
Abstract
Testicular tumors are rare in children, accounting for only 1% to 2% of pediatric solid tumors. Mature teratomas (MTs) are a benign subtype that typically occur in prepubertal boys and may occasionally mimic hydroceles. We report a case of a 3-year-old boy with left testicular swelling initially suspected to be a hydrocele. Over several months, the swelling evolved into a firm, painless mass. Ultrasound and MRI revealed a multiloculated cystic lesion with internal vascularity replacing most of the testicular parenchyma. Serum tumor markers, including alpha-fetoprotein, β-human chorionic gonadotropin, and lactate dehydrogenase, were within normal limits. The patient underwent left inguinal orchiectomy, and histopathology confirmed a MT without immature or malignant elements. Postoperative recovery was uneventful. He underwent routine follow-up every 3 months for 2 years, including physical examinations, scrotal ultrasounds, and serum tumor marker assessments. Findings from the first and second follow-ups were normal, with no evidence of recurrence to date. This case underscores the importance of early imaging and tumor marker evaluation in children presenting with persistent scrotal swelling. A systematic diagnostic approach facilitates accurate diagnosis, and orchiectomy remains the standard treatment for prepubertal MTs.
Introduction
Testicular tumors are uncommon in children, occurring in ~0.5 to 2/100 000 males and representing 1% to 2% of all pediatric solid tumors, with a peak incidence around 18 months of age. 1 The most common testicular tumors are germ cell tumors, which include seminomas, yolk sac tumors, teratomas, and others. Teratomas account for about 13% of all pediatric testicular tumors. 2 There are 3 forms of teratomas: monodermal, immature, and mature, which are typically benign and account for about 48% of prepubertal testicular tumors.1,3
In general, teratomas are more common in females, occurring in the ovarian or sacrococcygeal regions, while in males, they arise within the testis and are relatively uncommon. 1 The etiology of teratomas is poorly understood, but known risk factors include cryptorchidism and disorders of sex development. 4
Clinically, testicular teratomas usually present as painless, unilateral swelling. These tumors can cause different complications depending on the affected organ and are usually discovered incidentally during clinical examination, imaging, or during an operation for the abdomen. They may mimic other benign scrotal conditions such as hydroceles, leading to frequent misdiagnosis, particularly in early or atypical cases. This was the case in our patient.2,4
The primary treatment for this tumor is surgical removal, often by orchiectomy or testis-sparing surgery, depending on tumor size and benign features—detailed discussion follows later.1,5 Here, we present a case of mature testicular mature teratoma (MT) found in a 3-year-old boy, presenting as a scrotal swelling that clinically mimicked a hydrocele.
Case Presentation
A 3-year-old male child was referred to the pediatric urology clinic for evaluation of a left testicular swelling. The swelling was first noticed incidentally during a routine pediatric check-up at 18 months of age. It was asymptomatic, without palpable mass, discoloration, fever, genitourinary, or bowel complaints. Based on clinical findings, it was initially suspected to be a simple hydrocele, and the family was advised to continue observation with periodic follow-up. The patient has had no significant past medical history since birth, with no history of cryptorchidism. There is no family history of malignancy. He was born via an uncomplicated vaginal delivery, and his growth and developmental milestones have been normal.
Over the following months, the swelling remained stable and did not exhibit any sudden increase in size. However, when re-evaluated by a urology specialist, physical examination revealed a firm, nontender mass in the left testis. The overlying scrotal skin was normal in color and temperature, and no signs of inguinal hernia or contralateral involvement were found.
Scrotal Doppler ultrasonography demonstrated a thick-walled, septated, multiloculated left testicular mass, measuring ~2.3 × 2 × 2 cm, with no specific characteristics. The right testicle was unremarkable. A subsequent MRI was performed and shows a homogeneous cystic mass with fluid signal intensity (low signal intensity on T1, high signal intensity on T2 and T2-FS; Figure 1). The mass originated from the left testicle, occupying most of its parenchyma, with no local invasion or malignant-appearing lymph nodes. It shows avid enhancement of the mural nodule postcontrast administration (Figure 2). No abnormalities were noted in the right testicle, epididymis, or spermatic cord.
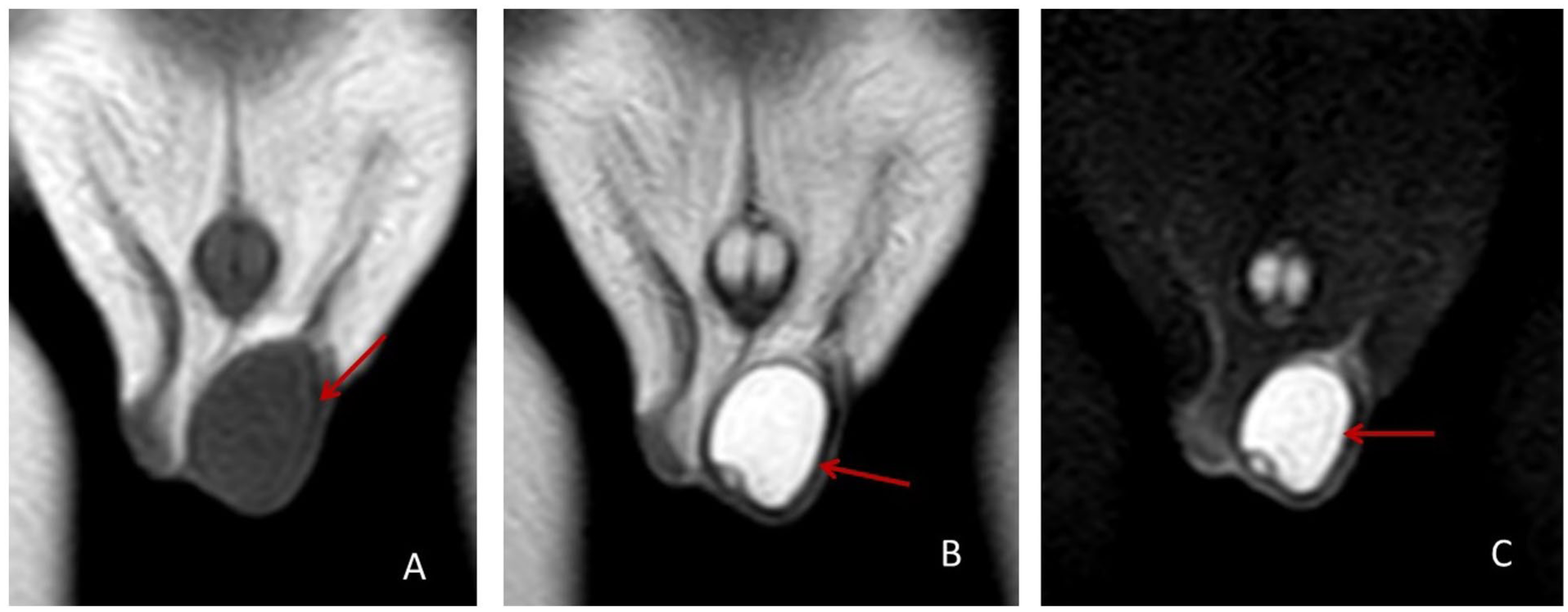
T1 (A), T2 (B), and T2-FS (C) coronal MRI shows left testicular loculated cystic mass (red arrows).

T1 postcontrast ((A) coronal view and (B) axial view), shows mural enhancing nodule (red arrow).
Laboratory evaluation included serum human chorionic gonadotropin (β-HCG) was negative, lactate dehydrogenase was 402 U/L, and alpha-fetoprotein (AFP) was 2.72 IU/ml. All of which were within normal limits for age. Complete Blood Count (CBC) and biochemistry panels showed no significant abnormalities. Due to the suspicious nature of the lesion and the potential risk of malignancy, surgical management was planned. The patient underwent left inguinal orchiectomy, and a sample was taken for histopathological examination. Histopathological evaluation of the biopsy confirmed the diagnosis of mature testicular teratoma. There was no evidence of immature elements or other germ cell components or malignancy. The postoperative course was uneventful. The patient was discharged 1 day after surgery and scheduled for routine follow-up every 3 months for 2 years. Regular physical examinations, scrotal ultrasounds, and assessments of serum tumor markers were all part of the follow-up protocol. Blood tests, echocardiography, and ultrasound were performed at the 3-month follow-up, all yielding normal results. Findings from the second follow-up were similarly unremarkable. To date, there has been no evidence of recurrence or contralateral involvement.
Discussion
Prepubertal MTs are benign germ cell tumors composed of well-differentiated tissues of at least 2 of the 3 embryonic germ layers: ectoderm, mesoderm, and endoderm. 6 These tumors are the most common benign testicular neoplasm in children under the age of 4 and represent a significant portion of pediatric testicular masses. They also exhibit distinct clinical and biological behaviors compared to their postpubertal counterparts, which are frequently associated with malignant germ cell tumors. In contrast, MT in prepubertal patients generally follows a benign course.7,8
The diagnostic approach is based on a detailed clinical examination and advanced imaging. Ultrasonography is the initial and most crucial modality, providing essential details on tumor size, cystic components, and architecture to aid in differentiating benign from malignant lesions. 7 If ultrasound is inconclusive, MRI can provide greater detail on tumor margins and their relationship to adjacent structures. 9 It’s crucial to check serum tumor markers; in MTs, AFP and β-HCG are typically normal, which helps distinguish them from many malignant germ cell tumors. 10
An important step in the diagnosis is to consider the differential diagnosis of prepubertal scrotal masses. Clinically, it can be difficult to differentiate a MT from other benign masses in children, like a hydrocele or epidermoid cyst. Because the presentation can sometimes be atypical, a high index of suspicion is essential to prevent misdiagnosis and delays in treatment.4,11 Other conditions that must be ruled out include testicular torsion, epididymitis, and inguinal hernia, all of which can present as a scrotal mass or swelling. 7
Surgery is the definitive treatment. Historically, radical inguinal orchiectomy was the standard approach to ensure complete tumor resection and prevent scrotal contamination. However, due to a better understanding of the tumor’s benign pathology and advancements in imaging, testis-sparing surgery is becoming an increasingly favored option in carefully chosen cases, particularly for small, localized lesions with normal tumor markers. 5 Histopathological examination of the excised specimen is ultimately crucial to confirm the diagnosis and rule out any hidden malignant components.6,8
In the present case, orchiectomy was performed because imaging showed that the lesion occupied most of the testicular parenchyma, leaving minimal viable tissue for preservation, and malignancy could not be confidently excluded preoperatively. As summarized by Kooij et al, 12 radical inguinal orchiectomy remains recommended for large or indeterminate testicular masses, while TSS is appropriate when the lesion is small, tumor markers are normal, and intraoperative frozen section is available.
After surgery, the prognosis for these patients is excellent, with a minimal risk of recurrence or malignant transformation. Consequently, adjuvant chemotherapy or radiotherapy is not indicated unless there is evidence of rare malignant change. Long-term follow-up involves a surveillance protocol consisting of regular physical exams, periodic imaging, and tumor marker monitoring to detect any new or recurrent disease. 10 Given the rarity and benign pathology of these tumors, a multidisciplinary team approach involving pediatric urologists, oncologists, radiologists, and pathologists is essential for providing optimal individualized care.6,8
Conclusion
This case underscores the importance of high clinical suspicion for persistent scrotal enlargement in pediatric age. Employing systematic evaluation—including physical examination, imaging, tumor marker analysis, and timely surgery—ensures diagnostic accuracy. Recognizing the benign nature of prepubertal MTs guides appropriate therapy, preventing overtreatment, and optimizing patient outcomes.
Footnotes
Acknowledgements
The authors thank the Polytechnic Medical Students’ Research Association (PMRA) for their invaluable input and support throughout the research process.
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to Participate
Written informed consent was obtained from the patient to participate in the clinical evaluation and management described in this case report.
Consent for Publication
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.