
Abstract
An aortoesophageal fistula (AEF) is a rare but often fatal complication associated with the placement of an aortic stent graft such as those utilized in thoracic endovascular aortic repair (TEVAR) procedures. Definitive surgical repair of AEF is the treatment of choice, as conservative management is nearly always fatal. We present the case of an AEF in a 74-year-old male managed by a unique treatment method; an esophageal stent was deployed to cover the fistula as a temporizing measure prior to definitive surgical correction, thus allowing time for resuscitation and hemodynamic optimization. The use of esophageal stents in the setting of AEF following TEVAR has been previously reported in the literature as a palliative measure for patients deemed incapable of tolerating open repair surgery. Our case demonstrates a new and innovative approach to the management of AEF following TEVAR in which the use of esophageal stenting is expanded beyond the role of palliative care and should be considered as a means to optimize at-risk patients prior to definitive corrective surgery in the hopes of improving outcomes.
Introduction
An aortoesophageal fistula (AEF) is a rare but life-threatening cause of upper gastrointestinal bleeding that results from a communication between the esophagus and aorta. Etiologies include foreign body ingestion, malignancy, infection, and thoracic aortic aneurysms. 1 Rarely a fistula results after placement of an aortic stent graft, such as those utilized in thoracic endovascular aortic repair (TEVAR) procedures.1,2 Although less invasive than an open repair, TEVAR carries its own morbidity and mortality due to the risk of unanticipated complications. 2 Aortoesophageal fistula is a rare but often fatal complication occurring in 1.9% of TEVAR procedures. 2
We present a case of an AEF in a 74-year-old male managed by a unique treatment method whereby an esophageal stent was deployed covering the fistula as a temporizing measure prior to definitive surgical correction allowing time for optimization. Written authorization was obtained from the patient prior to publication of this case.
Case Description
A 74-year-old male with a past medical history significant for chronic obstructive pulmonary disease, cerebral vascular accident, hypertension, peripheral vascular disease, and type 2 diabetes mellitus presented to the emergency department with hematemesis versus hemoptysis 2 months after undergoing emergent TEVAR for a ruptured thoracic aortic aneurysm. A computed tomography (CT) angiogram illustrated an AEF.
The patient was admitted to our Surgical Intensive Care Unit (SICU) and resuscitated, then the patient was promptly taken to the operating room for flexible bronchoscopy and esophagogastroduodenoscopy (EGD). Bronchoscopy was negative for endobronchial lesions in all lung lobes. On endoscopy, a large thrombus was noted in the mid-esophagus and significant blood was present in the stomach. Following irrigation and suction, no active bleed was discovered in the stomach, and attention was given to the large esophageal thrombus believed to represent the connection to the aorta. The vascular surgery team who placed the initial endograft was consulted, and the decision was made to stent the esophagus as a temporizing measure to tamponade the fistula. Fluoroscopy was utilized to measure the length of the thrombus to determine the size of the stent needed to fully cover the area. The large clot measured around 5 cm, extending from the level of about 30 cm from the incisors to 35 cm. In order to ensure that the entire defect was completely covered, a 15-cm stent was chosen. The area was delineated with radiopaque markers, and under direct vision, a guidewire was placed through the endoscope which remained in the esophagus. Under fluoroscopic guidance, the 15 cm stent was deployed, extending above and below the region of the thrombus.
The interim between esophageal stent placement and definitive surgical repair allowed adequate time for medical resuscitation and optimization of the patient’s condition. Seven days after esophageal stent placement, the patient returned to the operating room for definitive surgical repair of the AEF including left muscle-sparing thoracotomy, partial esophagectomy and high cervical esophagostomy, and resection of the infected thoracic aortic stent graft under femoral-femoral cardiopulmonary bypass. The thoracic aorta was reconstructed utilizing a rifampin soaked 24 mm × 30 cm gel weave tube graft. The surgery was completed without complication and the patient tolerated the procedure well.
Post-operatively, the patient was transitioned to enteral feeds via a J-tube. IV ampicillin-sulbactam was given for 6 weeks after tissue cultures grew Enterococcus faecalis. After a 22-day hospital course, the patient was discharged to a skilled nursing facility for further rehabilitation.
Discussion
The incidence of AEF following endovascular repair of the aorta has been reported to range from 1.7% to 1.9%, although this rate is expected to rise as TEVAR continues to be an increasingly utilized alternative to open surgery for emergent treatment of aortic conditions.2–4 Fistula formation usually occurs within 1 to 16 months following the original TEVAR procedure. 2 The definitive mechanism by which fistula formation occurs has not yet been elucidated. Possible mechanisms that have been hypothesized include erosion of the stent graft through the aorta, endoleaks into the residual aneurysm sac, pressure necrosis on the esophageal wall due to progressive expansion of the endograft, and ischemic necrosis of the esophageal wall secondary to the stent graft compressing aortic vessels that supply the esophagus.2,3
The classic presenting symptoms of an AEF have been described as the triad of mid-thoracic chest pain, sentinel hemorrhage with a small episode of hematemesis followed by a brief interval period, and eventual massive hematemesis and exsanguination.5,6 Constitutional signs and symptoms such as new onset fever, fatigue, anorexia, and elevated inflammatory markers are also commonly associated with this condition.2,6 Aortoesophageal fistula should be considered early and often in the differential for a patient with a history of TEVAR presenting with any of the aforementioned symptoms. Although many potential causes of hematemesis exist, AEF must be ruled out first in a patient with history of TEVAR before other causes can be entertained. 6
Early recognition and management is critical, as conservative treatment is not a viable option. Both endovascular and open surgical management carry a 64% risk of mortality. 3 Once an AEF is suspected, imaging studies should be conducted for definitive diagnosis. The most commonly utilized imaging modalities to investigate for AEF include contrast-enhanced CT and EGD.
Contrast-enhanced CT is a readily available modality that not only assists in identifying AEF but also may reveal other graft-stent abnormalities such as infection or endoleak. 6 In our patient’s case, the presence of an AEF was detected incidentally due to the presence of gas within the aneurysm sac and loss of the fat plane between the esophagus and the aorta on a CT angiogram. Esophagogastroduodenoscopy is another important diagnostic tool, allowing direct visualization of the esophagus and location of the fistula. It also provides a valuable means for investigating alternative causes of gastrointestinal bleeding, such as malignancy or peptic ulcer disease. 6 In our case, a large thrombus located at the communication between the mid-esophagus and aorta was observed on EGD. The stomach was also visualized, suctioned, and irrigated to definitively rule out alternative sources of bleeding. Somewhat unique to our case, bronchoscopy was also performed as an adjunct to contrast-enhanced CT and EGD. Upon presentation to our facility, it was unclear if the patient presented with hematemesis or hemoptysis, thus bronchoscopy was utilized to rule out an aortobronchial lesion as a possible source of bleeding.
Despite the literature lacking a consensus surgical technique regarding AEF repair, the same general guidelines are followed. The procedure should involve debridement and explantation of the previous TEVAR stent graft, immediate management of the aortic defect, and immediate or delayed esophageal repair.4,7 Aortic repair may be performed utilizing extra-anatomic bypass grafting, or an antibiotic-soaked endoluminal graft such as used in our case. Immediate esophageal repair comprises direct suturing of the esophageal defect, often incorporating a muscle flap cover for further reinforcement. 7 Delayed esophageal repair requires diversion of the esophagus, such as the partial esophagectomy with cervical esophagostomy used to treat our patient. Despite these measures, the intraoperative and perioperative mortality rates surrounding AEF repair remain high at 40%. 7
Our case demonstrates a novel management approach in which an esophageal stent was placed as a temporizing measure 7 days prior to definitive AEF repair. The stent was placed during the interval period after the sentinel bleed but prior to a potential massive hemorrhag, thus preventing potential exsanguination by tamponading the fistula. Stenting the esophagus also provided an ample time frame for resuscitation and hemodynamic optimization of the patient prior to undergoing open repair. The use of esophageal stents in the setting of AEF following TEVAR has been reported previously, but mainly as a palliative measure for patients deemed incapable of tolerating open repair surgery.2,5,8 Our case indicates there may be a further role for esophageal stenting in AEF management. This management strategy is not without risk, however, as there is the possibility for stent migration or further vascular erosion from the friction between the endograft and esophageal stent. The stent in our case was only deployed for 7 days, which may have limited the potential for complications, but evidence from further cases utilizing this approach would be beneficial. The temporizing measure of stenting the esophagus provides adequate time to resuscitate and optimize at-risk patients prior to definitive corrective surgery in the hopes of improving morbidity and mortality outcomes (Figure 1).
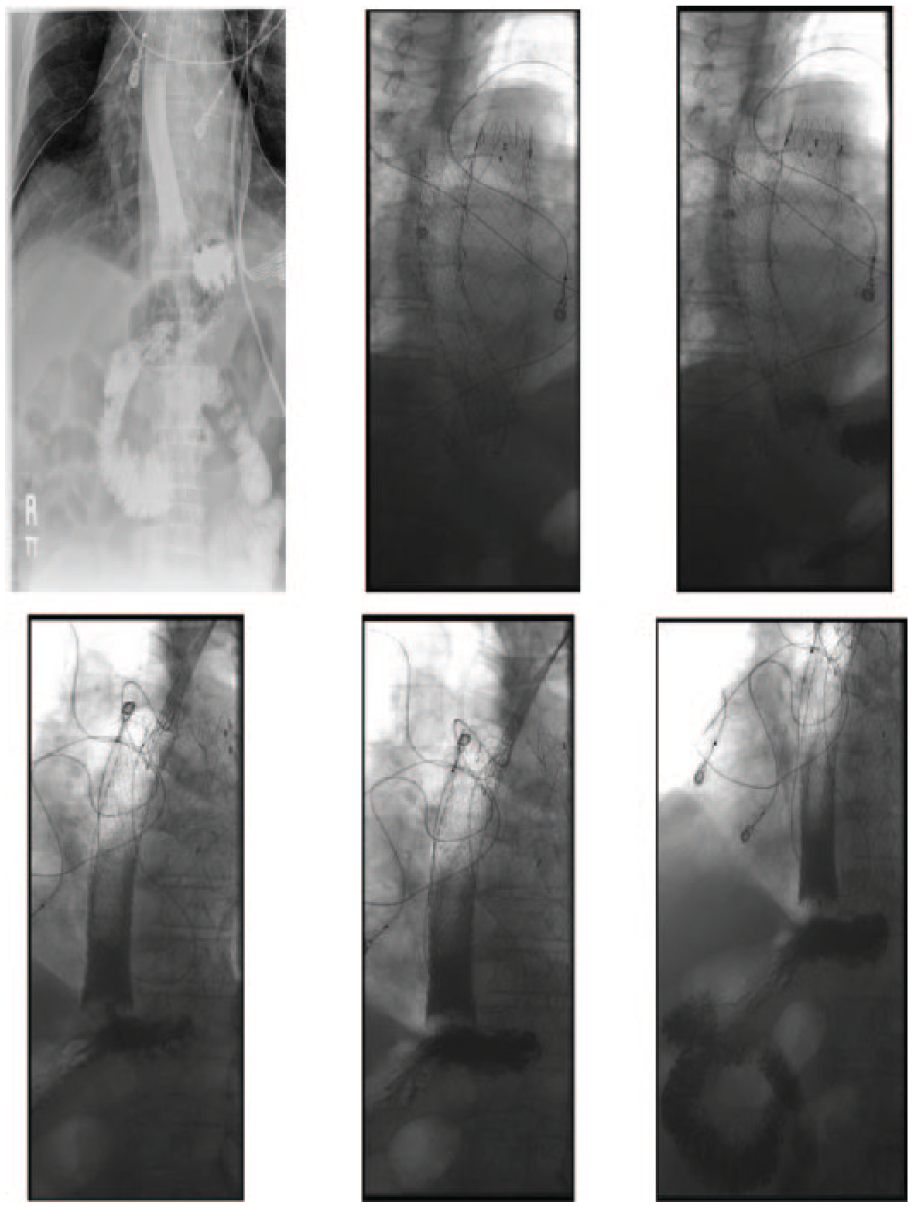
A series of images from an esophagram performed 1 day after esophageal stent deployment. The fluoroscopic images demonstrate normal peristalsis with free flow of contrast through the esophagus and esophageal stent lumen into the stomach without evidence of obstruction or stricture. There is no evidence of extraluminal contrast suggestive of leak or extrinsic compression of the esophagus or pharynx.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Conceived and designed the experiments: ES, AMJ, JJM; Analyzed the data: ES, AMJ, JJM; Wrote the first draft of the manuscript: ES, AMJ, JJM; Contributed to the writing of the manuscript: ES, AMJ, JJM; Agree with manuscript results and conclusions: ES, AMJ, JJM; Jointly developed the structure and arguments for the paper: ES, AMJ, JJM; Made critical revisions and approved final version: ES, AMJ, JJM; All authors reviewed and approved of the final manuscript.