorders may be caused or exacerbated by dopamine agonists prescribed in patients with hyperprolactinemia. 6 The most frequent side effects of dopamine agonists are gastrointestinal symptoms, dizziness, headaches, and orthostatic arterial hypotension. 19 Psychiatric side effects were also reported. Their incidence is estimated to be between less than 1% and 3%. 20 These side effects were described as isolated case reports or case series.21,22 They include impulse control disorders and behavioral disorders ranging from mood swings and irritability to psychotic, manic symptoms and paranoid delusions. 1 Impulsive control disorders are a heterogeneous and multifactorial group of diseases including hypersexuality, compulsive shopping, compulsive medication use as in our patient, binge eating, and pathological gambling. 6 They are well-known side effects of dopamine agonists. Their prevalence ranges from 2.6% to 34.8% in patients with Parkinson’s disease who were on dopamine replacement therapy.23,24 In patients with pituitary adenoma treated with dopamine agonists, impulsive control disorders were observed in 10% of cases. 25 In another study including 77 patients with prolactinomas and ongoing or past use of dopamine agonists, the prevalence of impulsive control disorders was about 25%. 26
Psychiatric disorders induced by cabergoline intake were stated to be more frequent in patients with a personal or family history of psychiatric illness.22,27 Our patient had no history of psychosis or mood disturbances. Other factors were reported to enhance psychiatric disorders in patients receiving dopamine agonists such as high doses, long duration of treatment, extended form, male gender, younger age (less than 65 years), being unmarried, and other associated comorbidities such as preexisting psychiatric pathology, sleep disorders, and personality disorders.28-30 Other factors related to the underlying disease were also identified, such as a younger age at the onset and a longer duration of the disease. 29
Psychiatric disorders are mainly related to dysregulation of frontostriatal and thalamic circuits. 17 The psychotic symptoms result from increased transmission of dopamine, or hyperdopaminergia in the mesolimbic pathway, which involves primarily the ventral striatum and other limbic structures. 31 This side effect usually appears early during the first year of therapy with cabergoline. 15 Our patient developed psychosis only 1 day after the initiation of cabergoline.
Due to the lack of large longitudinal prospective studies, definitive guidelines for the treatment and follow-up of dopamine agonists’ psychiatric side effects are waiting. In terms of management options, studies have suggested the withdrawal of dopamine agonists and/or the addition of clozapine in a patient with psychosis because of its minor effect on prolactin and prolactinoma growth. 21 Sohtaoglu et al 32 showed a recovery from compulsive behavior after reducing the dose of dopamine agonists in 16 patients out of 22. After reducing the cabergoline dose, our patient did not develop any psychiatric disorders again.
Conclusion
Patients with hyperprolactinemia receiving an initial high dose of cabergoline may develop changes in mood and behavior regardless of prior psychiatric history. Physicians prescribing dopamine agonists should be aware of the possible occurrence of psychiatric disorders. Larger prospective controlled clinical studies are needed to determine the prevalence of these psychiatric complications and to assess the appropriate management.
Footnotes
Acknowledgements
None.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
IO: conception and design, acquisition and interpretation of data, manuscript creation and drafting; CBS: manuscript creation and drafting, MC: Critically revision of the article for important intellectual content; all authors were involved in the management of this patient and the revision of the manuscript, and approved the final version.
Consent Statement
A written informed consent was obtained from the patient for the publication of this report.
Data Sharing Not Applicable
No new data generated.
Ethics Statement
Ethical approval for this case report was not required.