
Abstract
A 45-year-old man visited our clinic with a painless swelling of the left scrotum and an ulcer as chief complaints. A hard and indurated mass was palpable with ulcerating foci that were proximal and distal, measuring 3 × 2 cm and 2 × 1 cm respectively and about 2 cm apart. Laboratory data were normal except for an elevated erythrocyte sedimentation rate (ESR), and white blood cell (WBC) differential showed neutropenia and lymphocytosis. A diagnosis of left testicular tumor was made and the patient had a left orchidectomy with fistulectomy. Histopathology results showed a stratified squamous epithelium with tuberculous granuloma and necrotic caseation. Patient is currently on anti-tubercular medication. The rarity of this condition makes these findings important to report.
Introduction
Most people think of tuberculosis as affecting only the lungs, but in reality it affects almost every part of the body. Pulmonary tuberculosis (TB) is most common type, accounting for about 70% of cases. Sometimes, pulmonary TB will spread, though this usually happens only in immune-suppressed patients and young children.
Dissemination of TB to the testis may result in secondary infection of epididymis. In many of these cases, there is associated tuberculous prostatitis and seminal vesiculitis, and it is believed that epididymitis usually represents a secondary spread from these other involvements of the genital tract.1,2 The result is great thickening and the formation of a caseous mass. Caseous masses are very dense, but after a certain amount of time they generally breakdown, and, having burst externally, result in tedious fistulae. When mycobacterium tuberculosis (MTB) droplet nuclei are inhaled, they go to the alveoli where they are taken up by phagocytosis into air-space macrophages. Here the bacilli are processed into phagosomes that fail to acidify. The bacilli evade intracellular killing and can therefore survive and multiply for long periods of time. These infected macrophage carry viable bacilli in the lymphatics to regional lymph nodes or in the blood stream to any part of the body. Disseminated tuberculosis spreads haematogenously when blood vessels erode into blood vessels. The disseminated tubercles appear like millet seed in various organs (for example, liver, spleen, kidneys, brain meninges, bone marrow and other tissues). Reactivation of TB in later years can occur as a result of reactivation of viable bacilli (quiescent or dormant tubercle), which have persisted within nodes. On histology, areas of granuloma and caseous necrosis are seen.
Case Presentation
A 45-year-old car spare parts dealer presented to the Abnira medical centre with a five-year history of left scrotal swelling and a two-week history of left scrotal ulcer. The swelling, which had being increasing in size, regressed some months before presentation and became hardened with ulcerated foci some weeks after. There was a history of contact with persons with pulmonary TB in the past, for over a year.
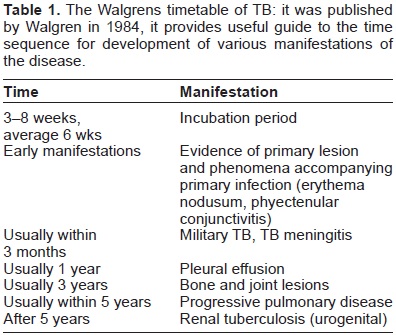
The Walgrens timetable of TB: it was published by Walgren in 1984, it provides useful guide to the time sequence for development of various manifestations of the disease.
On examination, he was not in obvious painful distress, not pale, anicteric, afebrile, not dehydrated, and had no obvious weight loss. His pulse rate was 80/minute and regular with full volume, and his blood pressure was 120/80 mmHg. Heart sounds were 1st and 2nd only, his respiratory rate was 14 cycles per minute and both lung fields were clear. The abdomen was full, moved with respiration with no palpably enlarged abdominal mass, and kidneys were not ballotable.
The right scrotum was normal whereas the left was swollen with two foci of discharging ulcer, with a proximal focus of 3 cm × 2 cm and a distal focus of 2 cm × 1 cm. The foci were approximately 2 cm apart. On palpation, the area was found to be non-tender, hard, able to go above the mass, not attached to the overlying skin, and not transilluminable.
The laboratory data showed an elevated erythrocyte sedimentation rate (ESR) of 40 mmfall/hr. Full blood count (FBC) showed a hemoglobin (Hb) of 12.3 g/dL, a white blood cell count (WBC) of 3,250 cells/mm, 3 and platelets of 259000 with a WBC differential showing 28 neutrophils, 69 lymphocytes, 1 monocyte, 2 eosinophils, and 0 basophils. Blood film showed reactive lymphocytes +++, toxic granulation ++, macrocytes ++, microcyte +, neutropenia, lymphocytosis, hypochromasia, and platelets to be adequate and normal. Swab microscopy culture and sensitivity (M/C/S) yielded a growth of the staphylococcus species after a 24-hour incubation at 37 °C, sensitive to gentamicin, levofloxacin and sparfloxacin. Chest x-ray, spinal x-ray, urea, electrolyte, creatinine and liver function tests were found to be normal. Retroviral screening and venereal Disease Research Laboratory (VDRL) tests were non-reactive.
An assessment of left testicular tumor was made and the patient was prepared for left orchidectomy (after obtaining an informed consent). At surgery, a tract was found connecting the proximal and distal ulcer foci. Fistulectomy and Orchidectomy.
The histological findings of the excised left testis were: macroscopic description (A): SCO soft-to-firm testicular tissue measuring 7 × 5 × 3 cm and weighing 57 g, with a cut section showing a mass of 4 cm diameter and 3 k. (B): SCO a skin tissue measuring 3 × 3 × 2 cm and weighing 8 g, with a cut section showing a grayish surface.
Microscopy: Testicular tissue showed stratified squamous within the stroma, several granuloma and extensive caseous necrosis. The histological diagnosis was tuberculosis.
Anti-tuberculosis chemotherapy was subsequently initiated. Three months after surgery, recurrence has not been found.
Discussion
Tuberculosis (formerly known as consumption, pthisis, or ‘wasting’) is an infectious disease caused by the bacillus mycobacterium tuberculosis. M. tuberculosis infects about one third of the world population and kills about three million patients each year and so is the single most important infectious cause of death on Earth. 3 There has being a dramatic increase in TB in the world and especially in Africa due to the emergence of Acquired Immune Deficiency Syndrome (AIDS). 3 The primary phase of M.TB infection begins with inhalation of the mycobacterium and ends with a T cell-mediated immune response that induces hyper-sensitivity to the organisms and controls 95% of infections. In secondary and disseminated TB, some individuals become re-infected with mycobacterium or reactivate dormant disease, or they progress directly from the primary mycobacterium lesion into disseminated disease. Following M.TB infection, 5%–10% of people will develop the active disease while more than 90% of M.TB infections do not result in disease in an individual's lifetime. 4 Primary disease occurs soon after the primary infection in the context of a naïve immune system, and the bacilli multiply and spread. Primary disease commonly occurs in the lungs and then disseminates to multiple sites, resulting in TB meningitis and miliary TB. Post-primary disease occurs long after primary infection in the context of a sensitized immune system, either as reactivation of a latent infection, or as a result of re-infection with a new strain. This may be because the strain of mycobacterium is particularly virulent or the host is particularly susceptible.

Section of the testis showing granulomatous and necrotic foci.
This patient had no history of chronic cough or weight loss; however, he had a history of drenching night sweats for over a year, with a positive history of contact with a person with pulmonary tuberculosis for over a year. He neither smoked nor worked in a place that would predispose him to such a disease.
In a reported case from Japan by Sensaki and colleagues in 2001, 5 it was shown that the presentation and findings of tuberculosis of the testis were similar to those reported here, other than the fact that we were unable to do a computerized tomography scan (CT-scan), beta-human chorionic gonodotropin (hcG) or magnetic resonance imaging (MRI).
In the absence of a histologic finding, the diagnosis of TB testis may be impossible. Patients with testicular masses should be fully investigated pre-operatively and post-operatively in order to increase the diagnostic index of this condition.
Conclusion
Although it is a very rare disease, the clinician should consider tuberculosis of the testis as a possible differential of a scrotal mass. This will increase the possibility of early diagnosis, as well as proper and early management.
Author Contributions
Conceived and designed the experiments: AIS. Analysed the data: AIS. Wrote the first draft of the manuscript: AMR. Contributed to the writing of the manuscript: CBU, RMM. Agree with manuscript results and conclusions: AIS. Jointly developed the structure and arguments for the paper: AIS, AMR, CBU, RMM. Made critical revisions and approved final version: AIS. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.