
Abstract
Rett syndrome (RTT) is a neurodevelopmental disorder characterized by severe dyspraxia, hand stereotypies, and sensory processing issues for which there is no known treatment. This case describes a child with classic RTT and the child’s responses to an Ayres Sensory Integration (ASI) treatment intervention (36 one-hour sessions, 3 per week). We coded and analyzed 36 detailed treatment notes to answer the following questions: What strategies and factors facilitated or interfered with participation in the intervention? What critical elements of treatment documentation might detect small changes in praxis and participation? How do patterns of motor or praxis milestones that emerge over time relate to this child’s level of participation? We observed an increase in participation when the therapist incorporated elements of neurodevelopmental treatment (NDT) and motor learning theory– treatment strategies commonly used with children who have neuromotor conditions. This increase in participation in the ASI intervention emerged at approximately the same time that the therapist documented acquisition of new motor and praxis skills. We observed the importance of using: lateral movement activities to develop weight-shifting and bilateral coordination, rotary play to increase trunk rotation and improve postural transitions, and rhythm to promote continuing or initiating actions. The documentation of the specific amounts of assistance and prompting needed during treatment sessions was an important tool for tracking small yet meaningful responses to treatment. This case illustrates a novel use of ASI intervention supplemented with strategies that developed foundational skills, and the emergence of praxis and participation in the therapeutic intervention. We suggest further research is needed to determine efficacy of ASI for other children with this rare disorder.
Keywords
Introduction
Rett syndrome (RTT) is a disabling neurodevelopmental disorder that primarily affects females and occurs in about one in every 10 000 live female births—roughly 7000 per year. Most cases are linked to mutation of the MECP2 gene. Children with RTT appear to develop typically during early infancy then they go through a period of regression around 6 to 18 months. This involves loss of previously acquired spoken language and gross motor and functional hand skills. They also develop dyspraxia of hand use and gait, sensory processing issues, and persistent hand stereotypies.1-3 Although difficult to assess, cognition may range from low average to severely impaired. 4
The severity of the dyspraxia5,6 associated with RTT combined with loss of previously acquired motor and speech/language skills severely limit active participation in nearly all facets of their lives. They may not be able to complete basic tasks of grasping or manipulating objects to feed or dress themselves, participate in school activities, or play with toys or peers. 2 Most depend on their families or caregivers for their personal care and require long-term specialized education and therapies. The impact and stress on these families can be very significant. 7 There are no studies that demonstrate effective treatment for their severe dyspraxia. 8
Serum Brain-Derived Neurotrophic Factor (BDNF)—a protein important for synaptic formation and neuronal activity that underlies balance and motor learning is reduced in those with RTT. 9 Studies with Mecp2 animal models housed in enriched environments (EE) (cages with climbing toys, a running wheel, textured objects changed every few days) found they developed an increase in the number of synapses in the brain, an increase in cerebellar BDNF expression, improvements in motor coordination, and a reduction of anxiety related behavior, compared those housed in barren cages.9-11 In a study of 12 girls with MECP2 mutations, Downs et al 12 found that BDNF increased and motor skills improved following an intervention that combined EE and targeted motor-learning techniques.
There are parallels between the environments described in EE studies and Ayres Sensory Integration (ASI) treatment, 13 an intervention developed to treat children who have sensory processing disorders, typically used by itself.9,14,15 ASI is provided by specially trained therapists in a sensory rich play environment—a space that contains adapted swings, therapy balls, scooter boards/ramps, rotating/bouncing/climbing equipment, and a variety of multi-sensory materials.9,12,15,16 According to ASI theory active engagement in a rich sensory-motor play environment with a just-right challenge promotes adaptive responses and neuroplastic changes 13 that improve skill, function and participation. Recent research of children with autism spectrum disorders suggests that ASI therapy heightens sensory awareness of the body’s position and movement and improves sensory processing and praxis abilities, which can lead to more active participation in important childhood occupations, including self-help, play and school activities.13,16-19 An earlier quantitative study used an interrupted time series design to investigate the efficacy of ASI in developing functional reaching and grasping in five children with RTT/Rett-related disorders. 20 That study provided preliminary data suggesting ASI had small positive effects on grasping objects. To better understand possible underlying mechanisms of this earlier study, we conducted a rigorous qualitative analysis of treatment notes of one child in that study to explore the relationship between observed praxis milestones and the child’s response to ASI treatment. Specifically, we addressed the following questions:
What strategies and factors facilitated or interfered with participation in ASI intervention?
What critical elements of treatment documentation may be useful to detect small changes in praxis and participation?
How do patterns of motor or praxis milestones that emerge over time relate to the child’s level of participation?
Case Representation
Participant information
In the earlier ASI study, 20 the Institutional Review Board gave approval to enroll 5 participants within the full range of RTT/Rett-related disorders. Written parental consent was obtained for participation and publication of study findings, including follow up case reporting. Of the 5 children with RTT/Rett-related disorders, only 2 had diagnoses of classic RTT, and of the two, one had never ambulated. Since approximately 60%-80% of children with RTT are ambulatory at some point in their childhood, 21 we chose to study the child who ambulated, in order to be most representative of other school age children with this condition.
This child is an 8-year old girl diagnosed with classic RTT (Mecp2R168X). She has severe dyspraxia, hand stereotypies, poor hand grasp, gait abnormalities, difficulty initiating motor actions and postural transitions, and GI issues. She requires full assistance to participate in all activities of daily living.
Table 1 summarizes this child’s abilities and areas of need at baseline, based on the following sources: occupational therapy (OT) evaluation, including sensory processing assessment; sensory processing surveys completed by her teacher and mother; OT treatment notes prior to the intervention; multidisciplinary team reports of present levels of performance from the Individualized Education Plan (IEP); and team quarterly reports on the student’s progress toward IEP goals. The team included her school physical therapist, speech language/communication therapist (SLP), classroom OT (different from study intervention therapist), school psychologist, teacher of students with visual impairment, music therapist, classroom teacher, and parent. A summary of her OT evaluation (Supplemental A), goals of the ASI intervention (Supplemental B), and description of ASI intervention (Supplemental C) were prepared by the OT providing the ASI intervention.
Participant’s occupational profile.

See Supplemental B Sensory Processing Evaluation Summary.
Relevant past interventions
School records show that primary concerns from at least 4 years prior to the intervention involved this participant’s mobility, communication, sensory processing, and self-regulation issues, as well as extremely limited hand use and participation in classroom activities, play, and self-care routines. This child attended a private school for children with substantial special needs, and received the following traditional therapeutic services at school:
Physical therapy: provided individual and group therapy for strengthening, balance, and mobility—specifically, increasing walking distance without stopping, and stair climbing
Occupational therapy: addressed sensory modulation, joint mobility, hand skills, self-feeding, and oral motor function through individual and group therapy
Speech and language pathology: addressed communication through individual therapy using a total communication approach relying on eye gaze
Music therapy: to increase language and participation.
Quarterly reports over this 4-year period prior to the study intervention revealed little to no measurable change in hand function, praxis, mobility or gravitational insecurity. Throughout this period, this child needed full assistance for all postural transitions, personal care, and for using classroom tools and materials, as described in her Occupational Profile (Table 1).
Treatment
Sensory integration is the ability to sort, organize and make use of the information simultaneously received by our senses (visual, auditory, tactile, proprioceptive, and vestibular). Sensory processing difficulties often lead to delays in motor development, praxis, self-regulation, learning, and social participation.17,22 ASI intervention addresses the child’s ability to organize and use this sensory information to respond in an adaptive and organized way. 23 ASI is implemented by therapists with specialized training, who adhere to specific guidelines set by the Ayres Sensory Integration Fidelity Measure© (ASIFM) . 16 ASI therapy (different from sensory diet or sensory regulation strategies) is conducted in a space that contains a variety of adapted swings, therapy balls, scooter boards, rotating/bouncing/climbing equipment, and multi-sensory materials. The therapist playfully supports the child through just-right sensory-motor challenges on this equipment, to facilitate adaptive responses, new skill development, and ultimately increased participation. 16
Since ASI is typically used to treat children who can initiate play on movable therapy/playground equipment with relatively minimal support or assistance, we anticipated that this child would require several accommodations to achieve fidelity to ASI and to maximize the functional outcome of ASI therapy. These included: the use of an individualized, total communication system to determine the child’s activity choice; adaptions to the physical environment and therapy equipment to accommodate for difficulty initiating movement and getting on/off therapy equipment, and to promote safety; cueing to participate in postural transitions; and extended wait-time (30 seconds) after cues to promote initiation of intentional movement and participation.24,25 Frequency and duration of the intervention were set at 36 sessions, 3 hours per week over a 3-month period based on review of ASI dosage literature. 26 Staff from The Koomar Center/Spiral Foundation affirmed the fidelity of the ASI intervention using the ASIFM . 16 This included a site visit (for space, equipment and safety checks) and remote scoring of some hour-long video recordings of treatment sessions to verify required process elements.
Method for analysis
This case report focuses on findings from one data source—treatment notes written after each intervention session by the treating OT. These notes were recorded on an Excel spreadsheet designed to document details of this participant’s responses during treatment sessions and the OT’s adherence to ASI fidelity. 16 On this spreadsheet the therapist recorded information pertaining to targeted goals, adaptive behaviors, quality of movement (eg, trunk rotation and weight-shifting), level of cues/assistance/participation, the child’s activity choices and how they were determined, and factors that interfered with and/or supported the development of praxis, sensory processing, and participation.
We systematically examined treatment notes using a priori codes based on ASI theory and best practices in OT. We used 8 categorical a priori codes, with more finite codes (sub-codes) positioned within each of the 9 categorical codes.
Table 2 identifies the coding categories and sub-codes. We primarily applied descriptive codes (to label/name observations), process codes (to label observable actions), and magnitude codes (to label levels of performance) as described by Miles et al. 27 The a priori categorical codes were: (1) sensory processing; (2) postural functions; (3) bilateral integration; (4) visual processing; (5) praxis; (6) participation; (7) strategies; and (8) interfering factors. Refer to the Coding Manual (Supplemental D) for detailed descriptions of coding categories and sub-codes.
Coding categories.

When coding and analyzing the data, we followed guidelines for establishing trustworthiness outlined by Braun and Clarke, 28 Nowell et al, 29 and Creswell. 30 These included peer debriefing, triangulation, and maintaining an audit trail of judgments and decisions. We describe the methods for documenting baseline functioning and measuring responses to treatment in our tables and supplemental files. Raw data that includes rich descriptions of the ASI intervention and participant responses during each intervention session is provided in Supplementals E and F. The authors’ data analysis can be cross-checked with all supplementals and tables.
Two OTs, with Sensory Integration Certification and expertise with RTT and ASI, independently read through all notes to gain a holistic overview before conducting 4 systematic passes through the treatment notes (rounds of coding). Both therapists were study authors—one was the treating therapist during this intervention.
After separately (blind) coding each pass, these therapists compared codes, discussed differences, and came to a consensus on the appropriate codes and emerging themes. In the first pass, we analyzed treatment notes using a priori codes. During the second pass, we synthesized treatment notes into a chart noting areas of interest and themes for further examination (Supplemental E). This chart also identified strategies that supported as well as factors that interfered with engagement and function. In the third pass, we studied the relationship between levels of participation and the emergence of sensory motor/praxis milestones (Supplemental F). For this chart, we assigned scores from zero (none) to 5 (independent) representing levels of assistance and/or participation of tracked items over the 36 sessions, and color-coded treatment sessions to indicate when highest levels of function/participation were reached and reliably maintained.
We condensed this chart into a timeline of weekly averages of sensory and praxis milestones, to view week-to-week relationships and participation patterns (Table 3). In our fourth pass, we further analyzed temporal associations between emerging sensory processing, acquired motor milestones, and levels of participation.
Sensory and praxis milestones: Weekly average of levels attained each week (3-sessions per week).

Bold number with *= skill becomes predictably reliable at this level. Key: 0 = Full (100%) passive physical assistance required, no active participation. 1 = Moderate (75%) physical assistance is needed for her to continue part of a motion/action while assisted practice is faded. 2 = Minimal (25%) physical assist is needed to continue partial or entire motion/action as assisted practice is faded, OR sustained grasp once placed. 3 = Touch prompt and/or gesturing cue needed for her to initiate and complete at least part of a motion/action. 4 = Initiated after physically assisted practice was stopped, she resumed same action and completed at least part, OR initiated part of a sequence of an action w/o physical cues. 5 = Initiated and completed the action independently, or used this skill while performing another more complex functional action.
Outcomes
During our coding process, we examined the following: factors that interfered with this child’s participation in ASI sessions; strategies that supported access to and promoted participation; critical elements of documentation that captured subtle responses to treatment; and patterns of motor or praxis milestones that emerged and relationship to participation.
Table 4 outlines the factors that adversely affected this child’s active participation in the ASI therapy process. The severity of her dyspraxia and hand stereotypies, and issues with neuro-motor delays, sensory processing, communication, and cognition necessitated varying levels of assistance/cues, particularly during the first month of treatment. The therapist assessed the child’s tolerability of the treatment during each session. Medical issues occasionally affected her participation, including gastrointestinal discomfort, upper respiratory infections, and fever. During those events the therapist consulted with the school nurse, sometimes vented her g-tube, and/or re-scheduled the therapy session.
Factors that interfered with participation during initial sessions of ASI intervention.

During our coding process, we identified several strategies the therapist used that were associated with increased participation in the ASI therapy sessions, over time (Table 5). These included elements of neurodevelopmental treatment (NDT) 31 and motor learning theory 32 that are often used by experienced therapists to treat individuals with neuromotor disorders.
Strategies that supported participation in ASI.

A spreadsheet was designed to document fidelity to the ASI intervention and to capture subtle responses to treatment to help the therapist monitor progress and/or the need to modify the approach (see Table 6). The recording of specific cues and the least levels of prompting and assistance needed throughout treatment sessions, enabled us to detect small steps that signaled the emergence of new skills. 33
Critical elements of documentation to capture subtle responses to treatment.
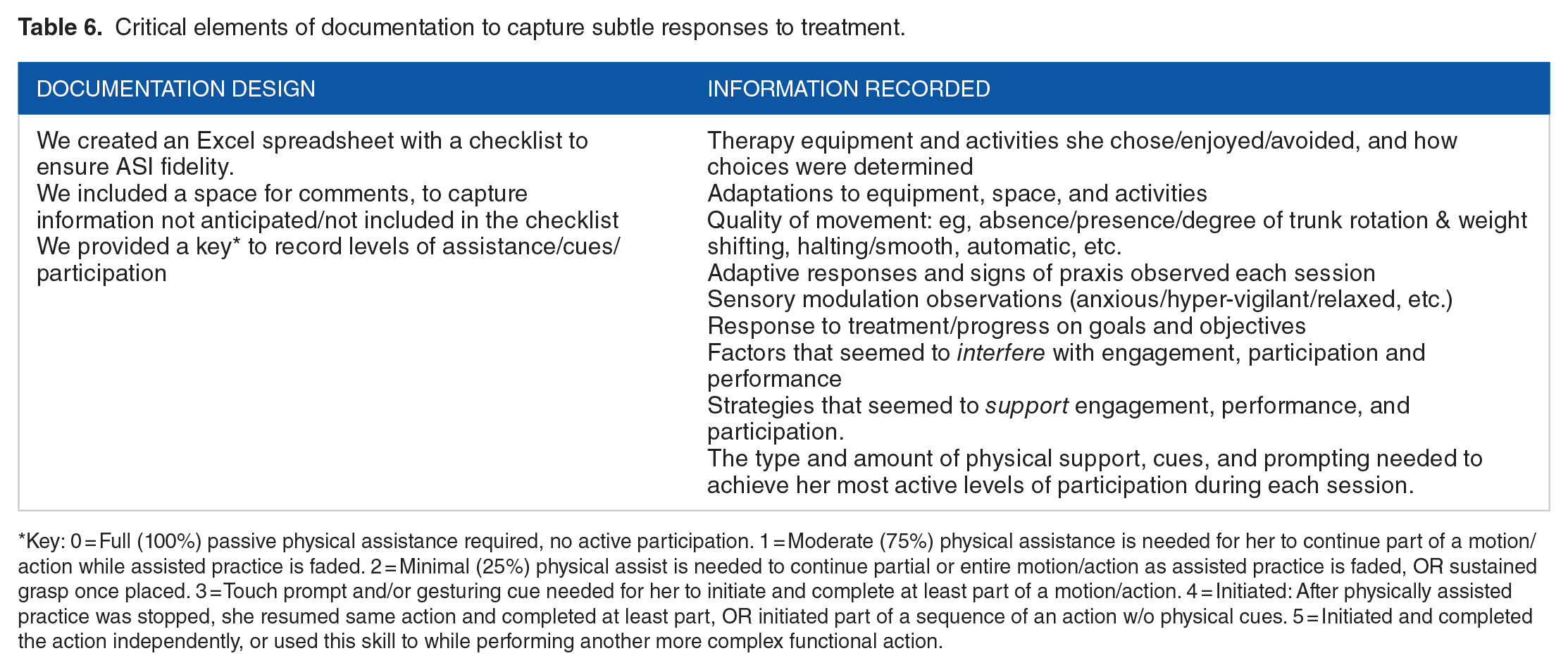
Key: 0 = Full (100%) passive physical assistance required, no active participation. 1 = Moderate (75%) physical assistance is needed for her to continue part of a motion/action while assisted practice is faded. 2 = Minimal (25%) physical assist is needed to continue partial or entire motion/action as assisted practice is faded, OR sustained grasp once placed. 3 = Touch prompt and/or gesturing cue needed for her to initiate and complete at least part of a motion/action. 4 = Initiated: After physically assisted practice was stopped, she resumed same action and completed at least part, OR initiated part of a sequence of an action w/o physical cues. 5 = Initiated and completed the action independently, or used this skill to while performing another more complex functional action.
Table 7 describes the interplay between emerging milestones and the child’s active participation in ASI.
Emerging motor/praxis milestones and relationship to participation.

Discussion
Our in-depth analysis of treatment notes revealed important strategies that supported, as well as barriers that interfered with this child’s participation in ASI therapy. We observed the importance of using lateral movement activities to develop weight-shifting and bilateral coordination, rotary play to increase trunk rotation and improve postural transitions, and rhythm to promote continuing or initiating actions. By recording specific cues and least levels of assistance needed throughout treatment sessions, we were able to detect small but significant gains that would not be picked up by standard scales or checklists.
Central to ASI is the child’s active participation in all aspects of the intervention. In early sessions, this child’s active involvement was very limited due to severe dyspraxia—that is, her inability to initiate purposeful movement. The therapist had to passively move her through many actions to help her sample activities to determine activity choice, transition on and off equipment, and use her hands during play. The therapist applied motor learning theory by using tactile-proprioceptive input through passive practice motions to help the child feel the desired movements and develop a concept of the actions. This technique is commonly used by therapists in the treatment of children who have neuromotor dysfunction.32,34 In this case, for example, the therapist provided multiple opportunities to passively practice component skills of trunk rotation and weight shifting during postural transitions and functional play activities, that led to the gradual emergence of active, independent rotation and weight shifting, and increasing participation. (See Supplemental E Treatment Notes—Columns 3-6)
These hypotheses are supported by the following research studies of motor learning involving neurotypical individuals. Chiyohara et al 35 showed that passive movement of the upper extremity through desired motions enhances proprioceptive acuity of those movements and improves efficiency and accuracy of motor production when assistance is removed. Bernardi et al 36 demonstrated that passive movements paired with positive reinforcement facilitated learning new motor actions and can be useful in early stages of motor learning. Rosenkranz and Rothwell 34 demonstrated that sensory attention activities without motor output influence motor learning. In theory, these techniques increase somatosensory awareness and facilitate emerging ideation of the task 5 and planning of new motor actions.
Our coding identified that the treating therapist incorporated elements of NDT and motor learning theory into many of the early ASI therapy sessions. These are tactile-proprioceptive techniques often used by experienced therapists to facilitate active movement for children with neuromotor involvement. At the outset of the intervention period, limited and rigid trunk movements interfered with this child’s ability to participate in many of the activities integral to ASI. NDT handling techniques facilitated active weight-shifting and trunk rotation. Lateral and rotary movement activities on suspended/moving therapy equipment activated weight-shifting, trunk righting, and trunk rotation. These new core skills led to improved bilateral integration and active participation in postural transitions. As transitional movements became more automatic, she participated in ASI treatments with greater independence and confidence. Supplemental F demonstrates this progression.
This child’s over-responsivity to movement/vestibular sensations initially contributed to avoidance of postural changes and certain types of play. This was measured by clinical observations of physical reactions when the child’s balance was challenged such as when moving on therapy equipment– (Refer to Sensory Processing and Modulation column of the daily treatment note, Supplemental E). The therapist interpreted the following signs as over-responsivity: apprehensive facial expressions, increase in total body tension, distressed vocalization, strongly grasping therapist or equipment, and avoidance of specific play activities. The therapist respected the child’s body language and adjusted the activity accordingly. Over time, this child slowly accommodated to gradual increases in acceleration as well as movement in many different planes of 3-dimensional space while playing on suspension equipment. As behaviors associated with gravitational insecurity decreased, she began developing new adaptive responses and demonstrated greater enjoyment/participation in movement activities that she had initially avoided.37,38
Creating meaningful play experiences is central to ASI intervention. This is a challenge when treating children with significant communication issues and limited ability to interact with objects. While imaginative play can be very engaging for many children, this child was better motivated by concrete activities with highly preferred sensory attributes. Also, the therapist’s playful use of self, and strategic placement of highly preferred materials and toys, became meaningful and strong incentives for her to attempt challenging activities involving postural transitions, crawling, reaching, and grasping. For example, placing a favorite gel-squishy toy at the opposite end of the mat enticed her to crawl for the first time. Likewise, dangling a favorite toy at arms-length enticed her to reach for this target while riding on moving equipment. This led to reaching for objects with other less-preferred textures while both she and the object were moving, and suggests emerging ideation of a new motor task and projected action sequencing—both major sub-functions of praxis development. 39
The therapist’s use of rhythmicity through touch, voice/music/sound, and physical movement cues supported the child in 2 important ways. Rhythmic cues helped her anticipate the next step in motor sequences, such as when transitioning from floor-sit to standing. It also helped the child time her movements as the therapist faded or stopped physically assisted practice motions. Determining the timing of movement initiation is a critical process that precedes voluntary action. 40 Rhythmicity is an important element of praxis and integral to motor planning, bilateral motor coordination, and projected action sequences. 39
The therapist waited at least 30 seconds for the child to respond to a cue before repeating it. “Wait time” after cues is recommended for children with RTT, 25 and 30 seconds is prescribed in this child’s IEP. This strategy allowed her time to develop a concept of the task and to initiate a motor response.5,41 This often resulted in the child continuing or re-enacting motions to participate in some activities for the first time.
Critical elements of documentation provided important insights into this child’s response to treatment. Most existing assessment tools and checklists lack sensitivity to capture subtle changes that we might expect for a child with this complex condition. Table 3 outlines the key that the therapist used to record specific amounts of physical support and prompting needed to achieve optimal levels of participation. 33 This systematic recording revealed small changes over time in the child’s quality of movement, sensory processing, praxis, adaptive responses, and participation. It also informed the therapist on effectiveness of treatment/techniques and/or the need for change. This documentation method proved to be highly effective for detecting the many small steps that signaled emergence of new skills.
More significant responses to treatment occurred in proximal praxis (functional trunk movements) compared to distal praxis (functional reach and grasping) during this 36-session intervention. This may be a function of the neuropathology of RTT—hand stereotypies and signature loss of hand function—or may be related to normal developmental progression from proximal to distal. 42 It poses the question of whether more significant arm/hand function would have eventually emerged if the intervention period had been longer.
Strengths and limitations
The systematic and detailed recording of treatment notes from 36 hour-long sessions provided an in-depth description of how one child with RTT responded to ASI treatment. This analysis reveals the interplay between specific treatment strategies and the child’s emerging skills and goal attainment.
As with all analyses of individual cases, these observations are not generalizable to other children with RTT. Nevertheless, we believe that this rich qualitative data may generate important hypotheses for further research into this novel application of ASI for treating the severe dyspraxia associated with RTT.
An important limitation to our analysis is social desirability bias—one of the authors provided all ASI treatments and treatment documentation. To minimize this risk, all treatment notes were coded independently by 2 study authors with expertise in RTT and ASI, with strict adherence to all measures outlined in our methods.
Conclusions
The previous ASI study measured the efficacy of ASI to develop functional reaching and grasping in 5 children with RTT/Rett-related disorders. In this case report, we conducted a thematic analysis of treatment notes from one of the children who had a diagnosis of classic RTT, to better understand underlying mechanisms of that earlier quantitative study. The severity of this child’s dyspraxia, hand stereotypies, sensory processing issues, and cognitive and communication concerns created challenges, especially at the outset of the intervention. Our examination of these notes revealed strategies that promoted active participation in the ASI therapy process. It was through this coding that we discovered that elements of additional neuromotor treatment techniques contributed to this child’s participation, through development of active weight shifting, trunk rotation, and bilateral integration. This report identifies patterns and possible relationships between a combination of therapeutic techniques/activities and this child’s emerging praxis and active participation.
These observations and insights highlight the importance of careful, methodical recording of subtle responses to treatment so that therapists can adjust approaches and/or incorporate additional strategies, with the aim of maximizing treatment effectiveness. We discussed the importance of recording the hierarchy of prompting/cues that the child needs to produce adaptive responses. This systematic documentation of clinical observations captured subtle changes in praxis, function, and participation. We illustrated the novel use of ASI to treat severe dyspraxia of one child with RTT, with the hope that future research into its efficacy for this population will expand treatment options for others with this condition.
Supplemental Material
sj-docx-1-pdi-10.1177_11795565231188939 – Supplemental material for Ayres Sensory Integration Therapy for a Child With Rett Syndrome: A Case Report
Supplemental material, sj-docx-1-pdi-10.1177_11795565231188939 for Ayres Sensory Integration Therapy for a Child With Rett Syndrome: A Case Report by Karen Rocco, Wendy` Drobnyk, Susan Bruce and Stephen B Soumerai in Clinical Medicine Insights: Pediatrics
Supplemental Material
sj-docx-2-pdi-10.1177_11795565231188939 – Supplemental material for Ayres Sensory Integration Therapy for a Child With Rett Syndrome: A Case Report
Supplemental material, sj-docx-2-pdi-10.1177_11795565231188939 for Ayres Sensory Integration Therapy for a Child With Rett Syndrome: A Case Report by Karen Rocco, Wendy` Drobnyk, Susan Bruce and Stephen B Soumerai in Clinical Medicine Insights: Pediatrics
Supplemental Material
sj-docx-3-pdi-10.1177_11795565231188939 – Supplemental material for Ayres Sensory Integration Therapy for a Child With Rett Syndrome: A Case Report
Supplemental material, sj-docx-3-pdi-10.1177_11795565231188939 for Ayres Sensory Integration Therapy for a Child With Rett Syndrome: A Case Report by Karen Rocco, Wendy` Drobnyk, Susan Bruce and Stephen B Soumerai in Clinical Medicine Insights: Pediatrics
Supplemental Material
sj-docx-4-pdi-10.1177_11795565231188939 – Supplemental material for Ayres Sensory Integration Therapy for a Child With Rett Syndrome: A Case Report
Supplemental material, sj-docx-4-pdi-10.1177_11795565231188939 for Ayres Sensory Integration Therapy for a Child With Rett Syndrome: A Case Report by Karen Rocco, Wendy` Drobnyk, Susan Bruce and Stephen B Soumerai in Clinical Medicine Insights: Pediatrics
Supplemental Material
sj-docx-5-pdi-10.1177_11795565231188939 – Supplemental material for Ayres Sensory Integration Therapy for a Child With Rett Syndrome: A Case Report
Supplemental material, sj-docx-5-pdi-10.1177_11795565231188939 for Ayres Sensory Integration Therapy for a Child With Rett Syndrome: A Case Report by Karen Rocco, Wendy` Drobnyk, Susan Bruce and Stephen B Soumerai in Clinical Medicine Insights: Pediatrics
Supplemental Material
sj-docx-6-pdi-10.1177_11795565231188939 – Supplemental material for Ayres Sensory Integration Therapy for a Child With Rett Syndrome: A Case Report
Supplemental material, sj-docx-6-pdi-10.1177_11795565231188939 for Ayres Sensory Integration Therapy for a Child With Rett Syndrome: A Case Report by Karen Rocco, Wendy` Drobnyk, Susan Bruce and Stephen B Soumerai in Clinical Medicine Insights: Pediatrics
Supplemental Material
sj-docx-7-pdi-10.1177_11795565231188939 – Supplemental material for Ayres Sensory Integration Therapy for a Child With Rett Syndrome: A Case Report
Supplemental material, sj-docx-7-pdi-10.1177_11795565231188939 for Ayres Sensory Integration Therapy for a Child With Rett Syndrome: A Case Report by Karen Rocco, Wendy` Drobnyk, Susan Bruce and Stephen B Soumerai in Clinical Medicine Insights: Pediatrics
Supplemental Material
sj-jpg-8-pdi-10.1177_11795565231188939 – Supplemental material for Ayres Sensory Integration Therapy for a Child With Rett Syndrome: A Case Report
Supplemental material, sj-jpg-8-pdi-10.1177_11795565231188939 for Ayres Sensory Integration Therapy for a Child With Rett Syndrome: A Case Report by Karen Rocco, Wendy` Drobnyk, Susan Bruce and Stephen B Soumerai in Clinical Medicine Insights: Pediatrics
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.