
Abstract
Granulomatosis with polyangiitis is a rare autoimmune disease that affects small to medium-sized blood vessels throughout the body. Here, we present a case of an infratemporal mass that was the result of granulomatosis with polyangiitis. A 51-year-old male presented to the emergency department due to right cheek and facial pain that he had been experiencing for 2 to 3 months. An MRI revealed a mass within the right infratemporal and pterygopalatine fossae extending into the inferior right orbital fissure along the maxillary division of the trigeminal nerve (V2) and the vidian nerve causing concern for malignancy. Histology from an endoscopic biopsy demonstrated multiple arteries with luminal obliteration with non-necrotizing granulomas. The patient was started on steroids and immunosuppressive therapy, which improved his symptoms and decreased the size of the residual mass. This case illustrates the need for laboratory testing, imaging, and biopsy of the involved tissue in cases where GPA is suspected to prevent treatment delays that could lead to the destruction of vital organs.
Introduction
Vasculitides occur when inflammatory leukocytes damage the blood vessel lumen leading to bleeding and tissue necrosis. This condition is categorized according to the size of the blood vessel that is affected (ie, large, medium, and small). Granulomatosis with polyangiitis (GPA) vasculitis predominately affects small- to medium-sized vessels. It commonly affects the kidneys resulting in glomerulonephritis and inflammation in the upper and lower respiratory track. 1
GPA is commonly diagnosed in individuals in their fifties and sixties, although it can be diagnosed at any age. 2 Additionally, males and females are equally affected. It occurs more frequently in people of European ancestry, with Caucasians generally having a higher incidence of GPA. 3 The initial presentation is frequently malaise and fevers, which makes for a difficult diagnosis and can lead to disease progression and life-threatening complications. Twenty percent of patients die within the first year of being diagnosed with GPA. 4 Among survivors, 20% require dialysis for end stage renal disease.4,5 Here, we report a rare case of ANCA-negative GPA involving the infratemporal and pterygopalatine fossae.
Case Presentation
A 51-year-old male presented to the emergency department with pain and facial swelling in the right cheek, which had been ongoing for 2 to 3 months. In the emergency department, a computerized tomography (CT) scan showed inflammation in the right maxillary sinus with mucosal thickening. A complete blood count (CBC) with differential and comprehensive metabolic panel (CMP) were both within normal limits. He was started on a 10 days course of oral antibiotics and fluticasone nasal spray.
Nine days later the patient presented to his primary care physician with concern for worsening right facial swelling, despite being on an antibiotic, and represented to the emergency department. The patient was started on vancomycin, piperacillin/tazobactam, and dexamethasone. A magnetic resonance image (MRI) of the brain was obtained and revealed a mass within the right infratemporal and pterygopalatine fossae extending into the inferior right orbital fissure along V2 and the vidian nerve, causing concern for potential malignancy (Figures 1 and 2).

Coronal images from MRI of the brain of a 51-year-old male patient presenting with pain and facial swelling of the right cheek. (A-D) The MRI was obtained using the trigeminal nerve (CN V) protocol with/without contrast. The T1-weighted magnetization-prepared 180° radio-frequency pulses and rapid gradient-echo (MP RAGE) sequence was obtained prior to biopsy. Coronal images from anterior (left, (A)) to posterior (right, (D)) demonstrate an enhanced infiltrative soft tissue mass (black arrows) centered in the right pterygopalatine fossa/retroantral fat extending into the right orbit/superior orbital fissure, right posterolateral nasopharynx and along the right maxillary branch of the trigeminal nerve and vidian nerves as well as the right masticator space. There is no definite intracranial extension. There is minimal involvement of the posterior right maxillary sinus.

Axial images from an MRI of the brain of a 51-year-old male patient presenting with pain and facial swelling of the right cheek. (A and B) The MRI was obtained using the trigeminal nerve (CN V) protocol with/without contrast. The T1-weighted magnetization-prepared 180° radio-frequency pulses and rapid gradient-echo (MP RAGE) sequence was obtained prior to biopsy. (A) Axial image showing enhanced soft tissue filling and expansion of the right pterygopalatine fossa extending into the right nasopharyngeal/parapharyngeal and masticator spaces (orange circle). (B) Secondary extension of the soft tissue mass along the lateral right orbital wall measuring 0.5 × 1.9 cm deep to the lateral rectus muscle (white lines).
He was transferred to a tertiary care center for evaluation and management. On physical examination showed diminished sensation at the right maxillary division of the trigeminal nerve (V2) but no double vision. His right face was swollen but not fluctant and he had trismus. The patient was taken to the operating room for biopsy. The sinonasal mucosal surface all appeared normal. The posterior wall of the maxillary sinus was removed to allow access to the mass, the internal maxillary artery appeared necrotic. Histological assessment demonstrated multiple arteries with partial to complete luminal obliteration associated with loosely formed non-necrotizing granulomas, consistent with granulomatous vasculitis (Figure 3). Serum studies were positive for antinuclear antibodies (ANAs) but were negative for anti-neutrophil cytoplasmic antibodies (ANCA).
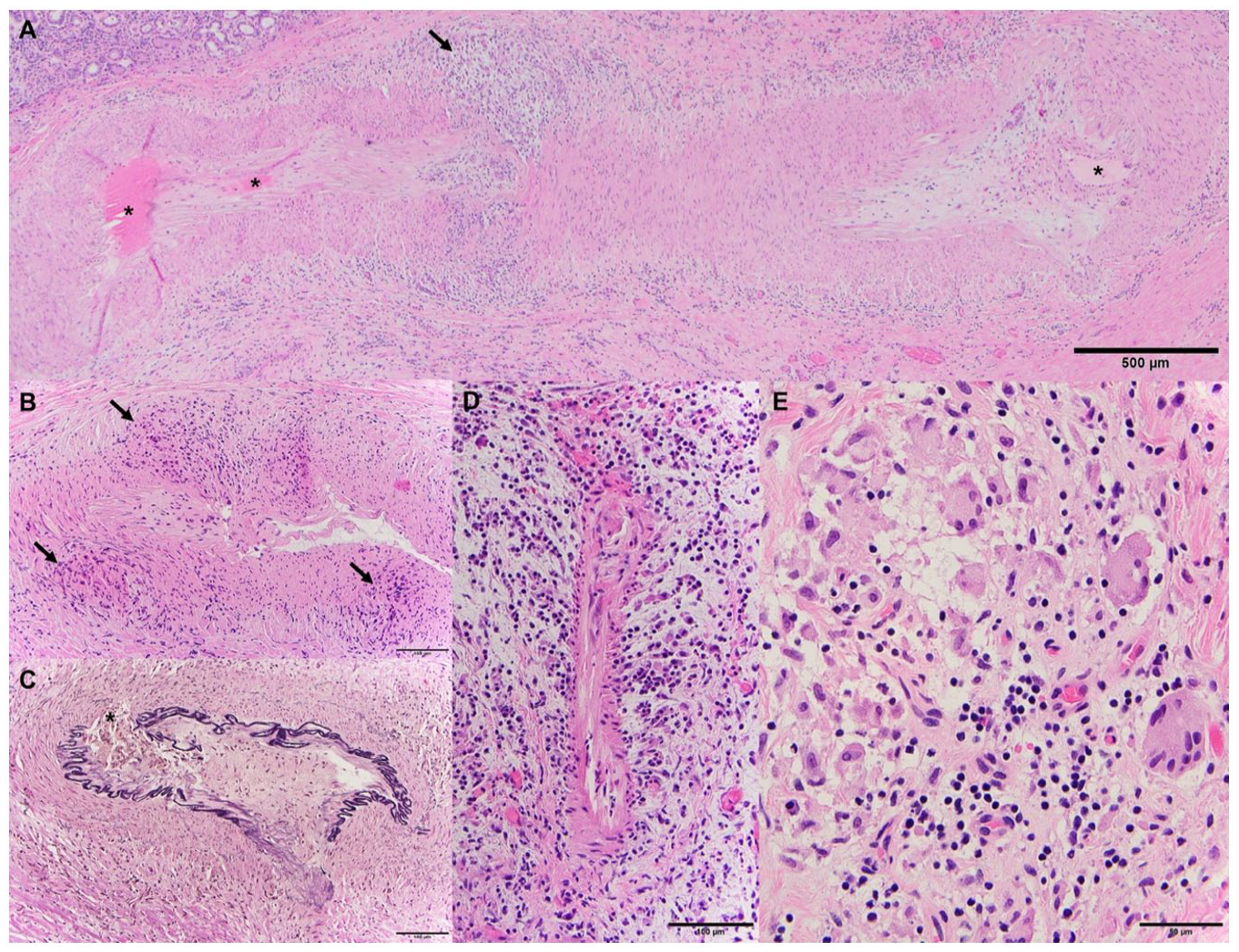
Histological analysis of intraoperative biopsy tissues of a 51-year-old male patient presenting with pain and facial swelling of the right cheek. (A-E). (A) The tortuous profile of a large sphenopalatine artery branch shows varying degrees of luminal obliteration (asterisk), fibrointimal edema, and focal transmural inflammation (arrow). (B) A different artery shows architectural irregularities due to granulomatous inflammatory infiltrates (arrows). (C) Elastin stain demonstrates focal obliteration of the elastic layer (asterisk). (D) Acute neutrophil-rich vasculitis of smaller vessels. (E) Poorly formed granulomas with multinucleated giant cells, lymphocytes, and edema.
The patient was evaluated by an infectious disease specialist and was negative for human immunodeficiency virus (HIV), hepatitis B and C, Mycobacterium tuberculosis, and other diverse opportunistic organisms. The patient was referred to a rheumatologist and nephrologist. Urine sediment showed 1 to 2 dysmorphic red blood cells (RBCs) per high-power field and 3 to 5 monomorphic RBCs per high-power field, concerning for renal involving vasculitis. The patient was diagnosed with ANCA-negative granulomatosis polyangiitis and was started on immunosuppressive treatment with prednisone and mycophenolate. At his 1-month follow-up with a nephrologist and otolaryngologist, the patient reported improved symptoms with decreased facial swelling, the ability to open his mouth, and improved sensation on the right side of his face. An informed written consent was obtained from the patient for publication of this case report.
Discussion
In 2010, the International Chapel Hill Consensus Conference (CHCC), which has gained widespread acceptance for defining vasculitides, renamed Wegener granulomatosis as granulomatosis with polyangiitis (GPA). GPA is defined as necrotizing granulomatous inflammation involving the upper and lower respiratory tract affecting predominately small to medium vessels. 6 The change was implemented in an effort to shift to the use of diseased-based nomenclature. 7
Patients with GPA generally present with non-specific symptoms such as fever, anorexia, weight loss, and fatigue. Thus, diagnosis is generally delayed . 2 Common otolaryngologic manifestations include sinusitis, otorrhea, and nasal crusting (Table 1). Delays in diagnosis can lead to dire consequences such as kidney failure and critical organ involvement. A survey of patients in a vasculitis patient support group in the United Kingdom revealed that approximately 22.9% experienced a delay in their diagnosis that was greater than 1 year. 8 Additionally, 80% of nonsevere GPA can evolve to glomerulonephritis and severe manifestation of the disease if left untreated. 9 Consequently, it is recommended that patients who are suspected of having GPA to receive a thorough patient history and physical followed by laboratory testing. Initial laboratory tests should include, but are not limited to, a CBC, a liver function test, an erythrocyte sedimentation rate (ESR) test, serologies for viral hepatitis, serum cryoglobulins, and urinalysis, as well as testing for serum creatine and/or C-reactive protein (CRP) levels. An ANCA test can also be administered for adults with high suspicion of vasculitides. Currently, there is no universally accepted criteria to establish a diagnosis of GPA. Histological evaluation of biopsied tissue remains the conclusive test for diagnosis. 2
Otolaryngology symptoms of granulomatosis with polyangiitis. 10

It is important to emphasize that a negative ANCA result and or negative biopsy does not exclude a diagnosis of GPA. Approximately 20% of patients with GPA have a negative test for ANCA in the serum.4,5 Published articles on GPA presenting as a skull-based mass (Table 2) demonstrate that a positive ANCA test is often used to establish the diagnosis. However, our case report shows that despite a negative ANCA test, a positive biopsy can still lead to a GPA diagnosis. This suggests that a GPA diagnosis should not be made solely on the outcome of an ANCA test, as subjective components of this immunofluorescence assay may obscure its interpretation and a positive outcome is not always associated with this condition. Interpreting indirect immunofluorescent assay, most widely used ANCA test, requires a seasoned laboratory technician to accurately read the result. Therefore, caution should be taken for both positive and negative ANCA test.
Published studies on skull base mass originating from granulomatosis with polyangiitis.

Conclusion
GPA affects small and medium arteries of the head and neck and there are limited case reports of vasculitis presenting as an infratemporal mass. Despite its rarity, upon diagnosis, referral to nephrology and/or rheumatology is recommended to rule out systemic involvement of the disease and to prevent treatment delays, which may lead to destruction of vital organs.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by NIH grants KL2TR002490 to AJK.The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors contributed to the design of the work, interpreted the data, drafted the article, and approved the final version of the manuscript.