
Abstract
Objectives:
Amyloidosis is a group of rare diseases that often manifest in multi-organ symptoms requiring an effective multidisciplinary team of care providers to manage. This study aimed to identify the best practices and key barriers to patient-centric care at US specialized amyloidosis centers (SACs) which have emerged as central hubs for multidisciplinary amyloidosis care.
Methods:
We conducted and analyzed interviews with 77 stakeholders of amyloidosis diseases, including specialist physicians from 17 SACs across the US, patients, patient advocacy group representatives, and referring physicians.
Results:
The most commonly mentioned best practices were patient-centric multidisciplinary care, timely intake of new high-risk patients, and responsiveness to patient questions. Expanding local physician education was noted as critical to earlier diagnosis. Fifteen out of 17 SACs are actively involved in clinical trials for amyloidosis treatments. Key barriers to care identified were patient distance to SACs, limited medical records and data sharing, and insurance hurdles. Most SACs keep track of metrics, such as patient volume, patient demographics, time to first appointment, as part of internal or in external registries to measure progress.
Conclusion:
These findings offer practical insights for optimizing amyloidosis care and highlight the structural and informational gaps that must be addressed to improve access and outcomes.
Plain Language Summary
Current State of Care for People With Amyloidosis at Specialized U.S. Centers: What Works and What We Need to Improve
Why was this study done?
Amyloidosis is a rare disease that can affect several organs in the body. Because it is complex and not well-known, people with amyloidosis often have challenges getting the right diagnosis and care. In recent years, specialized amyloidosis centers (SACs) have been set up across the United States by hospitals to provide appropriate care to these patients. This study aimed to understand how these centers work, what they do well, and what challenges they face.
What did the researchers do?
The research team spoke with 77 people across the U.S., including doctors, nurses, patients, referring physicians, and leaders of patient advocacy groups. All participants were involved in amyloidosis care. The interviews explored how SACs provide care, how patients access services, and what could be improved.
What did the research find?
Participants described several best practices at SACs, such as coordinated care by teams of different specialists, fast intake for high-risk patients, and strong communication with patients. Most SACs also track data on patients and many are involved in clinical trials. Patients valued the compassion and responsiveness of SAC staff.
However, some challenges remain. Patients and doctors still see a lot of delays in diagnosis. Travel distance to centers, insurance barriers, and limited emotional support were common issues. Many patients said they received little information at the time of diagnosis. Telemedicine was helpful for some but not ideal for all situations.
What do these findings mean?
This study shows that SACs offer many benefits for people with amyloidosis, but improvements are still needed–especially in education, emotional support, and coordination with local care providers. The researchers and participants hope that by sharing their perspectives, newer SACs and doctors, as well as patients, can be better informed about providing and receiving care that centers the patient experience.
Keywords
Introduction
Amyloidosis is a group of rare diseases characterized by the progressive deposition of misfolded proteins leading to organ dysfunction. Though prognosis vary by type of amyloidosis, recent therapeutic advancements have improved the care of more common types such as immunoglobulin light chain amyloidosis (AL) and transthyretin amyloidosis (ATTR). 1 Delays in diagnosis and access to treatment remain, often due to limited healthcare provider (HCP) awareness, missed diagnosis, inadequate screening, and nonspecific early symptoms.2-6
Amyloidosis can affect various tissues and organs, including the heart, kidneys, liver, nervous system, and gastrointestinal tract, among others. Due to the range of manifestations, a multidisciplinary and specialized care approach is essential for diagnosis, timely treatment initiation, comprehensive symptom management and optimization of patient outcomes. 7 Structured organization of patient care activities, care coordination, timely and appropriate delivery of services and interdisciplinary collaboration are key components of optimal amyloidosis patient management.8-13
An increasing number of specialized amyloidosis centers (SACs) have been established across the United States (US) for this cause. These dedicated centers often employ a multidisciplinary approach with key care providers with expertise in diagnosing, managing, and supporting patients with amyloidosis. 8 As awareness of amyloid diseases grows and more SACs emerge, sharing best practices and strategies to address key barriers is important to standardize amyloidosis care and ensure patients receive optimal care nationwide.
With the mission to improve patient-centric care and encourage knowledge-sharing, this working group aimed to assess the best practices, identify key barriers and explore opportunities for improvement for patient-centric care at US SACs. A qualitative approach was used to explore diverse stakeholder perspectives involved in amyloidosis care to gather comprehensive insights from multidisciplinary healthcare providers, patients, and patient advocacy groups nationwide.
Methods
Study Design and Rationale
A qualitative design was selected to explore stakeholder perspectives and real-world care experiences across SACs. Guided by a constructivist paradigm that acknowledges the complexity of amyloidosis care delivery, a semi-structured interview guide was used to elicit contextual, lived insights from healthcare providers, patients, and patient advocacy group representatives to understand the current state of amyloidosis care from diverse perspectives. While this study is not a formal phenomenological analysis, analytic attention was given to participants’ description of their lived experiences with amyloidosis care. A codebook-based thematic analysis supported identification of common and recurring patterns across key themes.
Inclusion and Exclusion Criteria, and Participant Selection
A purposive sampling strategy was used to select 17 US SACs for a diverse snapshot of amyloidosis care. First, a list of nationwide SACs was drafted through publicly available information and input from the ARC-ASPIRE working group given the lack of a standardized registry of SACs. SACs were then assessed for their geographic location, patient volume, years of operation, and disease types treated. These attributes informed selection of SACs to ensure representation across regions, center size and years of operation, helped mitigate potential selection biases, and avoid potential overrepresentation of insights from any single type of SAC.
Within each SAC, participants were purposively selected to ensure representation across clinical specialties and care roles. Healthcare providers (physicians, advanced practice providers [APPs], and registered nurses [RNs]) were eligible for inclusion if they were aged ⩾18 years and directly managed or supported the management of patients with ATTR and/or light chain amyloidosis.
Patients were eligible for inclusion if they were aged ⩾18 years, had a confirmed diagnosis of ATTR or light chain amyloidosis, and were receiving care at a specialized amyloidosis center in the US. Patients were recruited on a first-come, first-served basis to meet predefined recruitment targets across amyloidosis type and geographic regions, using recruitment postings on patient forums hosted by ARC and AF Amyloidosis Foundation (AF).
Additionally, representatives from patient advocacy groups were identified and invited to participate in this study. All participants were excluded if they did not meet the above eligibility criteria or were unable to provide informed consent to participate in an interview.
Sampling continued until data saturation was reached within each stakeholder type, defined as the point when successive interviews no longer yielded substantively new themes and responses demonstrated internal consistency.
Interviews were conducted by third-party healthcare consultants experienced in qualitative interviewing. All interviews took place via teleconference between December 2023 and February 2024, lasting approximately 60 minutes. Interviews were audio-recorded when consent was given and transcribed verbatim. A semi-structured guide—tailored by participant type—was used to explore care models, the patient journey, diagnostic pathways, treatment delivery, and access barriers. The guide was designed for flexibility and was not formally pilot-tested. Full discussion guides are available as part of supplementary information. Details of this qualitative research as outlined by the consolidated criteria for reporting qualitative research (COREQ) and research instruments used are available in the supplementary information. 14
Researcher Reflexivity
The interviewer had no prior relationship with participants and held no preconceived assumptions about the research topic. As a third-party researcher external to ARC-ASPIRE and the authors, the interviewer’s position likely supported open disclosure by participants. Participants were informed that the study was being conducted on behalf of ARC-ASPIRE.
Data Analysis and Rigor
A structured codebook was developed based on the interview guides, study objectives, and key thematic concepts, and was iteratively refined as new insights emerged from the interviews. Verbatim interview transcripts and detailed notes were coded into Microsoft Excel, with coding into a shared codebook conducted by 3 independent coders, including the primary interviewer, and reviewed with among the research team through regular debriefings to ensure analytic consistency and consensus on discrepancies. Anonymized recordings, verbatim transcripts, and detailed notes supported trustworthiness and transparent interpretation of the findings, and regular debriefings among the research team and authors helped minimize biases.
Ethical Considerations
Ethical approval was obtained from the North Star Review Board in December 2023 (Protocol NB300162). All participants gave informed consent verbally and in writing. Participation was voluntary, and confidentiality was maintained throughout. No identifying details are included in the analysis, and participants consented to the open publication of aggregated, de-identified findings.
Results
The final research sample included 77 participants with diverse representation among HCPs and patients in terms of geography, types of amyloidosis managed, and years since establishment or diagnosis (Table 1). The sample also included referring physicians and representatives from 3 US-based amyloidosis PAGs who were able to provide aggregate perspectives from working closely with patients.
Attributes of Study Participants.
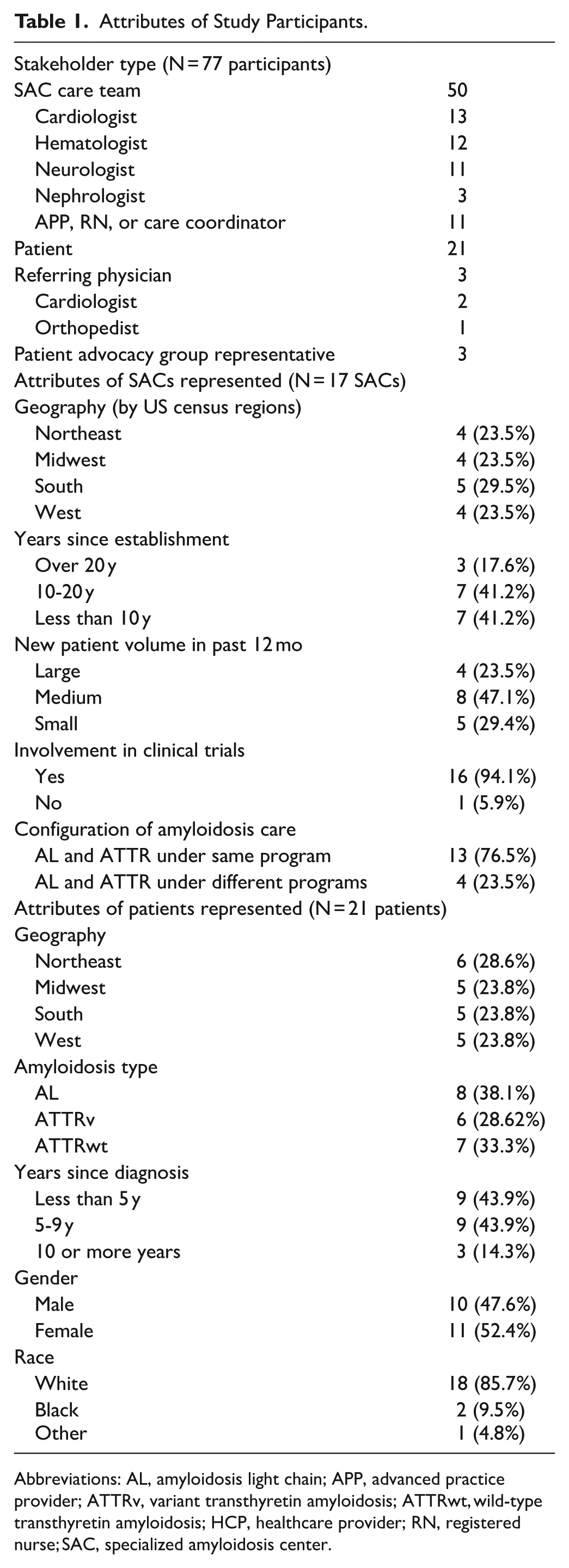
Abbreviations: AL, amyloidosis light chain; APP, advanced practice provider; ATTRv, variant transthyretin amyloidosis; ATTRwt, wild-type transthyretin amyloidosis; HCP, healthcare provider; RN, registered nurse; SAC, specialized amyloidosis center.
Best Practices
Multidisciplinary Care Coordination
Amyloidosis patient care requires strategic alignment across multidisciplinary team members including cardiologists, neurologists, hematologists-oncologists, APPs, care coordinators, and research staff (Figure 1). Genetic counselors assist with family testing and education for ATTRv; most SACs utilize institutional counselors though one SAC outsourced due to internal delays. All care providers lauded the multidisciplinary nature of their SACs to deliver comprehensive care addressing multi-organ amyloidosis manifestations, with one APP stating “it’s a multi-organ disease so you need to have a multidisciplinary team. . . . Unless you sit in a room with a bunch of different specialists, you’re never going to understand how this disease affects every single organ.”

Common components of a specialized amyloidosis center.
Among SACs in this research, more tenured SACs (ie, established for longer than 20 years) typically had larger teams (17 vs 13 HCPs on average) compared to newer SACs (ie, established for less than 10 years) with closer involvement of specialties such as nephrology, pathology, gastroenterology, and endocrinology. Furthermore, more tenured SACs were more likely to have dedicated care coordinators compared to newer SACs (40% vs 10%).
SACs enhance teamwork through multiple avenues. All SAC HCPs engaged in real-time communication. Most SACs (76%) have unified amyloidosis care under a single department, typically within hematology (47%) or cardiology (38%). If separate, AL and ATTR are managed under hematology and cardiology respectively. Most SACs (82%) have regular meetings to discuss new patients and patients with complications. Nearly half (47%) have dedicated clinic days to facilitate patient-centric scheduling that minimizes patient travel and improves team communication. Among those, 2 SACs offer a single clinic location for amyloidosis patient care which can greatly improve patient care coordination and communication with one neurologist noting “the nice thing about our program is that we all reside in the same area. We have an amyloid day. . . in the same clinic space. We try to make it easy for patients, because a lot of our patients come from far away. All testing is done on the same day and then patients see all the pertinent clinicians in the same place. This is ideal. Things get lost on an email chain. But if you’re in the same space, it’s really easy to discuss cases.”
Centralized System for Referrals and Patient Intake
HCPs report that the majority of SAC referrals come from HCPs (77%), while some (23%) are self-referred by patients (Figure 2). Cardiologists tend to be the most frequent referrers, followed by neurologists. Patient perspectives align, as 19% of patients had self-referred to SACs based on online search portals and amyloidosis PAG resources. Patients report cardiologists were most likely to refer for ATTRv and ATTRwt, while AL referrals are distributed across various specialties.

Referral patterns to SACs: (A) referral patterns reported by SAC HCPs and (B) referral patterns reported by patients.
Most (59%) SACs have a centralized intake system–such as a single person or group of people dedicated to managing and reviewing referrals, paperwork, and additional testing for new patients—to prioritize high-risk cases. Such high-risk cases include suspected AL patients, given the faster disease progression, who are seen on average within 1 week across SACs. This centralized intake system was viewed as integral to SACs who have them with one neurologist describing the nurse coordinator running the centralized intake at their SAC as “our jack of all trades. . . as the point of contact for all amyloidosis patients, she coordinates everything.”
Active Education and Outreach
SAC HCPs are engaged in educational initiatives to raise amyloidosis awareness. Institutionally, they conduct grand rounds while externally, they routinely educate referrers on methods to improve diagnostic accuracy, common drug-drug interactions and contraindicated treatments. All HCPs frequently attend amyloid conferences with 6 out of 17 SACs also hosting their own regional conferences. Tenured HCPs also frequently consult with less experienced HCPs to share guidance and expertise, with one cardiologist at a tenured SAC sharing “the hard part [of amyloidosis care] is that people just do not understand the nuances and there is misinformation out there. . . . Even if less frequent, [monitoring] should be done by amyloidosis experts at a specialized center.”
HCPs are committed to coordinated care with regional providers to support care more local to the patient. Half of HCPs currently co-manage most of their amyloidosis patients through such coordinated efforts, with more tenured HCPs more likely to do so. Within co-management, SAC HCPs tend to manage the diagnostic workup, treatment recommendations, and proactive communication of medical records. Of note, some newer SACs regularly invite regional HCPs to SAC journal clubs and multidisciplinary meetings to improve amyloidosis awareness and foster better co-management relationships.
Use of Metrics
Most SACs track metrics to measure the success of amyloidosis care such as patient volume (9 SACs), internal registries (8 SACs), participation in external registries (7 SACs), survival rate (8 SACs), patient demographics (3 SACs), time to first appointment (3 SACs), referral volume (3 SACs), and functional status (3 SACs). 4 out of 17 SACs do not track any metrics due to limited resource. 15 out of 17 SACs offer clinical trials for amyloidosis.
Patient and PAG Perspectives on Best Practices
Patients frequently identified care team responsiveness as a best practice, linking it to care quality and their own sense of reassurance. Most (95%) used online patient portals for communication with SAC teams. Compassion and expertise were also highly valued, particularly at tenured SACs. Longer appointments (1 hour) were appreciated for reviewing test results and addressing concerns. Patients also benefited from SAC and specialty pharmacy support in navigating insurance prior authorizations for access to treatment.
Patients at tenured SACs reported higher satisfaction with continuity of care, especially when coordinated with local physicians. Regional differences were noted, with Midwest patients reporting higher satisfaction rates (80% vs 60%-70% in other regions). Timely referrals to specialists were highlighted as another best practice, with tenured SACs referring more patients (33% vs 20% at newer centers). Common referrals included gastroenterologists, nephrologists, orthopedists, and physical therapists.
Patients and PAG representatives emphasized critical factors for recommending SACs: multidisciplinary expertise, seamless patient navigation (ie, clear contact information, intake coordinator, or dedicated clinic), insurance assistance, co-management with local providers, and psychological support, especially for ATTRv cases requiring family testing. Referring HCP recommendations and PAG directories also influenced SAC selection.
Barriers to Care
Key Challenges Experienced by HCPs
HCP participants consistently identified delayed diagnosis as a primary barrier to optimal care, stemming from low local awareness and insufficient familiarity with diagnostic algorithms. One neurologist notes “I think [a key challenge] is to expedite diagnosis, because people are diagnosed years after symptom onset. So, education is needed so first touch providers recognize these symptoms to lead to an accurate diagnosis.”
HCP participants also viewed patients’ access to SACs as a challenging barrier, as geographic distance and associated travel pose physical and economic burdens for patients. SACs are also concerned that high out-of-pocket treatment costs and insurance hurdles contribute to patient hesitancy to pursue treatment.
HCP participants also reported that limited and inconsistent medical record sharing between SACs and patients’ local providers, compounded by sparse communication and differing electronic medical record (EMR) systems, often hindered effective co-management. Additionally, they note some institutional reluctance to share aggregate patient data is limiting cross-SAC collaboration and research opportunities.
Key Challenges Experienced by Patients
Delayed diagnosis was the most frequently cited barrier mentioned by patients, with 81% having consulted multiple specialists before amyloidosis was suspected. One PAG representative observed “all patients have had the unfortunate situation of having physicians be unaware about the disease. Most have seen multiple specialists before a diagnosis. . . the physicians can be highly regarded, reputable, but they hadn’t run into patients with this disease.” As such, two-thirds of patient participants had seen 3 or more HCPs before encountering one knowledgeable enough to make a referral, delaying initiation of disease modifying treatment.
Over half (68%) of the patients perceived their initial education on amyloidosis to be insufficient, particularly if being managed at newer SACs (80%) compared to tenured centers (50%). Patients would have appreciated timely referrals to PAGs at diagnosis, additional time dedicated to education, more frequent educational sessions throughout the patient journey, and more information on available clinical trials. Throughout their patient journey, patients were most likely to reference educational materials developed by PAGs such as patient booklets and online webinars from ARC. Patients also appreciated support group meetings led by their SACs (available at 5 out of 17 SACs interviewed) or Amyloidosis Support Groups (ASG).
Insurance hurdles delayed treatment for nearly half of patients, with 80% in western regions facing coverage barriers. Travel to SACs posed logistical and financial challenges, such as missed work and symptom exacerbation, for nearly half of patients. Lastly, the need for additional emotional support was flagged by a third of patients with many expressing a desire for more psychosocial support for themselves and their caregivers. In particular, they point to the value of connecting with other amyloidosis patients for shared experiences.
State of Telemedicine in Amyloidosis Care
HCP participants noted that although telehealth was crucial during the COVID-19 pandemic, post-pandemic regulatory changes complicate its continued use, particularly due to in-state medical licensing requirements for telemedicine. While 85% of HCPs at SACs still incorporate telehealth into amyloidosis care, HCPs hold mixed views on the value of telemedicine (Figure 3).

Perception of value of telehealth in amyloidosis care by SAC HCPs: (A) summary of telehealth perceptions among HCP participants and (B) distribution of telehealth perceptions by HCP type.
Enthusiasts (29%) see telemedicine as particularly well-suited for rare diseases like amyloidosis where specialized care often requires significant travel. They often adopt measures such as obtaining multiple state licenses and alternating virtual and in-person visits, emphasizing the value of patient convenience and more frequent check-ins. One hematologist shared “I think telemedicine is a great way to make treatment more convenient and accessible for patients. It’s not uncommon for patients to have well over an hour drive to reach our center, the parking is also a separate expense for patients. I’ve embraced telemedicine because I think it is so much better for the patient.”
Moderates (39%) support telemedicine for stable patients but stress telemedicine cannot replace in-person visits. Additionally, they perceive the logistical and legal restrictions to diminish the continued feasibility and overall value of telemedicine. Skeptics (33%) highlight the complexities of managing amyloidosis virtually. Neurologists, whose routine evaluations require sensory assessments, being most likely to be skeptics with one saying, “I’ve tried all pandemic long, but most of what I do in exams is hands on.” Some also note the technological barriers and peripheral time burdens that reduce telemedicine’s net value, particularly when managing older patients.
Patients also expressed mixed views on telemedicine. While a third of patients view telemedicine positively given its ability to reduce travel burden, some (19%) reported negative experiences such as perceived insufficient HCP engagement during virtual visits. Nearly half (48%) were neutral, and view telemedicine as suitable alternative in certain situations such as follow-up visits or non-urgent questions. Patients who viewed telemedicine positively often appreciated the intentional efforts of their SAC HCPs to coordinate co-management of local physicians, improving the efficiency and effectiveness of their virtual appointments.
Discussion
Historically, SACs were limited in number and location, leading to disparities in amyloidosis care across the US. Recently, more institutions have recognized the value of multidisciplinary SACs, driven by increased awareness, improved diagnostic capabilities, and new therapeutic options. Although some variation in patient experience was observed across regions in this study, the growing number and broader distribution of SACs may have improved geographic access to multidisciplinary amyloidosis care nationwide and reduced travel burden for patients over the years. Encouragingly, most SACs actively participate in clinical trials, offering novel treatment options. As SACs expand, fostering communication, mentorship and collaboration between established and newer centers remains vital to reducing disparities and enhancing care quality.
Multidisciplinary Expert Care
Our findings align with previous studies, which also emphasized the importance of multidisciplinary care in amyloidosis management (Supplemental Figure 1).8-15 Our findings suggest that the breadth of multidisciplinary care co-evolves with program maturity, as more tenured SACs tended to have larger care teams and greater representation across specialties to better enable the more comprehensive management of the multi-organ manifestations of amyloidosis.
Though the SACs surveyed likely differ, it is promising to observe the rise in prevalence of multidisciplinary meetings in the US from Nativi et al 8 to this study. Cheng et al 15 ., which had an expanded scope of both US and international centers, reported a lower prevalence of multidisciplinary meetings which may indicate differences in approach in care between the US and globally. Importantly, participants in our study described these meetings not just as logistical functions but as critical spaces for clinical decision-making, shared learning, and holistic patient planning—highlighting their embedded value in the lived experience of care delivery.
Centralized Intake and Triaging System
Our findings, consistent with those of Cheng et al 15 ., identify centralized intake systems as a crucial best practice in effectively managing patient flow and ensuring timely evaluation of high-risk patients. In this study, 59% of the participating SACs had implemented such system, primarily managed by APPs or SAC directors. SACs without a centralized intake system cited organizational inertia as the main barrier but acknowledged their growing importance as referral volumes rise.
It is particularly notable that more tenured SACs were more likely to have dedicated care coordinators who support centralized intake and coordination across multiple specialties and providers. Providers from these more established SACs emphasized that centralized processes helped relieve administrative burdens, prioritize urgent cases, review prior medical records, and ensure needed testing was completed in advance. They also facilitated tracking of key metrics, such as referral sources and time to appointment, which enabled performance improvement and impact measurement over time.
Metrics
SACs note that tracking metrics has been instrumental in demonstrating the value of their programs and enabling long-term tracking of patients over time. Patient registries, in particular, helped reveal key institutional and clinical trends. However, maintaining data systems for metrics tracking is resource-intensive and nearly a quarter of SACs lack the means to do so, emphasizing the need for institutional support to enhance metric tracking capabilities.
Barriers to Care
Barriers to care identified by HCPs were delayed diagnosis, patient financial burdens, telehealth restrictions, and limited data sharing. Patients echoed these concerns and added challenges such as inadequate initial education, challenges with insurance coverage, travel burden, and emotional support needs.
Delayed diagnosis remains a particularly consequential barrier with implications for both clinical outcomes and patient experience. In addition to raising greater awareness of amyloidosis diseases among HCPs outside of SACs, integration of systemic diagnostic approaches—such as genetic screening for family members of patients diagnosed with ATTRv and the use of advanced echocardiographic techniques, including speckle tracking—may help support earlier diagnosis and more timely initiation of treatment.16-18
Divergent perspectives on the role of telemedicine in amyloidosis care were observed in this study and likely reflect the evolving regulatory and clinical approaches of care delivery in the US. Most providers and patients noted that virtual visits occurred less frequently than in-person appointments in the post-pandemic period, driven in part by patient or provider preference as well as limitations related to cross-state licensure. At the same time, greater familiarity with virtual care persists, with patient-SAC communications and remote follow-up appointments becoming a more common component of amyloidosis management. Compared with the more uniformly positive views on telemedicine reported by Cheng et al (2024), which was based on data collected earlier in the pandemic period (2021), the mixed perspectives observed in this study likely reflects the shifting and cementing role of telemedicine post-pandemic. 15 Taken together, these findings suggest that telemedicine is a complementary tool that can support communication and follow-up care in select contexts, particularly for patients based in remote areas with limited access to local specialized care.
Educational and Supportive Resources
In order to better support patients, particularly with initial and ongoing education about their disease, HCPs may benefit from proactively leveraging existing resources from amyloidosis PAGs. Examples include MyAmyloidosisPathfinder.org offered by ARC to support those searching for SACs and clinical trials and free educational resources developed by ARC, ASG, Amyloidosis Foundation, oneAMYLOIDOSISvoice, professional societies—such as the American College of Cardiology (ACC), American Heart Association (AHA), American Society of Nuclear Cardiology (ASNC), the American Association of Heart Failure Nurses (AAHFN), Heart Failure Society of America (HFSA)—amyloidosis treatment manufacturers, as well as those from SACs themselves.
Beyond education, PAGs often provide practical support by helping patients locate nearby SACs, navigate insurance processes, and foster invaluable emotional peer support through connecting patients through online or in-person support groups meetings, hosted by PAGs or their SACs. Other supportive services for amyloidosis patients include telemedicine for renewing treatment plans for stable patients, coordination of home-based rehabilitation services and medication delivery, which may alleviate travel-related burden for patients. Tenured and newer SACs alike should be aware of the breadth of educational and supportive resources available, and the authors highly suggest proactively recommending these resources to patients.
SACs play a pivotal role in delivering multidisciplinary care, supporting early diagnosis and comprehensive management of patients living with amyloidosis. The findings of this study highlight several practice-relevant considerations for the ongoing development and optimization of SACs. Participants—providers and patients alike—underscore the importance of multidisciplinary team structures as well as dedicated care coordinators who can support centralized intake, triage of patients based on risk, and coordination of appointments. Where possible, having dedicated space and days for amyloidosis patient care can support patient-centric care and encourage multidisciplinary communication. Telemedicine can be an effective tool for ongoing management while relieving patient travel burden for stable patients. Proactive integration of resources developed by PAGs may help address persistent patient barriers related to patient education and psychosocial support. We hope that the collective best practices highlighted in this study serve as valuable insights for both SAC and non-SAC specialists, reinforcing the importance of comprehensive, patient-centric approach to amyloidosis care.
Limitations
There were several limitations to this study to consider. As qualitative researchers working within a constructivist paradigm, we recognize that our findings reflect co-constructed insights drawn from the unique perspectives of patients, providers, and advocates at a particular moment in time. Selection of participating SACs was deliberately geared to include a representative snapshot of current amyloidosis care in the US based on geographic location, patient volume, and years of experience. SACs were selected independent of their consideration as a “Center of Excellence,” a non-standardized term identifying institutions providing state-of-the-art amyloidosis care. Thus, it is likely that some nuances and variations were not documented as not all US SACs are represented in the findings.
Similarly, the identification of SACs was challenging due to the lack of a centralized list of all US SACs and the evolving landscape of amyloidosis care; it is possible that lesser-known SACs delivering amyloidosis care with less conventional structures were not included for consideration. The first-come, first-served logistics of patient recruitment through patient forums as well as the demographic composition of the patient sample— predominantly White and female—also limits the generalizability of patient experiences, particularly for individuals from underrepresented racial and ethnic groups or those with more limited access to PAG resources.
Given the involvement of industry funding and authors affiliated with companies active in amyloidosis therapeutics, steps were taken to minimize bias and support the integrity of the study design and findings. Interviews were conducted by an independent third-party research team with no prior relationships with participants, using semi-structured guides. Codebook-based thematic data analysis with regular debriefings with the broader author team also ensured analytic consistency and interpretation.
To enhance the comprehensiveness of this research, several avenues of further research warrant exploration. Expanding this study to include a broader range of specialists could provide a more nuanced understanding of care dynamics. Engaging with a larger sample of referring physicians would offer valuable insights into care coordination processes. Lastly, a quantitative evaluation of key patient-centric metrics could provide a trackable and goal-oriented view into the evolution of amyloidosis care. These steps could contribute to a more thorough evaluation of the care landscape and identify potential areas for improvement.
Supplemental Material
sj-docx-1-cic-10.1177_11795468261444669 – Supplemental material for Best Practices and Key Barriers for Amyloidosis Patient Care at US Specialized Amyloidosis Centers: An Analysis by ARC-ASPIRE
Supplemental material, sj-docx-1-cic-10.1177_11795468261444669 for Best Practices and Key Barriers for Amyloidosis Patient Care at US Specialized Amyloidosis Centers: An Analysis by ARC-ASPIRE by Jose Nativi-Nicolau, Johana Fajardo, Alyssa Galloway, Sami Khella, Nisith Kumar, Michaela Liedtke, Isabelle Lousada, Tiffany Patrick, Colleen Moffitt, Lori Klein, Gabriela Tamariz, Karthikeyan Veeraraghavalu and Alexandra Haddad-Angulo in Clinical Medicine Insights: Cardiology
Footnotes
Acknowledgements
The authors would like to thank all participants in this research. Data collection, analysis and medical writing support was provided by Hyein Grace Lee, PhD, CMPP of Putnam Associates, MA.
Ethical Considerations
This study has been approved by an independent review board, North Star Review Board, on December 2023.
Consent to Participate
Participants gave informed consent, both in writing and verbally, before interviews.
Consent for Publication
Participants consented to the open publication of aggregated, blinded analysis of the interviews resulting from this study.
Author Contributions
The authors confirm contribution to this publication as follows: study conception, design, analysis and interpretation: JNN, JF, AG, SK, NK, ML, IL, TP, CM, LK, GT, KV, AHA. Manuscript preparation: AG, CM, LK, AHA. All authors reviewed the manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KV, employee of Prothena Bioscience, Inc, and stockholder in Prothena Corporation plc.; AHA, employee of Pfizer and holder of Pfizer stock / stock options; AG, employee of BridgeBio; NK, employee of Pfizer and holder of Pfizer stock / stock options; TP, employee of Alnylam at the time of study and is an Alnylam stockholder; CM, employee of Alnylam and holder of Alnylam stock; GT, employee of Alnylam. SK, consultant for Ionis, Alnylam, Pfizer, BridgeBio, and Alexion; JNN, clinical trials with Alnylam, Alexion, and Intellia; ML, consultant for AbbVie, Adaptive Biotechnologies Corporation, BMS, GSK, Janssen, Kite Pharma, Natera, Nexcella, and Takeda Oncology.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The ASPIRE Coordinated Care Working Group is supported by Alnylam, BridgeBio, Pfizer and Prothena. The Amyloidosis Stakeholder Partnerships for Impact, Reach & Equity (ASPIRE), facilitated by the Amyloidosis Research Consortium (ARC), brings together biotech and pharmaceutical companies with the shared goal of optimizing amyloidosis patient care.
Data Availability Statement
Due to the nature of this research and participant consent, individual data is not available for sharing. Aggregate analysis of data is available from the corresponding author upon reasonable request*.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.