
Abstract
Xanthogranulomatous inflammation is a rare, destructive pattern of inflammation, affecting different organs, that often produces a mass-like lesion, simulating malignancy. Although benign, it can coexist with malignancy. We, herein, report the case of a 60-year-old male patient, who presented with a testicular mass that was partly necrotic and showed heterogeneous enhancement on contrast study. Testicular tumor markers were normal. In view of clinicoradiological suspicion of a malignant cause, high inguinal orchidectomy was performed. However, histopathology showed features of a xanthogranulomatous orchitis with no evidence of any malignancy. Pathologists must be aware of this entity as definitive diagnosis requires histopathologic examination and adequate sampling must be done to rule out a coexistent malignancy.
Introduction
Xanthogranulomatous inflammation is a non-neoplastic, inflammatory disease, commonly affecting the kidney and gall bladder. However, it can also affect the liver, appendix, ovaries, vagina, bones, and urinary bladder. 1 It can rarely affect the prostate, epididymis, and testicle. Involvement of the testicles by xanthogranulomatous inflammation is rare and exact pathogenesis remains unknown. 1 Furthermore, xanthogranulomatous orchitis (XGO) mimics a testicular malignancy clinically as well as radiologically; pathological examination is essential for a confirmation and thorough histological examination is needed to rule out any coexistent malignancy. 2
Case Report
A 60-year-old, hypertensive, male patient presented with chief complaint of gradually increasing swelling of the left scrotum for 1 year. It was not associated with pain, weight loss, loss of appetite, urinary symptoms, or history of testicular trauma. The patient never had a complaint of sudden, severe pain in the scrotum and no history of chronic leg or chest pain. On examination, there was a non-tender left testicular mass with a variegated consistency and normal right testis.
Tumor markers were not raised and scrotal ultrasound revealed a large diffuse heteroechoic mass in the left hemiscrotum, measuring 10.9 × 9.8 × 9.7 cm3 with areas of calcification and cystic change (Figure 1). Contrast-enhanced computed tomography (CECT) showed similar findings in the left hemiscrotum with moderate heterogeneous enhancement on contrast study (Figure 2). Right hydrocele was noted with a normal-appearing right testis and epididymis. Rest of the organs appeared to be normal with no significant lymphadenopathy and no evidence of free fluid in the peritoneal cavity.

Left scrotal ultrasound image where fluid-filled cystic areas are black foci (arrow) interspersed within the white solid mass.

Contrast-enhanced computed tomography of the pelvis showing a large diffuse heterodense mass lesion in the left scrotum with heterogeneous enhancement (arrow) on contrast study.
With a provisional diagnosis of a testicular tumor, the patient underwent high inguinal orchidectomy procedure. Intraoperatively, a left testicular necrotic tumor-like lesion was identified, measuring 15 × 8 × 6 cm3. The mass ruptured inadvertently during surgery and 150 mL of serohemorrhagic fluid was drained.
Grossly (Figure 3), the specimen of high inguinal orchiectomy weighed 560 g and measured 13 × 9 × 5 cm3. The testis was enlarged and showed complete loss of normal architecture with replacement by cystic, necrotic, solid gray-white to bright yellowish areas and foci of calcification.
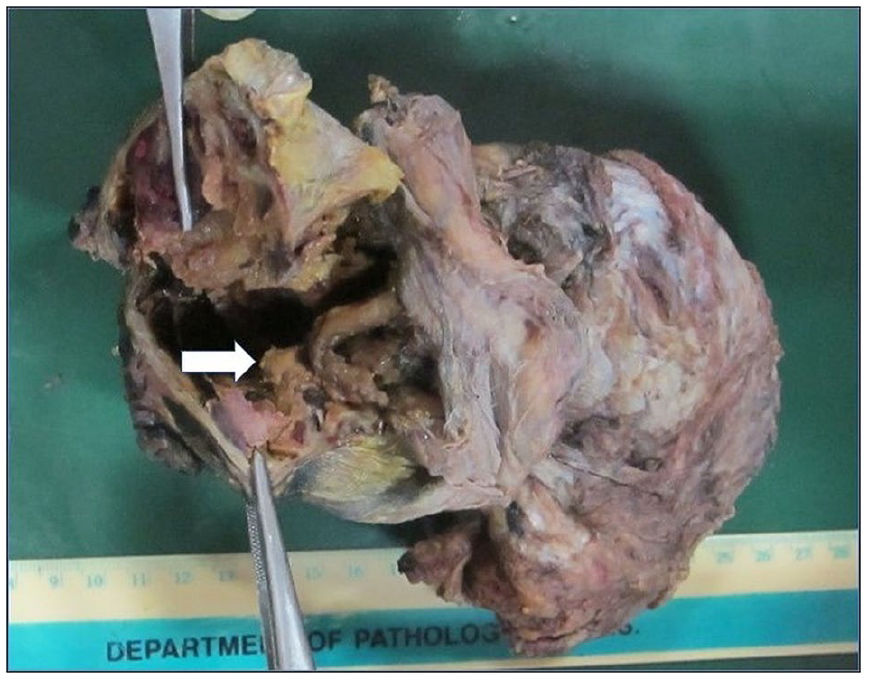
Specimen of the left testis showing a large solid, cystic mass with foci of yellowish discoloration (arrow).
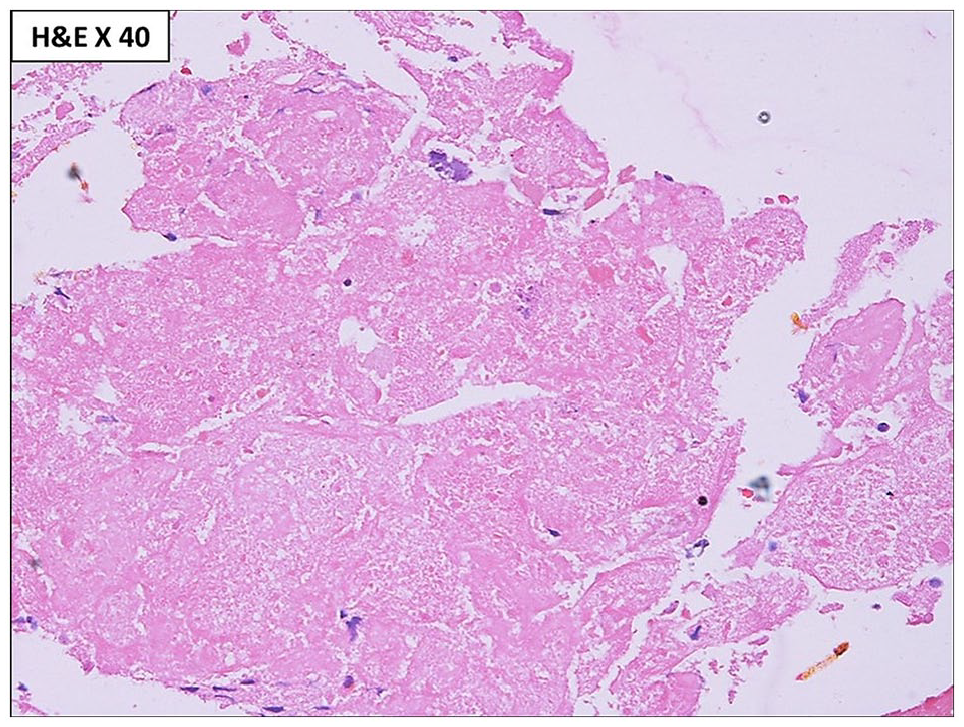
Microscopy showed complete replacement of the testicular parenchyma by diffuse sheets of histiocytes and giant cells with areas of old hemorrhage, suggestive of xanthogranulomatous inflammation (Figure 4). A cystic change containing necrotic debris was identified (Figure 5). Asteroid bodies were noted in the cytoplasm of most of the giant cells (Figure 6). The xanthomatous histiocytes and giant cells were immunoreactive for CD68 (Figure 7). There was no evidence of Michaelis-Gutmann bodies within the cytoplasm of the cells, thereby ruling out close differential diagnosis of malakoplakia. Special stains (Giemsa, Ziehl-Neelsen, Periodic acid Schiff, and Grocott methenamine silver) did not reveal any microorganism.

Photomicrograph showing diffuse sheets of histiocytes (small arrow) and giant cells (big arrow).
Necrotic material was identified in cyst contents.
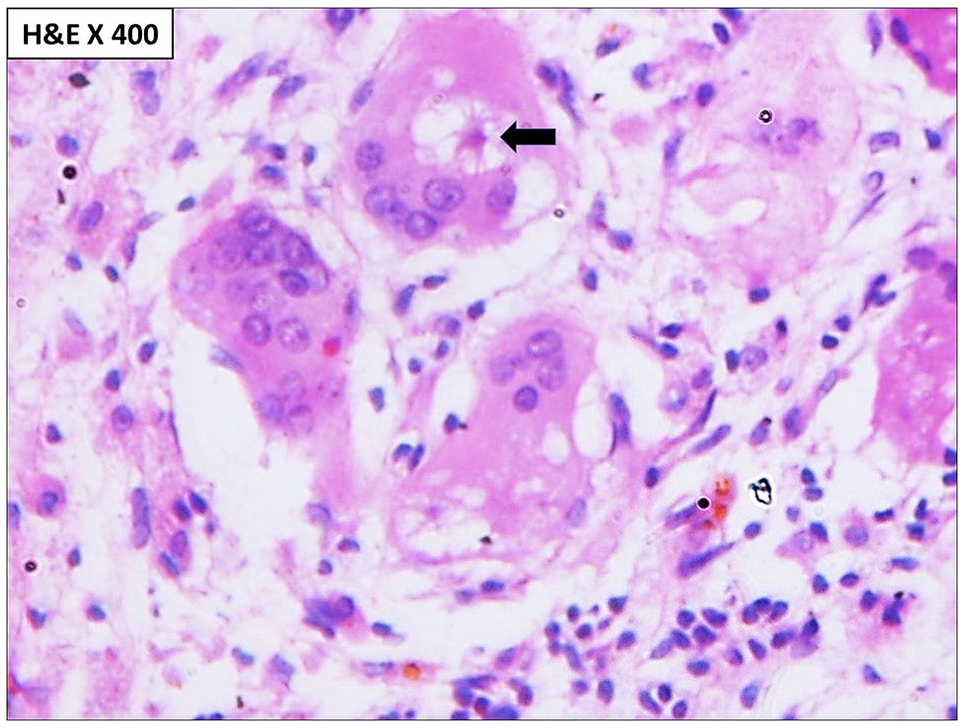
Asteroid bodies (arrow) seen in the cytoplasm of giant cells.

The mononuclear as well as giant cells show diffuse and strong immunopositivity for CD68, suggestive of histiocytic origin.
Discussion
General epidemiology and clinical presentation
Xanthogranulomatous orchitis is an extremely rare inflammatory lesion that presents as a mass with or without pain. It has a wide age range of distribution. The youngest case of xanthogranulomatous orchiepididymitis and funiculitis reported in the medical literature is that of a 13-year-old adolescent boy who presented with a painless left hemiscrotal swelling. 3
The pathogenesis of this entity is not well established; however, multiple factors leading to xanthogranulomatous orchiepididymitis have been hypothesized by different authors. Obstruction of epididymis or urinary obstruction is among the prominent factors. 4 Xanthogranulomatous orchitis has also been reported to occur due to testicular ischemia secondary to atherosclerosis in elderly patients and endarteritis or endophlebitis in younger patients. 2 The index patient does not have history of testicular torsion or obstructive uropathy. Urinary tract infection has also been implicated as an etiological factor. 2 There are few case reports of XGO where Escherichia coli and Pseudomonas aeruginosa were cultured. 5 However, identification of an infective microorganism may be difficult as this is a chronic inflammatory process. Past history of urinary tract infection cannot be ruled out in the index case which may have led to XGO.
Malnutrition, abnormal lipid metabolism, and lipid accumulation in macrophages are the other rare contributing factors. 1 Xanthogranulomatous inflammation may also occur as a local response to tumor. 1 It has been reported to occur after blunt testicular trauma. 6 There were no testicular trauma, abnormal lipid metabolism, and any associated tumor in the current case.
Differential diagnosis
Differential diagnosis of XGO includes testicular tumor, infectious epididymo-orchitis, malakoplakia, Rosai-Dorfman disease, lepromatous orchitis, and idiopathic granulomatous orchitis.1,7 Malakoplakia is an uncommon granulomatous process of the testis, characterized by accumulation of macrophages with granular and eosinophilic cytoplasm. These macrophages contain characteristic intracytoplasmic inclusions known as Michaelis-Gutmann bodies. 8 Rosai-Dorfman disease of the testis is an inflammatory lesion consisting of lymphocytes, plasma cells, and sheets of pale staining histiocytes which show emperipolesis. 9 Emperipolesis is a process, in which a cell penetrates another living cell and exists as a viable cell within another. No structural or functional abnormalities are caused to either of them during the process. 10 Lepromatous leprosy can have orchitis as the initial presention. 11 Histology reveals atrophied and hyalinized seminiferous tubules with interstitium showing infiltration by foamy macrophages that contain intracellular acid-fast bacilli.
Xanthogranulomatous orchitis may coexist with a testicular malignancy. Val-Bernal et al 7 reported a case of XGO and a concurrent, occult typical seminoma. Hence, histopathologic examination is important and is the only conclusive evidence to rule out malignancy and to diagnose xanthogranulomatous inflammation. Extensive sampling of the orchidectomy specimen is recommended to exclude an occult germ cell tumor that has been done in this case. Burnout seminomas or seminomas with a prominent granulomatous reaction may be misinterpreted as idiopathic granulomatous orchitis. In such cases, the residual seminiferous tubules must be examined for unclassified intratubular germ cell neoplasia. 7 Furthermore, immunostaining for placental alkaline phosphatase (PLAP), CD117, and OCT3/4 may help by highlighting residual tumor cells obscured by inflammation. In the index case, the testicular mass was extensively sampled and sections were examined which ruled out the possibility of occult germ cell tumor with extensive granulomatous response.
The distinction between an inflammatory and a neoplastic cause is difficult. There is no specific pattern on ultrasound and magnetic resonance imaging that can allow a specific diagnosis. 7 Hence, histopathology of the resection specimen is gold standard for confirmation.
Management
Orchidectomy is curative due to wide tissue destruction seen in XGO. 7
The role of antibiotic treatment is a matter of debate because most cases end up with loss of the affected organ. Transinguinal orchiectomy should be the operative procedure of choice if the scrotum is intact. If testicular abscess or scrotal discharging sinuses are present, then the scrotal approach for orchiectomy combined with hemiscrotectomy is preferred. 2
Conclusions
Xanthogranulomatous orchitis, although a rare diagnostic entity, is clinically significant as it closely resembles malignancy clinicoradiologically and may even coexist with it. Clinicians must be aware of this mimicker before planning any radical operative procedure, whereas pathologists must be aware of its notoriety in masking an underlying testicular tumor. A comprehensive work-up involving adequate history, thorough clinical examination, radiological investigation, and serum biochemistry for tumor biomarkers is important to provide clues; however, pathological examination is imperative for a conclusive diagnosis and to rule out any occult germ cell tumor.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
PR and PS: Manuscript writing and case analysis; AS: Case work-up; MDR: Case work-up and analysis.
Informed Consent
Informed patient consent to publish the case study has been obtained.