
Abstract
We presented an unusual arrhythmogenic right ventricular cardiomyopathy (ARVC) case of a late-60s elderly man’s death, due to severe pericardial/pleural effusion and ascites, and arrhythmic events, with unique pathological features. The hypertrophic heart grossly displayed yellowish to yellow-whitish predominantly in the variably thinned wall of the dilated right ventricle. Microscopic findings showed diffuse fatty/fibrofatty replacement in not only the right but left ventricular myocardium, together with an outer lymphoplasmacytic infiltrate. According to the lipid contents analysis, the triglyceride content, but not the cholesterol content, in our patient’s right and left ventricular cardiac muscle was much higher than that in the control subject. We propose that this unique triglyceride deposition in our possibly late-onset ARVC case might be one of new clues to understand its enigmatic cause. Further prospective studies are needed to validate the presence and significance of a greater volume of triglyceride deposit, after collecting and investigating a larger number of early and late-onset ARVC cases examined.
Introduction
Arrhythmogenic right ventricular cardiomyopathy (ARVC) is a well-known genetic cardiomyopathy that most commonly affects young adults.1,2 Arrhythmogenic right ventricular cardiomyopathy is characterized by progressive replacement of ventricular cardiomyocytes with variable amounts of fatty and fibrofatty tissue, and thus, usually results in sudden cardiac death.1,2 We herein presented an unusual ARVC case of a late-60s elderly man’s death, due to severe pericardial/pleural effusion and ascites, and arrhythmic events, with unique pathological features. Especially, according to the lipid contents analysis, the triglyceride (TG) content, but not the cholesterol content, in our patient’s right and left ventricular cardiac muscle was surprisingly much higher than that in the control subject. We would like to propose that this unique TG deposition in our possibly late-onset ARVC case might be one of new clues to understand its enigmatic cause.
Case Report
The patient presented here was a late-60s elderly man, showing right ventricular cardiac hypertrophy and dilation with occasional atrial tachycardia in a background of T wave inversion and mean QRS duration ⩾ 105 ms in V1 through V3, by 12-lead electrocardiogram (ECG) recording, 6 years before his death. The clinicians diagnosed as late-onset ARVC, based on the ECG abnormalities. But, the cardiomyocytic biopsy findings from the right-sided interventricular septum showed no extracellular lipid accumulations 6 and 1½ years before his death, respectively. According to the echocardiography, left ventricular function gradually worsened over the 6 years. Neither the genetic test nor the evaluation for possible causes of infection was performed. He died due to severe pericardial effusion (1600 mL), pleural effusion (500 mL; 900 mL), huge ascites (7600 mL), and arrhythmic events, approximately 2 months after the onset of general fatigue, cardiac failure, and/or dyspnea. There was no history of essential hypertension, diabetes mellitus, dyslipidemia, malignancy, immunosuppressive disorders, or unusual infections. At autopsy, the hypertrophic and balloon-like appearing heart, weighing 477 g, grossly displayed yellowish to yellow-whitish predominantly in the dilated right ventricle (Figure 1A). On the myocardial cut surface (Figure 1B) and its scanning magnification (Figure 1C), the cross-section characteristically demonstrated a diffuse fatty/fibrofatty replacement in not only the overtly yellow-whitish and thinned right ventricular wall but also the variably thickened left ventricular myocardium. The coronary arteries displayed mild atherosclerosis with wide patency, and foci of myocardial infarction were absent (Figure 1B and C). The schema of fatty/fibrofatty replacement in the right and left ventricles was shown, partly revealing the disappearance/absence of the right ventricular myocardium (Figure 1D).
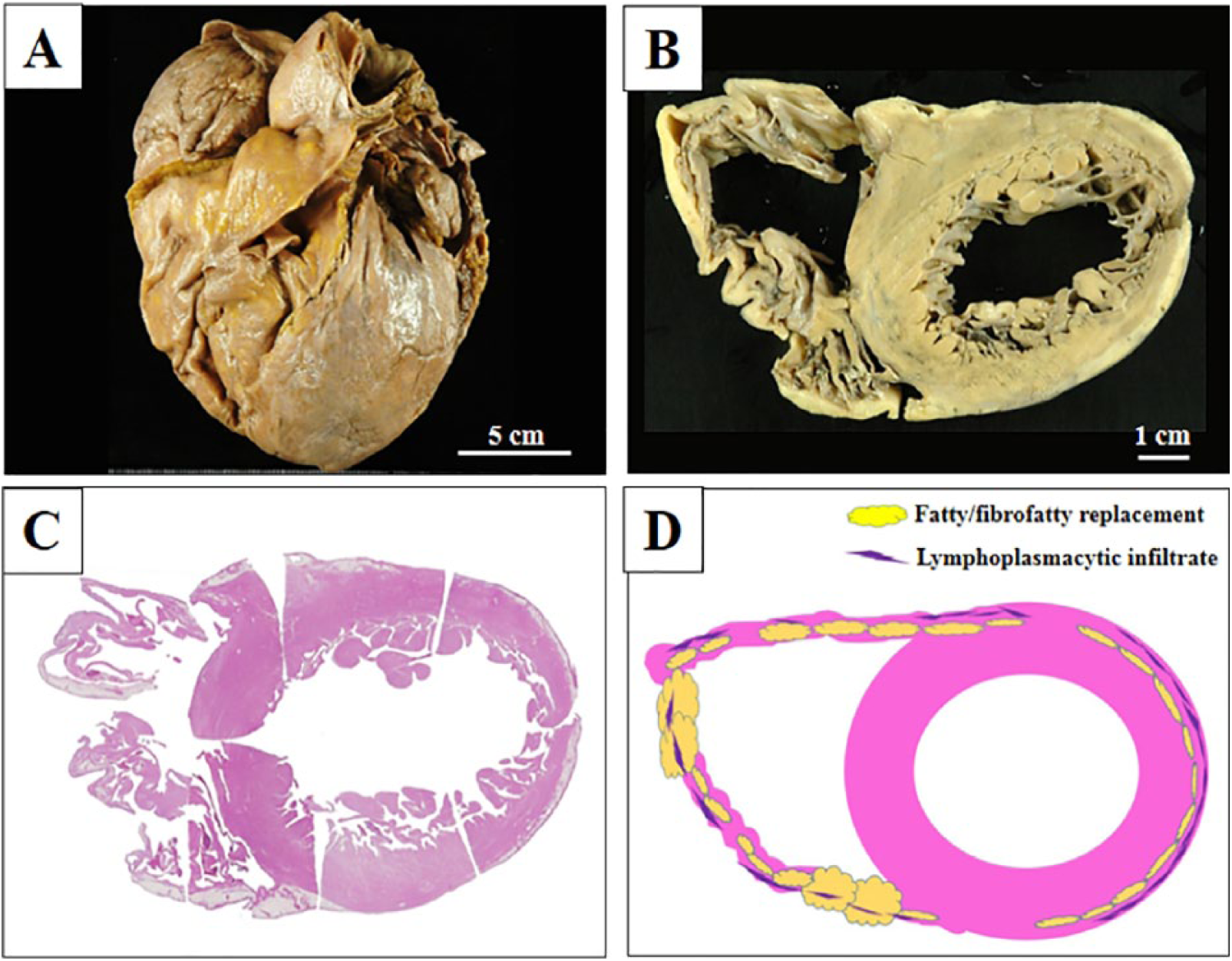
Gross examination of the heart on the present possibly late-onset ARVC. (A) On gross examination, the hypertrophic and balloon-like appearing heart shows markedly yellowish to yellow-whitish predominantly in the dilated and thinned right ventricle. Bar = 5 cm. (B) The myocardial cut surface characteristically reveals a diffuse fatty/fibrofatty replacement in not only the overtly yellow-whitish and thinned right ventricular wall but also the variably thickened left ventricular myocardium. The coronary arteries show mild atherosclerosis with wide patency, and foci of myocardial infarction are absent. Bar = 1 cm. (C) On the scanning magnification of myocardial cut surface, the cross section makes foci of the fatty/fibrofatty replacement very clear (H&E stains). (D) Correspondingly, the schema of fatty/fibrofatty replacement (yellow) with an outer lymphoplasmacytic infiltrate (purple) in the right and left ventricles is shown, partly revealing the disappearance/absence of the right ventricular myocardium. ARVC indicates arrhythmogenic right ventricular cardiomyopathy.
Microscopic findings uniquely showed a transmural fatty (Figure 2A) and fibrofatty (Figure 2B) replacement in the markedly thinned right ventricular wall, accompanied by an outer lymphoplasmacytic infiltrate (Figure 2A and C), as shown in Figure 1D. In immunohistochemistry, these infiltrating inflammatory cells were predominantly positive for CD20/CD38 (not shown). By contrast, the remnant right ventricular cardiomyocytes were overtly hypertrophic, occasionally containing bizarre nuclei (Figure 2D). Specifically, those intercalated disks immunohistochemically showed a significantly reduced expression of several desmosomal proteins, including plakoglobin (not shown). 1 Overall, these cardiac features confirmed as a final diagnosis of unusual possibly late-onset ARVC. According to the lipid contents analysis, 3 the TG content (Figure 3A), but not the total cholesterol content (Figure 3B), in our patient’s right and left ventricular cardiac muscle was much higher than that in the control subject from the recent autopsy case of a late-60s elderly man without any evidence of cardiac diseases. To examine the above cardiac muscle lipid profiles, each snap tissue of the cardiac muscle (100 mg) was homogenized and extracted with chloroform-methanol (2/1 v/v) solution, as described previously. 3 The organic phase was dried and resolubilized in 2-propanol. Then, the TG and cholesterol contents were determined using commercial assay kits (Wako Pure Chemical Co., Osaka, Japan).

Microscopic examination of the heart on the present possibly late-onset ARVC. (A) Low-power view uniquely shows a transmural fatty and fibrofatty replacement in the markedly thinned right ventricular wall, accompanied by an outer chronic inflammatory cells infiltrate. Bar = 1 mm. (B) These fibrous foci are overtly blue-stained with Masson’s trichrome staining. Bar = 500 µm. (C) On high-power view, those infiltrating inflammatory cells predominantly consists of B-lymphocytes and plasma cells. Bar = 200 µm. (D) The remnant, hypertrophic right ventricular cardiomyocytes occasionally have bizarre nuclei. Bar = 50 µm. ARVC indicates arrhythmogenic right ventricular cardiomyopathy.

Analysis of the lipid contents for the cardiac muscle from our possibly late-onset ARVC and the control subject. (A) Intriguingly, the TG content in our patient’s RV and LV cardiac muscle is 3-folds higher than that in the control subject. But, the TG contents in the cardiac muscle from the IVS show no remarkable change between our ARVC case and the control. (B) Surprisingly, the total cholesterol (Cho) contents in the cardiac muscle from RV/IVS/LV are not relatively large in volume and have no remarkable change between the current possibly late-onset ARVC case and the control subject. ARVC indicates arrhythmogenic right ventricular cardiomyopathy; IVS, interventricular septum; LV, left ventricular; RV, right ventricular; TG, triglyceride.
Discussion
It is most likely that our ARVC autopsy case is clinicopathologically remarkable for 1 reason at least: To our knowledge, we for the first time have analyzed the lipid contents on the ARVC tissue samples, and subsequently, reported confirming results regarding an increased volume of TG, but not cholesterol. The findings overlap with those of TG-deposit cardiomyovasculopathy (TGCV), a distinct entity, whose primary is genetic mutations in adipose TG lipase, an essential molecule for hydrolysis of intracellular TG. 4 We propose that this unique TG deposition in our possibly late-onset ARVC case might be one of new clues to understand its enigmatic cause. However, the cause of TGCV could be very different from that of ARVC.1,4 In fact, unlike TGCV, approximately 40% of patients with ARVC have shown mutations in genes encoding desmosomal proteins, such as plakoglobin, desmoplakin, plakophilin 2, desmocollin 2, or desmoglein 2. 1 Furthermore, in marked contrast to ARVC, TGCV with adipose TG lipase-mutations/deficiency is characterized by profound intracellular, but not extracellular, TG deposition in multiple tissues, including cardiomyocytes or smooth muscle cells. 4 Despite that, Hirano et al 5 have more recently reported that the medium-chain TG (ie, tricaprin) diet may be beneficial on the treatments for the TGCV patients, based on a growing body of data from adipose TG lipase-knockout mice models. Nevertheless, it would be intriguing to assess the significance of lipid analysis for the ARVC management on future studies, after collecting and investigating a larger number of early and late-onset ARVC cases examined. This short case report could interest the scientific community, taken together with potentially specific, new findings of ARVC.
Footnotes
Acknowledgements
This article is based on the Presentation at the 107th annual meeting of The Japanese Society of Pathology, in 2018, and its presenter Kentaro Yamamoto, first author of this article, has received the Young Medical Student’s Award, The Japanese Society of Pathology, for his presentation. We would like to thank Dr Hironobu Akao, PhD, Department of Cardiology, Kanazawa Medical University, Ishikawa, Japan, for his helpful comments, and thank Mrs Yuka Hiramatsu and Mrs Chikako Yonenaga for their expert technical assistance.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/ or publication of this article: This work was partly supported by a grant from the Kanazawa Medical University Fund, Ishikawa, Japan (to SY).
Declaration of conflicting interest:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
SY and KY participated in conception of the idea and writing of the manuscript. SY, KY, XG, KM, NK, MK, AS, SN, TT, YI, HA, and KK performed the clinical investigation and pathological/immunohistochemical interpretation of this unusual ARVC. All authors have read and approved the final manuscript.
Availability of Data and Materials
The dataset supporting the findings and conclusions of this case report is included within the article.
Informed Consent
Written informed consent was obtained from the patient and his family on admission for the publication of this case report and any accompanying images.