
Abstract
The Rubinstein-Taybi Syndrome (RSTS) literature is limited about sensory integration, which is a foundational neurological function of the central nervous system that may affect the development of cognitive, social, and motor skills. The aim of this case report was to investigate the effects of Ayres Sensory Integration® (ASI) intervention on processing and integrating sensations, motor functions and parental goals of 3-year-old child with RSTS. Analysis of assessment data reviewed before and after treatment. Assessment collected by interview, Sensory Profile (SP), Sensory Processing Measure-Preschool (SPM-P) Home, Peabody Developmental Motor Scales-2 (PDMS-2), Gross Motor Function Measurement-88 (GMFM-88), and Gross Motor Function Classification System (GMFCS). Progress toward goals and objectives was measured with Goal Attainment Scale (GAS). ASI intervention was implemented 3 times per week for 8 weeks. At pre-intervention, SP and SPM-P Home revealed prominent sensory processing and integration difficulties in this case. PDMS-2 scores indicated the child was far behind his peers in fine and gross motor areas. In addition, systematic observations determined that the child’s GMFCS level was III. After 8 weeks of ASI intervention significant improvements were found in parent reports of sensory processing in the areas of vestibular, tactile, and oral functioning on the Sensory Profile. Gains in functional motor skills were found on the GMFM-88 and the GMFCS. Consistent with these results, significant gains at or above expected levels of performance were found on GAS goals which reflected the family’s main concerns for social participation, feeding, play, and movement. There are limited studies on sensory processing and integration in children with RSTS. This case report identified sensory processing and integration difficulties for the first time in a child with RSTS. Results also provide preliminary support for the positive effects of ASI intervention on sensory processing, functional motor skills, and parental goals of a child with RSTS.
Keywords
Introduction
Rubinstein-Taybi Syndrome (RSTS) is a complex neurodevelopmental disorder characterized by poor physical growth, mental retardation, microcephaly, dysmorphic facial features, broad thumbs, and big toes.1 -3 RSTS is a rare syndrome first described in 1963 by Rubinstein and Taybi. 4 RSTS is caused by a microdeletion of chromosome 16p13.3, or by a mutation in either CREB-binding protein (CBP) or E1A-binding protein (p300). 5 The incidence of RSTS is 1 in 100,000 to 125,000 live births. 6 Delays in motor development and skills, language and social functions are the most common symptoms in RSTS and present in 98.5% of children diagnosed with this disorder. Parents report behavioral problems in 25% of children which are often characterized by short attention, stubbornness, lack of persistence, and sudden mood changes.1,7,8 Studies of individuals with RSTS have shown they may experience sensory system-based difficulties such as hearing loss, and a variety of visual deficits.9 -12 In addition, challenges in social, cognitive and motor development are reported in studies on children with RSTS.13,14 Motor concerns in RSTS include low muscle tone and motor developmental delays, clumsiness, poor coordination, and insufficient postural control 15 which may be hypothesized to be related to decreased proprioceptive and/or vestibular processing.16,17 Functional limitations in children with RSTS which maybe related to these sensory and motor challenges include feeding difficulties 18 and hand skills and object manipulation difficulties.14,19 -22
Sensory integration is the process of organizing sensory inputs so that the brain produces a productive and meaningful body response and also useful perceptions, emotions, and behaviors. 20 During sensory integration, sensory information is registered, modulated, and interpreted to produce adaptive responses. 23 Difficulties in sensory processing and integration may contribute to many behavioral, emotional, and motor problems in children which interfere with daily functions and performance. 24 Although there are many classification systems that describe sensory processing and integration disorders, the most recent classification categorizes sensory integration challenges as sensory modulation (including sensory reactivity) and sensory perception-based difficulties including sensory discrimination and praxis challenges. 22 Sensory reactivity is characterized by excessive or reduced reactions to typical levels of sensation that interfere with participation in daily life and consists of 2 main subtypes: Over-responsivity (aversive and/or defensive reactions) and under-responsivity (poor registration) to sensory experiences. Sensory reactivity may cause behavioral consequences such as attention, regulation, affect and activity level challenges, and withdrawal from sensory experiences, sensory seeking, and poor self-esteem. Sensory perception is defined as difficulty identifying, discriminating, and interpreting sensation and may interfere with a child’s ability to use sensations for activities, for example such as processing visual and tactile sensations for praxis and motor skills needed to button clothes. 25 Poor postural-ocular control, difficulties in sensory discrimination and body schema, vestibular-based bilateral integration, sequencing problems, and somatodyspraxia are all considered sensory perception-related dysfunctions. Behavioral consequences of poor sensory processing and integration include poor self-esteem or self-efficacy, avoidance of motor activities, poor gross, fine, visual-motor coordination, and organization skills and sensory seeking. 22 Sensory reactivity problems are determined by direct observation and family interviews and caregiver questionnaires (eg, Sensory Profile [SP] or Sensory Processing Measure [SPM]) while sensory perception-based difficulties are primarily determined by direct observation, direct administered assessment measures (eg, Sensory Integration and Praxis Test [SIPT]) and sometimes with caregiver questionnaires (eg, the SPM is the only questionnaire that has questions on sensory perception and sensory perception-based problems). 25 Ayres Sensory Integration® (ASI) is an evidence-based intervention approach used to treat these sensory integration-based participation difficulties (ie, play, feeding, gross, and fine motor areas) in populations such as children with Autism Spectrum Disorder (ASD).25,26
There is very limited research on sensory processing and integration challenges in RSTS. Some studies have suggested that individuals with RSTS have behavioral patterns similar to individuals with ASD whose sensory processing and integration difficulties are well documented.13,28,29 Thus, examination of sensory processing and integration problems in the RSTS population as a potential contributor to these behavioral patterns is warranted as a previously unexamined area of concern. The knowledge base on child development points to the critical role of sensory–motor experiences for cognitive development, movement skills, emotion regulation, social relationships, and activity participation in early childhood,20,30,31 all areas which are severely compromised in children with RSTS. In addition, there are a considerable number of studies which describe the importance of sensory integration for the brain’s ability to generate appropriate responses to these sensory-motor experiences.20,22,32
RSTS is primarily treated by physical therapists using traditional motor performance interventions such as NDT. 33 These approaches are limited as they do not specifically address broader sensory-based issues or functional occupational performance concerns. Ayres Sensory Integration® (ASI), however, is a commonly used theoretical intervention framework used by occupational and physical therapists which address sensory integration-based fuctional motor skills. 22 This approach is often unknown and unused among therapists who work with individuals with physical disabilities. However, ASI is based on many principles of enriched environments such as sensory experiences, challenge, and active engagement which have been found to have positive effects on physical disabilities. 34 ASI is also guided by parent and client goals. In children with RSTS, the literature suggests that behavioral problems such as short attention and sudden mood changes that may affect social and cognitive performance and motor development are the most desired areas of change by parents.1,7,8,13,35 These areas align well with the goals of ASI intervention. Therefore, ASI intervention may prove to be a unique and important intervention for addressing the sensory motor challenges (and related behavioral and functional difficulties) found in children with RSTS.
This case report focused on possible sensory processing and sensory integration-based functional and motor problems in a child diagnosed with RSTS. Individualized intervention programs for children with RSTS are created according to the specific developmental difficulties identified in these children. ASI intervention was used for this case with RSTS due to reported possible sensory processing and integration problems by the family and the physiotherapist that referred the child for services. ASI intervention is based on sensory integration theory which articulates that sensory-motor skills may be improved through active participation in meaningful individualized sensory and motor experiences which increase the child’s ability to make adaptive responses to environmental demands and which consequently allow the child to better engage in functional activities. 36
Study objective
To investigate sensory processing, sensory integration and motor functioning of a 3-year-old child with RSTS pre and post 2 months of ASI intervention.
Method
Study design
A descriptive case report design was used to evaluate the effectiveness of ASI intervention on sensory processing, sensory integration, motor functions and parental goals in a 3-year-old child with RSTS. While there are limitations of case reports, they represent an important study design to advance scientific knowledge, especially of rare diseases such as RSTS. 37 The case report approach provides the researcher the opportunity to collect data from various sources and to analyze the data to illuminate the case38,39 and to analyze intervention outcomes. 40 Although the case report approach does not allow generalization of findings, it informs clinical practice by explicating clinical problems and useful solutions.
A specific method was utilized to gather and organize data as recommended by Schaaf and Smith Roley 41 (See Figure 1). The child was referred to the first author by his hospital-based physiotherapist due to lack of progress and concerns that the child had problems processing and integrating sensation which were interferring with his progress. A developmental and sensory history completed by the parents, an informal parent interview in which the family freely described their main concerns, and a review of previous evaluation reports supported these referral concerns and suggested that many of the parents’ concerns could be related to sensory processing and integration difficulties, thus a formal comprehensive sensory integration-based evaluation was completed. The evaluation consisted of systematic observations of the child’s responses to sensory activities in the clinical setting; parent completion of the Sensory Profile (SP) 42 and the Sensory Processing Measure-Preschool (SPM-P) Home 43 ; and administration of the Gross Motor Function Measure (GMFM) 44 and Peabody Developmental Motor Scales-2 (PDMS-2) 45 by the lead clinician. Based on the parent-report and therapist administered assessment data, specific goals were developed using Goals Attainment Scaling (GAS) and reviewed with the child’s mother to assure that the goals identified and addressed appropriate areas of concern (see Table 4). Post-intervention documentation was collected at the end of the second month of intervention which included the same questionnaires and assessments used at initial evaluation. A follow-up parent interview was also conducted to obtain feedback about the child’s past and present concerns and to investigate parent perception of the success of the ASI intervention program in meeting the child’s needs. Written consent was obtained from the family of the individual participating in the case study before the study started.

Method utilized to gather information. Adapted from Schaaf and Smith Roley. 41
Participant
A detailed developmental and medical history gathered from the child’s mother revealed that K is a 3-year-old male born after a full-term pregnancy. His medical history showed that he had meconium aspiration at delivery and was hospitalized in the NICU for 21 days. At 1 month of age he was diagnosed with Rubinstein-Taybi Syndrome at the Istanbul University, Istanbul Faculty of Medicine Hospital, Child Neurology department. After the diagnosis, the family was referred to the hospital’s early intervention services which consisted of pediatric physiotherapy and child development specialist supports. The child worked with the same professionals until 3 years of age who primarily utilized a traditional NDT intervention approach with minimal success. A comprehensive assessment conducted at age 3 by the early intervention team found that K continued to demonstrate significant delays in fine and gross motor skills, as well as social-emotional, language and cognitive areas. The professionals who completed the assessment concluded that K’s gross motor skills had progressed less than expected. Parents further reported that K was afraid of movement and they and the early intervention physiotherapist believed that his fear of movement was related to gravitational insecurity (a sensory integration-based movement problem) and his motor delay. Consequently, the physiotherapist referred K to the first author for a sensory integration evaluation and ASI intervention.
K’s mother was interviewed at intake to determine areas of challenge for K related to participation in home and community activities. His mother described K as a child who was anxious when confronted with a new person, object or environment and that he preferred to sit rather than move. She reported he was able to crawl on flat floors, stand up by holding on, and walk by holding on to the edge of the seat. She further reported that he refused to free his hands while standing, was not able to crawl on an angled or uneven surface, got stressed when he tried to sit on swing and refused new toys, especially textured materials. She indicated that his hand skills were not developed enough to manipulate crayons, spoon or fine motor toys in an age-appropriate manner and his expressive and receptive language was quite limited. He had 5 to 10 simple words, however, he was not able to use them in a sentence and he could only understand simple instructions. Moreover, she reported many concerns around all developmental areas. Primary concerns were that he was not able to walk independently, had difficulties in engaging in play activities that included moving objects such as ball play and that he was afraid of playground equipment such as swings. His poor communication skills, refusal to touch foods and being a picky eater especially in regard to solid foods were other major concerns of the family. The child was further assessed by a specialist for swallowing and no anatomical problems were found related to feeding.
Assessments
In addition to performing the detailed parent interview described above, an independent evaluator completed a series of assessments as noted above. No appropriate standardized therapist administered assessments for sensory integration are available for a child of K.’s age and disability level, therefore, parent report measures were the only option. A few measures were considered and rejected as they were not available to the authors or were not appropriate for the child’s developmental level. To obtain the best information, 2 different parent-report measures were used to evaluate sensory processing and integration functions. The Sensory Profile (SP), 42 which is the most widely used measure to evaluate sensory processing difficulties addresses largely sensory modulation and reactivity and related behavioral problems was completed. The Sensory Processing Measure-Preschool (SPM-P) Home, 43 which also addresses sensory modulation but, additionally, has questions related to sensory integration, (including perception and sensory discrimination) and praxis skills not addressed on the SP was also completed.
The SP is a 125-question standardized criterion-referenced family questionnaire that measures children’s responses to sensory events in daily life. It provides data about how patterns in sensory processing might contribute to, or create barriers to, performance in daily life. The version used was appropriate for children 3 to 10 years of age. Test-retest and inter-rater reliability is well established and the measure has been found to successfully differentiate between children who are developing typically and children with a range of developmental conditions.22,42 Scores are reported as raw scores which then are categorized as Typical Performance, Probable Difference and Definite Difference based on cut scores for each category. Thus change results are indicated by movement between categories and/or changes in raw scores by subcategories. No total score is available for the SP. Standard errors of measure are provided to identify confidence intervals for the raw scores. Raw score changes that result in non-overlapping confidence intervals for pre and post scores indicate statistically significant improvement. Scores are not rated by age.
The SPM-P Home is a 75-question standardized, parent/caregiver report questionnaire that requires the caregiver to rate the frequency of behaviors on each item. 43 The SPM-P Home includes areas of social participation, vision, hearing, touch, taste and smell, body awareness, balance and motion, and planning and ideas subscales. These areas assess different aspects of sensory integration (such as perception or discrimination), motor performance, and their impact on social participation. The SPM-P Home version used is appropriate for children 2 to 5 years of age. The measure has established discriminative validity between children with special needs from various clinical groups and typically developing children.22,46 Scores are reported in standard T-scores by age which are then converted to categories of Typical Function, Some Problems and Definite Problems based on cut scores. 95% confidence interval are provided for each T-score. With a single subject significance testing for pre post change in scores is accomplished by the presence of non-overlapping confidence intervals for pre and post T-scores.
The Peabody Developmental Motor Scales-2 (PDMS-2) 45 and The Gross Motor Function Measure-88 (GMFM-88) are performance-based therapist administered measures that assess fine and gross motor abilities. The PDMS-2 is comprised of 3 gross motor and 2 fine motor subtests and is appropriate for children 1 month through 72 months of age. The PDMS-2 generates standard scores for each subtest and gross motor, fine motor and total motor quotients. Confidence intervals are also presented for each score. The PDMS-2 has good discriminative reliability and validity and test-retest reliability is high.45,47
The GMFM-88 was used to examine gross motor development, although originally developed for children with cerebral palsy (CP) or e CP type motor problems, it is stated in the manual that it may be used with children with developmental delays or severe motor, so was deemed appropriate for this child. The GMFM-88 is a standardized criterion referenced measurement tool designed to be used for both clinical and research purposes to measure change over time and the effectiveness of interventions for children with disabilities, ages 5 months to 16 years of age based on performance of specific gross motor skills.48,49 The PDMS-2 was used in addition to the GMFM-88 as it provided a more comprehensive evaluation of all motor skills since it includes fine motor skills and object manipulation skills as well as gross motor skills. Scores on the GMFM-88 are reported as raw scores. No standard scores are available as the score is based on change of performance in specific skills. Therefore, it is impossible to report if changes are statistically significant or not.
The GMFCS examined self-initiated functional movements, with an emphasis on head and trunk control, sitting, transfers, and mobility. It is a 5-level pattern-recognition system (Level I represents the best gross motor abilities and Level V the least function) developed originally for children with cerebral palsy or other neuromotor diseases. The classification of level-specific motor abilities is age dependent, and there are specific motor ability definitions for various levels in each age band. There are 5 described age bands: before the second birthday, from age 2 to 4, from 4 to 6, from age 6 to 12, and from age 12 to 18 years. 50 Levels are reported as age bands. No standard scores are available.
Individual goals
Progress on individualized functional goals was gathered using Goal Attainment Scales (GAS). GAS is the most recommended goal setting methodology for measuring change during and after ASI intervention both in clinical and research applications. 51 Evidence suggests that GAS is a reliable tool for use with children with sensory processing and integration challenges. 52 GAS provides subjective information about the client’s needs and is a method of measuring the extent to which the client’s individual goals, set at the start of intervention, are achieved as a result of intervention. 53 In general, a 5-point scale (–2 to +2) is used for scaling goals. Zero (0) is specified as the predicted level of performance, with –1 indicating somewhat less than expected outcome, −2 much less than expected outcome, +1 somewhat more than expected outcome, and +2 much more than expected outcome. 54 While several other researchers have proposed different definitions for levels of this rating scale the GAS scaling used in this study was as described by Kiresuk et al. 54 All evaluations before and after the intervention were made by a therapist who was competent in the tests applied and was blind to the intervention (see Table 4).
Intervention
ASI intervention was selected as the most appropriate intervention approach for this child because a comprehensive assessment of K’s sensory processing, integration and motor skills revealed the presence of problems processing and integrating sensation. ASI intervention uses principles of sensory integration theory as developed by A. Jean Ayres and focuses on engagement in child-directed, sensory-rich experiences that are individually designed to address each child’s specific sensori-motor needs. 25 The therapist promotes and adjusts the sensory qualities of the environment, encourages self-direction and play while facilitating adaptive responses in motor, affective, social, language, and cognitive functions.34,41 The goal of intervention is to improve the child’s ability to process and integrate sensory information as a basis for enhanced independence and participation in daily life activities.22,36 ASI intervention is manualized with a well-validated fidelity measure. The data-driven decision making (DDDM) framework was used to guide the intervention and document the outcomes of intervention. DDDM is a systematic approach that is used to guide the clinican’s clinical reasoning and decision making by using data to guide assessment and intervention. The DDDM approach consists of 8 series of steps that create links from the child’s strengths and presenting concerns to collection and analysis of assessment data for hypothesis generation and testing. 25 Use of the DDDM approach facilitates replicability of the intervention process.
The Ayres Sensory Integration Fidelity Measure© (ASIFM) 55 was used to assure that the intervention provided for this case met the criteria for ASI intervention. Intervention was delivered by a physical therapist with advanced training and experience in ASI intervention and who met the therapist qualification outlined in the structural elements of the ASFIM. The therapist was trained in ASI with a minimum of 120 contact hours and was supervised by a physical therapist with more than 10 years of experience in the field of sensory integration intervention. Fidelity for both the structural and process elements of ASI intervention was met using the ASFIM. The therapy space met the structural elements with a rating of 100 of 100 points (Part I/Safe Environment: 10, Part II/Record Review: 38, Part III (A)/Physical Space: 10, Part III (B)/Available Equipment: 36, Part IV/Communication with parents and teachers: 6) as described in Parham et al. 55 To ensure that treatment sessions were in compliance with the process elements criteria of ASIFM, randomly selected treatment sessions from each week were rated by an experienced therapist that was trained on the ASIFM. The mean ASIFM process elements score of 8 randomly selected intervention sessions was 82.75 out of 100 which meets the criteria for fidelity. The therapist ensured physical safety, presented sensory opportunities, helped the child to attain and maintain appropriate levels of alertness, challenged postural, ocular, oral, or bilateral motor control, praxis and organization of behavior, collaborated in activity choice, tailored activity to present just-right challenge, ensured that activities were successful, supported the child’s intrinsic motivation to play and established a therapeutic alliance as described in the ASIFM process elements.25,55 Intervention was provided for 50-minute sessions, 3 sessions per week, over a period of 8 weeks (Figure 2). The intervention was clinically-based and the family was informed about the intervention at the end of each session. No recommendation were made for any home activities and the family was advised to continue their routine daily life. See Figure 2 for examples of treatment activities.

Sample activities from different ASI intervention sessions.
Results for this descriptive case report are provided in 2 primary formats. Descriptive observational changes noted in functional performance and objective data obtained from pre and post testing. Because single cases using a pre-post format cannot be empirically tested using traditional significance testing (eg, t-tests, ancovas, etc.), use of confidence intervals derived from population data is recommended as an acceptable means of determining if variability in pre-post scores is likely related to chance or not. 95% confidence interval are thus applied to each score. When pre-post scores have non-overlapping confidence intervals, this reflects effect sizes greater than 1 and indicates that the results are not likely to have occurred by chance, thus represents a true change. 56 Therefore, this method was used, where possible, to determine if reported changes indicate true change or not. All confidence interval information was obtained from the appropriate assessment manuals.
Results
Observation changes
Unstructured clinical observations before intervention found that K was afraid of swings and most of the moving objects in the clinical setting such as big therapy balls. He also avoided moving his head out of a vertical position or moving on high platforms. K avoided touching most of the tactile objects provided such as beans, fidget toys, and plush toys. He also rejected participation in messy activities such as playing in shaving cream. Although the child was able to crawl he was not able to navigate an obstacle course of uneven surfaces consisting of big mats, tunnels, and wedges. The child used gestures to ask his parents to do something for him such as bring a toy or help him move close to an object. His play repertoire was limited to activities such as pushing, pulling, or throwing objects. Further, clinical observation found that gravitational insecurity (GI), which is known to be related to vestibular processing was identified in this child. Indicators of GI were: child’s dislike for feet off the ground, fear of unstable surfaces, head position out of upright, and fear of disorienting visual stimuli such as moving objects in the environment.
After 2 months of intervention K demonstrated a clinically observable reduction in his gravitational insecurity. He was able to sit and enjoy swings while the swing was moved by the therapist. He was able to climb on or off the swings; and moving objects in the environment no longer bothered him. His participation in tactile play experiences increased and he started to explore objects more with his hands. The child was able to crawl over various objects in the obstacle courses and engaged in many activities involving gravitational challenges such as being on platforms high above the ground. One of the biggest developments observed was that the child started to take several independent steps on flat ground. Further, K’s parents reported that he started to climb on the furniture and to show more interest in exploring places at home after intervention. His parents also observed that K now enjoyed ball play with his father and that he started to use utensils at meals.
Assessment findings
Processing and integration of sensation
Performance changes on the SP were reported in 2 formats, changes in descriptive categories which reflect functional changes and raw scores with confidence intervals which provide insight into the statistical trustworthiness of the results. In the area of descriptive categories, before intervention, K’s SP revealed 6 definite differences, 5 probable differences, and 3 typical performance scores in the sensory processing categories. He further had 3 definite differences, 1 probable difference, and 5 typical performance scores on the factor scores of the SP before treatment (see Table 1-Before Therapy). Pre-intervention SP results demonstrated that K had definite problems in the areas of vestibular, touch, and oral sensory processing. Findings from the SP also showed that K had definite sensory processing difficulties related to endurance/tone, modulation related to body position and movement, and definite differences on behavioral outcomes of sensory processing. The factor summary of the SP showed that K had definite differences on low endurance/tone, oral sensory sensitivity, sensory sensitivity, and on fine motor/perceptual. SP scores after 8 weeks of ASI® intervention demonstrated significant changes in many category scores (see Table 1 for specific category changes). These areas included vestibular processing, touch processing, oral sensory processing, sensory processing related to endurance/tone, behavioral outcomes of sensory processing and factors of sensory seeking, emotional reactivity, low endurance/tone, inattention/distractibility, sensory sensitivity, and sedentary.
The Sensory Profile ratings according to raw scores and confidence intervals for K.U. before and after therapy.

Scores with *indicate significant changes in performance. Changes among categories and factors after therapy are highlighted in.
In the area of objective changes, significant improvements were identified in all areas that changed functional categories as post-test scores reflected non-overlapping confidence intervals with pre-test raw scores. K demonstrated significant improvements in vestibular, touch and oral sensory processing. Post-intervention SP results also revealed that K performed significantly better in endurance and tone. Positive significant changes were also noted on behavioral outcomes of sensory processing suggesting that K performed better behaviorally at home. Performance on all factor categories were significantly improved except for oral sensory sensitivity, poor registration and fine motor/perceptual. See Table 1.
The SPM-P Home scores were reported in the same manner as the SP, change in the descriptive category (based on raw scores) and reporting of confidence intervals. In this measure confidence intervals are based on the derived T-scores for the measure. Before intervention K had definite dysfunction in total sensory integration and in the areas of social participation, hearing, touch, balance and motion, planning and ideas, vision and some problems in body awareness (Table 2). K was over-responsive to sounds, touch and motion. Poor visual discrimination and body awareness were definitely decreased. Following intervention, K’s SPM-P Home raw scores showed improvement by changing the test’s interpretive category from Definite Dysfunction to Some Difficulties in visual, hearing, touch, balance and motion subtests, and total sensory integration indicating functional improvements in these areas. Gains in social participation, body awareness, planning and ideas subtests were not sufficient to change the test’s interpretive category. See Table 2.
SPM-P Home category ratings according to raw scores and raw scores before and after treatment.

Cores with *indicate changes among categories after therapy.
Objective scores on the SPM-P demonstrated decreased scores (eg, improved performance) in all areas except planning and ideas (see Figure 3). No areas had change sufficient to result in non-overlapping confidence intervals. However, hearing and the total score are only 0.2 SEM’s different, a functionally negligible difference (see Table 3).
SPM-P Home standard T-score confidence intervals before and after treatment.


SPM-P Home standard T-scores before and after therapy (Lower scores indicates improvements). No significant changes in T scores were found BT and AT. Abbreviations: BT, before therapy; AT, after therapy.
Motor performance
Pre-intervention PDMS-2 assessment results found that K had below average performance in both gross and fine motor areas. After intervention, K demonstrated improvements in raw scores for all areas except the stationary subscore (Table 4). Standard scaled scores improved in all areas except stationary and visual-motor integration. Gains in object manipulation and grasping subscores indicated changes among categories after therapy. Object manipulation changed 1 category from Very Poor to Poor and grasping changed 2 categories from Very Poor to Below Average. However, these improvements in scores pre- to post-intervention did not result in non-overlapping confidence intervals for each score. Thus while changes suggest there were observable functional improvements, it was impossible to determine if these changes were statistically significant as no confidence interval information was available for these scores (see Table 4). The developmental quotients of Gross Motor, Fine Motor and Total Score also reflected improvements in standard scaled scores in all 3 areas. The Fine Motor Quotient changed descriptive category from Very Poor to Poor. However, the confidence intervals for the Gross Motor and Fine Motor scores were overlapping suggesting no significant improvement. The Total Score confidence intervals overlapped by only one point (eg, both included a score of 58), this again is a negligible overlap and may represent a significant overall change in motor performance (see Table 5).
PDMS-2 subscale raw scores, standard scores, and descriptive ratings before and after therapy.
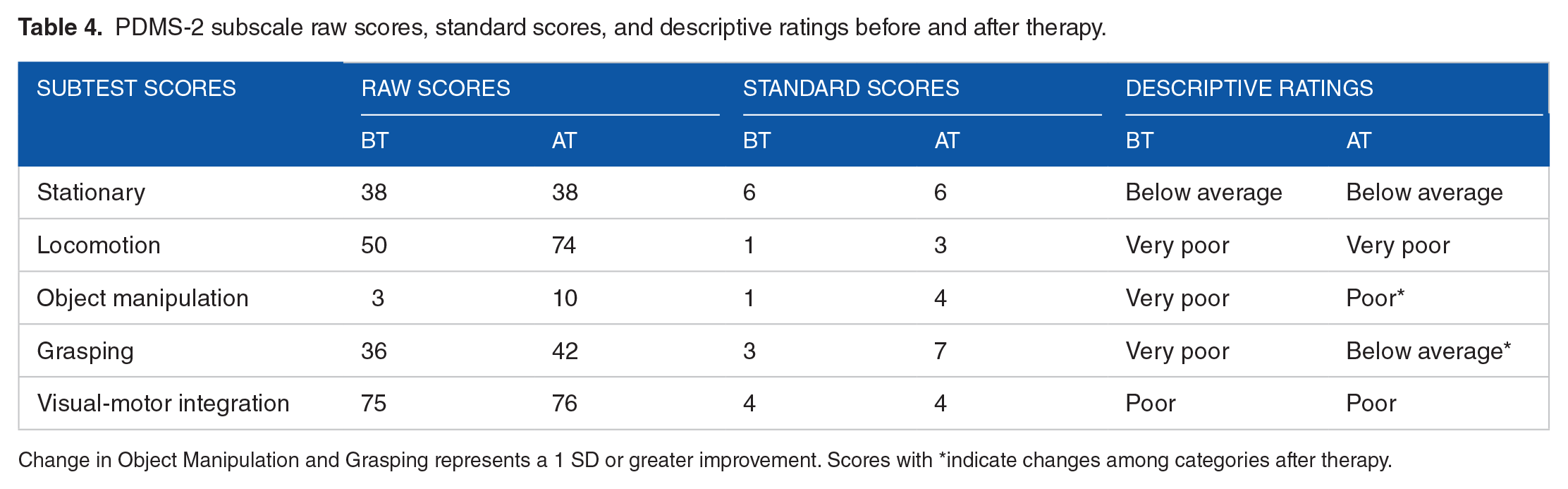
Change in Object Manipulation and Grasping represents a 1 SD or greater improvement. Scores with *indicate changes among categories after therapy.
PDMS-2 quotient scores and confidence intervals before and after intervention.

Abbreviations: BT, before therapy; AT, after therapy.
Scores with *indicate changes among categories after therapy.
The GMFM results are presented as percentage of raw scores out of a total possible score. No standard scores or confidence intervals were available. Pre-intervention GMFM scores were 51/51 (100%) for gross motor activities of lying and rolling; 48/60 (80%) for sitting; 24/42 (57.1%) for crawling and kneeling; 5/39 (12.8%) for standing; 12/72 (16.6) (for walking, running, and jumping; and 140/264 (53%) for total score. Post-intervention, K demonstrated improvement in performance of discrete gross motor skills in 4 GMFM subscores and the total GMFM score (see Table 6). His scores improved 20% for sitting; 14% for crawling and kneeling; 33% for standing; 11.5% for walking, running and jumping; and 16% for total score. These reflect production of specific developmental motor skills that were not present prior to intervention and which had not developed over the 3 years of previous NDT-based therapy.
GMFM scores before and after ASI therapy compared to maximum possible scores for age.

Abbreviations: BT, before therapy; AT, after therapy.
K’s observed gross motor performance initially was classified as Level III on the GMFCS (Table 7) at pre-intervention. Post-intervention observations, however, found K made definite functional progress with change in gross motor performance to a GMFCS level I-2 (Table 7). This change indicated an improvement of 4 to 6 months of development over 2 months of intervention. While no standard scores are available for this measure this change suggests a greater gain than would have been expected by normal development alone, thus suggesting a significant improvement in performance of functional gross motor skills following ASI intervention.
Description of GMFCS Levels for ages between second and fourth birthday, and childs’s motor performance according to GMFCS levels before and after therapy.

Functional goal attainment
K’s goal attainment scales, established prior to intervention, were rated by his parents post-intervention. K attained the expected level of outcome for goals 2 and 4 and demonstrated more than the expected outcomes for goals 1, 3, and 5 as depicted in Table 8. This resulted in a overall GAS score of 1 which indicates that K demonstrated somewhat more progress than expected following intervention. The GAS score of 1 translated to a t-score of 65.08 which reflects significant improvement on the goals 1.5 SD above expected performance. T-scores of 45 or greater indicate the child has achieved or exceeded the expected goal performance.
Goal Attainment Scale post-intervention.
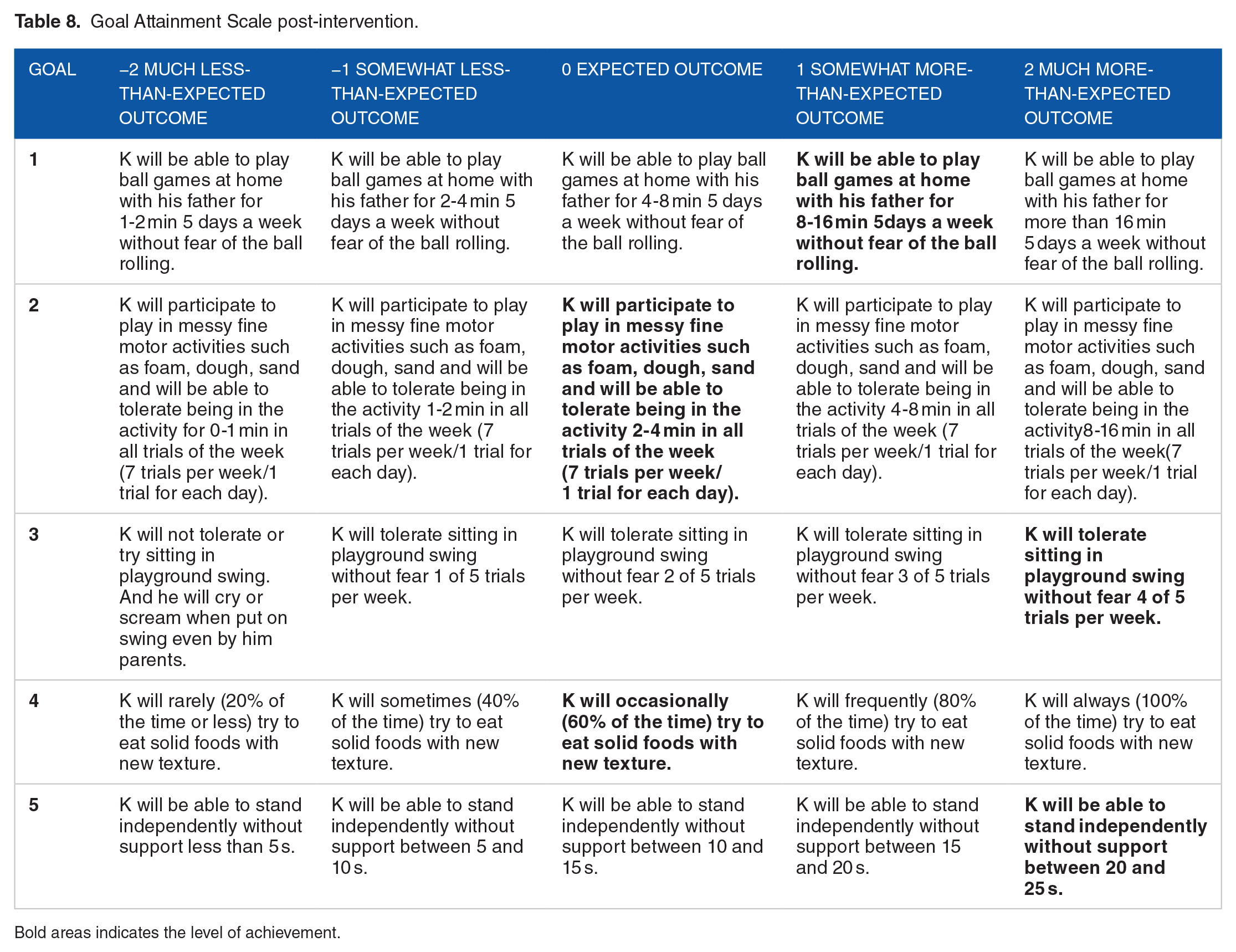
Bold areas indicates the level of achievement.
Discussion
This case report is the first known example of the use of Ayres Sensory Integration® intervention with a child with RSTS with difficulties processing and integrating sensations. Results provides preliminary support for the effectiveness of ASI intervention on sensory processing (particularly sensory modulation/sensory reactivity), functional gross motor skills, fine motor and functional parental goals in a young child with RSTS. Observable changes were also noted in reduction of gravitational insecurity symptoms and improvement in behaviors.
Outcomes in this case report were obtained from a variety of sources including observation of functional skills and behaviors as well as use of standardized assessments. As has been previously reported in the ASI literature, there were challenges in the use of some of the standardized assessments. 28 In the area of processing and integrating sensations, the Sensory Profile found numerous significant improvements in behavior and functions, while the Sensory Processing Measure had no significant results. This difference may be attributed to the Sensory Profile primarily capturing changes in behaviors associated with sensory modulation and overall behavior. While the Sensory Processing Measure reflected improved scores, these were not found to be significant. This is possibly due to the fact that this test measures sensory modulation but also measures sensory discrimination and praxis skills not captured on the Sensory Profile. It is possible that changes in these areas of discrimination and praxis were not sufficient to result in statistically significant changes with the short duration of intervention provided to this case.
In the area of motor skills, the Gross Motor Function Measure, the Gross Motor Function Classification System and the Peabody Developmental Motor Scales all demonstrated improved performance in areas of fine and gross motor functioning. The PDMS, however, did not reflect significant gains. This is likely due to this measure not being sensitive enough to capture change in motor performance at this child’s age and developmental level. Unfortunately, there are few standardized motor assessments appropriate for the age and functioning level of this child. The GMFM and the GMFCS, which examine functional skills, demonstrated more observably significant functional change but unfortunately do not have standard scores to allow for significance testing as their emphasis is on observable change. The findings of the sensory and motor tests is consistent with challenges demonstrating change in foundational mechanisms identified in the ASI literature.28,57
The greatest changes were noted on measures and daily observations that captured functional performance change such as the Goals Attainment Scales. This finding is also consistent with recent studies examining ASI intervention effectiveness58,59 which recommend that outcomes of ASI intervention focus on functional performance instead of measuring change in foundational mechanisms. Thus this case report provides important preliminary information on the use of ASI intervention with children with RSTS.
There is no known research in the literature on processing and integrating sensations in individuals with RSTS. Sensory processing and integration difficulties which may affect participation in daily life are commonly reported in children with neurodevelopmental disorders.60 -65 Outcomes of this case report align with research that suggests ASI intervention has positive effects on sensory processing and integration, motor function, and participation in children with developmental difficulties.26,58,66 -72
Problems in social, cognitive, and motor development observed in children with RSTS are clearly noted in studies conducted to date.13,14,33 Motor concerns such as low muscle tone have been linked to the motor developmental delays seen in children with RSTS. 73 These children may also have difficulty in proprioceptive processing due to low muscle tone16,17 and poor proprioceptive processing could be one of the factors that effects motor functions. On the other hand, low muscle tone, clumsiness, poor coordination, and insufficient postural control seen in individuals with RSTS 15 may be a result of poor vestibular processing. 22 The Sensory Profile results of the child in this study revealed a definite difficulty with endurance/tone and vestibular processing, which may affect motor functions. Further, gravitational insecurity (GI), which is known to be related to vestibular processing also was identified in this case. In children, GI may interfere with participation in many daily activities 52 and K’s avoidance of standing on his feet without external support, avoidance of moving in different planes, or trying new motor activities could be a result of GI. RSTS individuals may have visual or hearing impairments,74,75 however, auditory processing deficits have not been found in the research to date, except for a brief note on noise intolerance. 14 Moreover, evaluation results clearly demonstrated K.’s auditory over responsivity.
Feeding difficulties are another challenge faced by individuals with RSTS and their parents. 18 Oral sensory sensitivity observed in this case may be one of the causes of feeding problems.20,76 Malformations of the hands and thumbs often cause obvious object manipulation difficulties in these children. Beyond the structural limitations seen in RSTS, tactile defensiveness found in this case can also be another important factor that causes hand withdrawal and avoidance of manipulative functions of the hand.19 -22 Furthermore, there are studies which demonstrate that RSTS individuals have behavioral patterns similar to those with ASD.13,27,75 Since difficulties processing and integrating sensations are very common in the ASD population,28,29 there is a clear need for assessment of sensory processing and integration in the RSTS population. Families of children with ASD report that behaviors associated with difficulties processing and integrating sensations create social isolation for their child, restrict participation in daily living activities and impact social engagement. 28 Consequently, ASI intervention is the most often requested service by parents of children with ASD to address problems associated with difficulties processing and integrating sensations. 77 Data provided by randomized controlled studies found that ASI® intervention has positive affects on social-communication, self-care and adaptive behaviors, preacademic skills, challenging behaviors, and motor skills of children with ASD28,72 ASI® is also now accepted as an evidence-based intervention for ASD. 26 Accordingly, it can be hypothesized that ASI intervention may help ameliorate ASD-like difficulties seen in RSTS.
A wealth of data confirming the beneficial effects of enriched environments (EE) comes from different experimental studies.78,79 EE is seen as a method of intervention with significant curative effects for many neurodevelopmental and neurodegenerative disorders.80 -86 Nozari et al 87 showed that EE treatment prevents deficits related to cognitive performance, spatial learning, memory, and motor functions in postnatal MK-801 treated rats. A study on RSTS mice has shown that exposure to EE resulted in remarkable improvements in motor skill learning and memory. 88 Lopez-Atalaya et al 89 further suggested that occupational therapy that uses EE may also ameliorate deficits seen in RSTS. After comparing 7 essential features of EE (sensory experiences, structural features, novelty, challenge, active engagement, play/enjoyment social and safety) with ASI, Reynolds 33 suggested that ASI intervention shares many common features with EE. Moreover, structure and process elements of the ASIFM also meet these 7 common features of the EE model. Morgan et al 90 describe 4 elements of EE interventions: cognitive, sensory, motor, and social. ASI intervention includes these 4 elements of EE with an emphasis on sensory enrichment. 25
Based on this information, positive effects of ASI on RSTS may be related to the intervention’s enrichment effects. EE effects expression levels of genes (some of these genes are known to be associated with learning and memory) involved in neuronal structure, synaptic signaling, and plasticity.91,92 Furthermore, researchers demonstrated that exposure to EE may induce an increase in brain-derived neurotropic factor (BDNF) levels in rodents, which leads to changes in synaptic plasticity in the brain.93 -95 Thus improvements observed in this RSTS case may be related to both gene expression changes and increased BDNF due to the EE effects of the ASI intervention.
Finally, there are a number of limitations to this case report. The use of only parent report for assessment of sensory processing and integration skills may introduce some bias. Also, the use of ASI intervention for only 2 months may not have resulted in as robust outcomes as might occur over a longer period of time, especially in the areas of sensory discrimination and praxis. This short intervention period also may have resulted in standard score changes that were not statistically significant due to large standard errors of measure. It is also possible that standardized assessments such as the PDMS-2 and SPM-P are not sensitive enough to detect statistically significant changes over a short period of time. In future studies, use of specific sensory integration assessments such as post-rotary nystagmus 96 or specific therapist-administered praxis tests would be warranted if appropriate for the age and developmental level of the children being evaluated. Further research over a longer intervention period and use of an A-B-A single case study design would address some of these concerns in future research. Use of blind examiners for the standardized administered assessments, however, were a strength of this case report as was documentation of the clinical reasoning process and use of the ASI fidelity measure to assure intervention fidelity. Finally, one case report which used principles of NDT demonstrated improvement in motor skills on the GMFM similar to those found in this report. 33 Therefore a future study should compare NDT and ASI.
Conclusion
This case report demonstrated the first evidence of difficulties processing and integrating sensations in a child with RSTS. Results provided preliminary support for the effectiveness of ASI intervention on processing and integrating sensations, gross and fine motor function, and parental goals of a child with RSTS. Although this case provided information that can be useful for clinicians working with children with RSTS, as a case report, the results cannot be generalized to the larger population of individuals with RSTS. Additional studies are needed to validate these findings and to address limitations in the study.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author’s Note
Ayse Firdevs Aracikul Balikci is now affiliated to Paşabahçe Secondary School, İstanbul, Turkey.